
Abstract
Rectal malignant melanomas (RMM) are remarkably uncommon, the rectal location represents less than one percent of all rectal cancer. Because of its low global survival rate, the surgical strategy is a subject of controversy for attaining a r0 resection. the palliative treatment is also debateable, but recently; radiotherapy and immunotherapy became the preferred treatment and offer the best outcome. to ensure r0 resection, abdominoperineal resection (apr) is considered the main surgical option, but because of its morbidity and functional limitations, local excision techniques such as endoscopic mucosal resection (emr) combined with chemoradiotherapy are being increasingly performed to preserve the quality of life and reduce local recurrence rate. In this report, we evaluate the place that apr still keeps as surgical procedure in comparison to partial excision. we report a case of a 72 years old patient, who presented rectal syndrome with rectorrhagia for 2 months, the diagnosis of localized rectal melanoma was confirmed by endoscopy, magnetic resonance imaging, histological analysis tissue with immunohistochemistry. the procedure strategy was a surgical treatment with apr. After a long recurrence-free survival period, the patient develops local recurrence and immunotherapy-resistant metastasis.
Keywords
Introduction
Malignant melanomas are formed from the pigment system. The rectal location is fairly uncommon. The typical total survival rate is very low and the median recurrence-free survival is 9 months, 1 all patients die because of metastases. There is a minor female preponderance. It develops at all age categories with the maximum frequency starting the 6th decade. 2
Melanocytes are in general absent in the rectum. However, both the presence of metaplasia's sites with melanocytes and the submucosal shift of a lesion initially formed in the anal canal can possibly explain the rare occurrence at rectal level. 3
RMM's symptoms are insufficient and indefinite. Frequently, they appear at late stage and mistakenly linked to benign anorectal disorders, such as bleeding or a mass, which is to blame for the misdiagnosis of RMM. Most patients presented an associated nodal metastasis at diagnosis. Very few patients are diagnosed by chance during a screening test. 4 If the RMM is mistaken for haemorrhoids, the 1-year survival rate drops to only 29% and the average survival to only 6.0 months. 5
Typically, this tumour takes a polypoid and ulcerative form, sometimes, it's either nodular or sessile. In addition, differentiating RMM from other anorectal tumours is rendered more difficult since 30% are non-pigmented.
Colonoscopy is a necessity for identifying RMM. Additionally, finding melanocytic characteristics thanks to histology and immunohistochemistry by using a classic colouring of Fontana expressed by tumour cells (S100 + , HMB48 + , vimentin + ) is fundamental to the diagnosis of RMM. 6
Endoscopic ultrasound (EUS), computed tomography (CT) and magnetic resonance imaging (MRI) are the mainstay for local and systemic staging, along with PET scanning to look for distant metastases.
The stage of RMM can be simplified on 3 levels (I, localized tumour with or without satellite(s) within a distance of 2 cm from the primary tumour; II, regional nodal metastases and/or nodules more than 2 cm from the primary, but not beyond the lymphatic drainage area of the primary; III, distant metastases). 7
As a result of its poor prognosis, the treatment is highly debateable with no consensus reached to date. Previously, the APR was the commonest treatment method because of its complete local control. But this has a high morbidity and functional limitations so local excision has become more commonly performed in recent years. However, due to high local recurrence rate, the recent data results substantiate the role of adjuvant radiotherapy combined to LE in decreasing the local recurrence rates. In our case study, the patient underwent an APR for localised RMM and put onto surgical follow-up. He was disease free for 5 years until he represented with local recurrence and multiple metastasis and then received immunotherapy. We additionally review the case in question with recurrence-free survival rate related to LE in literature.
Case presentation
Chief complaints
The patient was a 72-year-old man who presented with rectal syndrome and a discrete blood stool for 2 months.
History of past illness
The patient reported a history of defaecation pains and intermittent discrete rectorrhagia for 2 months, with a body weight loss over the past 4 months.
Personal and family history
The patient has diabetes and high blood pression. No family medical history.
Physical examination
Rectal examinations found an intrarectal polypoid mass at 5 cm from the anal margin.
Laboratory examinations
Serum tumour markers, including carcinoembryonic antigen, cancer antigen-125 and cancer antigen-19-9 were in normal ranges. In addition, normal liver and kidney function were revealed. Mild anaemia with haemoglobin of 11.4 g/dL (normal range: 12–16) was revealed.
Imaging examinations
Colonoscopy with biopsy showed hyperplastic rectal polyps and low rectal polypoid masse.
The pelvic MRI showed a pedunculated polypoid lesion, endo-luminally budding, measuring with the lower pole 40 × 26 mm at 51mm from the anal margin (AM).
The CT-TAP was normal.
The diagnosis of malignant melanoma was confirmed preoperatively by histopathology.
Final diagnosis
The final diagnosis was confirmed to be primary rectal melanoma T2N0M0.
Treatment
He was treated surgically by APR with permanent colostomy.
The specimen had 21 cm long and 8 cm in diameter.
On opening, the tumour was budding, blackish-grey, brittle, measuring, 5.5 × 3cm infiltrating the entire rectal wall, located at 3 cm from the distal limit of the resection.
Absence of vascular emboli, perineural invasion and the lymph nodes metastasis with a clean lateral limit.
History of present illness
Deep vein thrombosis, deterioration of general condition, dyspnoea, abdominoperineal pain.
Outcome and follow-up
Afterward, the patient underwent regular clinical examinations and imaging scans (CT or colonoscopy) for 5 years with satisfying results without metastasis and local recurrence.
One year later, the patient presented with leg swelling due to deep vein thrombosis.
The PET scan, CT TAP, and the histopathology of lung biopsy fragments: found local recurrence, secondary pulmonary, bone and muscle metastasis with distant lymph node one, the prevertebral inferior mediastinal and the right primitive iliac (figures 1 and 2). He received 4 sessions of immunotherapy with anti pd1 monoclonal antibodies (pembrolizumab) at a dose of 200 mg by slow infusion every 21 days. The control with pet scan did not show any improvement. Furthermore, it objectified an aggravation of the pre-existing tumour lesions and the appearance of other secondary hepatic, cardiac, muscular, intestinal and another lymph node metastasis (figure 3) The decision was to put him under chemotherapy with paclitaxel 30 mg during 8 sessions over 8 weeks. The patient passed away before finishing all of chemotherapy sessions.

Computed tomography for pelvic imaging in rectal melanoma 5 years after APR: A: Pelvic soft tissue suspicious for local recurrence. B and C: suspicious bilateral nodal pelvic metastases.

PET-scan for body imaging in rectal melanoma 5 years after APR: Intense FDG-activity in inferior mediastinal lymph nodes, the lungs, right iliac nodes, right ischia-pubic bone, within the pelvis and in the right obturator interns muscle.
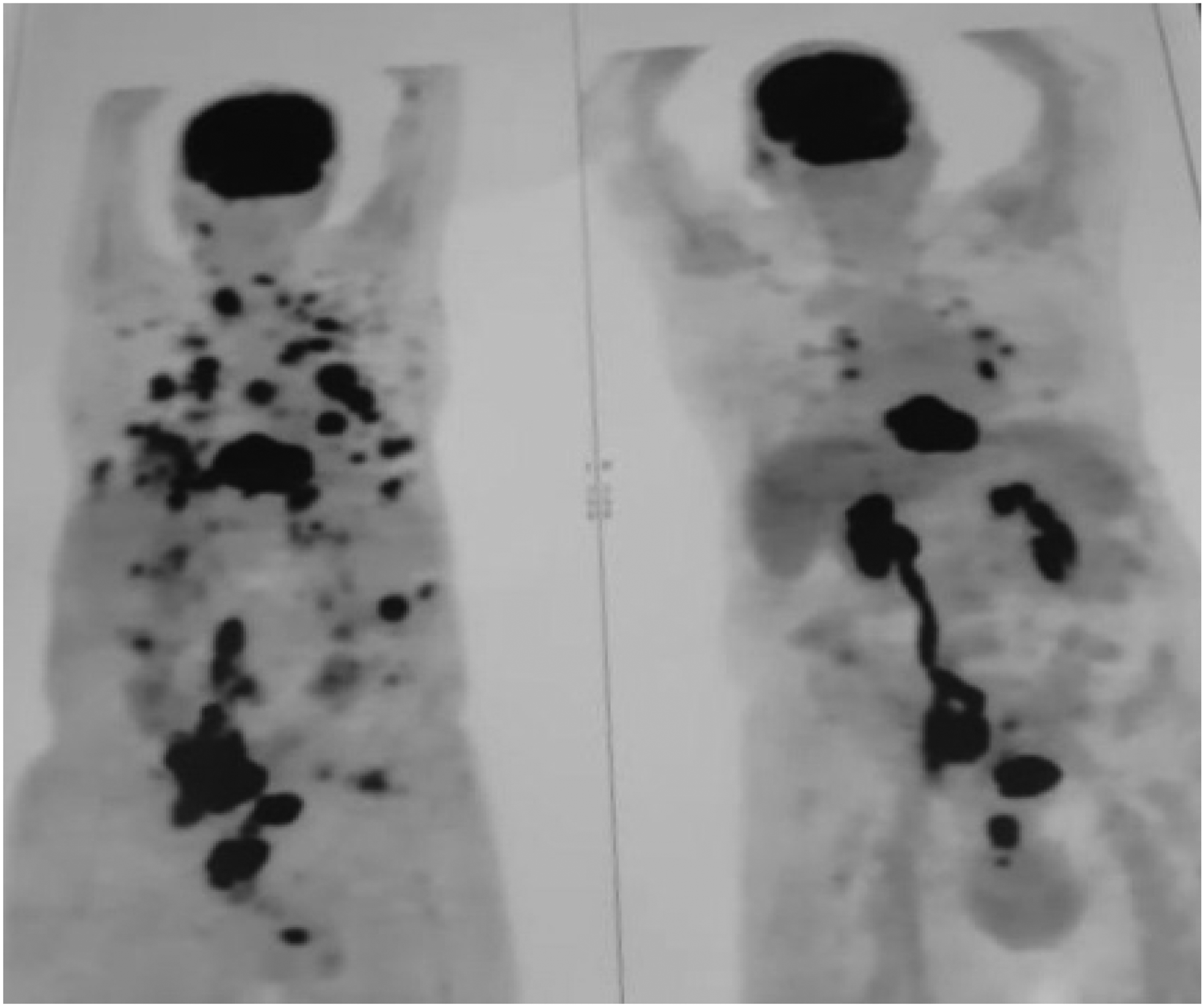
PET-scan for body imaging in rectal melanoma after immunotherapy: aggravation of pre-existing lesions and marked progression throughout the body following immunotherapy.
Discussion
Rectal melanoma is exceptionally unusual, aggressive tumour, representing 1–3% of all malignant melanomas and less than 1% of all anorectal malignancies. The prognosis is poor with a median survival of 16 months and overall survival of 14% at 5 years. 8 Although surgery remains the optimal treatment with the aim to achieve an R0 resection, outcomes remain poor.
Formerly and long before, APR was recommended by most authors, 8 because of its highly local control rate and ensuring a safe resection margin. However, due to its low survival rate and the frequency of its complications, newer recommendations are in favour of local excision when negative margin can be achieved (Procedures without lymph node removal and preservation of the rectum) following by radiotherapy.8–10
Local excision of a rectal tumour can be Performed with zero threat of morbidity or mortality, in the meantime, extensive resection is a far more intrusive procedure with drawbacks such as a longer hospital stay, a longer recovery period and frequently the concern of a colostomy with unfavourable effect on the lifestyle. The current data shows that the general survival was better when R0 resection was done by local resection than when APR was required.7,9
To spare the APR's morbidities, it is true that the LE is considered as a credible approach when negative margins can be achieved. 8 Nonetheless, there are many disadvantages of the clinical use of LE, particularly when the tumour size is too large to be completely resected initially. The incidence of local recurrence after local surgery has been reported to be high around 50%. This consequently compromises the goal of performing limited surgeries.
Some studies have demonstrated an increase in survival with APR or pelvic exenteration in selected patients, such as those with lower stage cancers. 11 This seems the case with our patient who defied prognostic indicators by surviving disease free for 5 years after APR.
On the other hand, the laparoscopic ultralow anterior resection (ULAR) with total mesorectal clearance is considered as a standard approche in treating low rectal cancer, but using ULAR for RMM has never been reported. In theory, ULAR has the advantage of a LE and it is equal with APR. Additionally, mesenteric lymphadenectomy could be adequately conducted by ULAR. The most important advantage of ULAR compared to APR is preserving the gastrointestinal continuity. 12
Regardless of tumour stage, if we compare surgical approaches, none of them confer an improved survival above the others. 11
Adjuvant therapies including chemotherapy, radiotherapy and immunotherapy are higher in demand because of the poor prognosis of RMM. Recent cases, report that Local excision combined to adjuvant radiotherapy having a favourable effect, by decreasing a local recurrence rate under 20%, and increasing the sphincter preservation and function.10,13,14 However, more research on the effect, fractionation and timing in relation to surgery are required.
Immunotherapy consists of using monoclonal antibodies directed against immune checkpoints. Currently, the anti-checkpoints used in oncology target inhibitory receptors present on the surface of lymphocytes (CTLA4, PD1) or their ligands (PD-L) expressed by tumour cells to evade the immune system.
Some studies show that the response rate to inhibitor therapy is between 30% and 50%, which is superior to chemotherapy. However, Low immunogenicity of anorectal melanomas, as defined by low mutation burden (and hence low neo antigenicity), low TILs infiltrates, and low PD-L1 expression, may contribute to poor immunotherapy responses.15,16 Because of our patient who received immunotherpy until local recurrence and metastasis stage with ineffictive result. we need in the futur to demonstrate the role of immunotherapy in the neoadjuvant and adjuvant setting.
In our case report, APR was successful in keeping our patient disease free for 5 years, allowing excellent local disease control, before developing local recurrence and metastatic disease followed by hyper-progression when given immunotherapy. This suggests that APR despite its greatrer morbidity should not be abandoned in favour of more local excision options, even though these are now gaining more credibility.
Conclusion
The management and treatment of RRM continue to be challenging for all physicians and surgeons. APR remains a preferred surgery method for this rare and poor prognosis disease by producing a complete local control and a long desease free survival independently to palliative treatement. The local excision following by radiotherapy doesn't always give best outcomes, in this case giving immunotherapy did not help at all.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article