
Abstract
Summary
Idiopathic left ovarian vein thrombosis was diagnosed in a 27-year-old woman at the time of a diagnostic laparoscopy performed because of a suspected ovarian torsion.
The diagnosis was confirmed by abdominal computed tomography scanning. Subsequent magnetic resonance imaging showed no signs of an abdominal or pelvic mass nor enlarged lymph nodes. The patient was treated with systemic anticoagulation therapy for 3 months and made a good recovery. During follow-up it became clear that the patient was already diagnosed with familial hypercholesterolemia before the occurrence of the ovarian vein thrombosis. It remains unclear if familial hypercholesterolemia played a role in the occurrence of ovarian vein thrombosis in our patient.
Keywords
Introduction
This manuscript highlights a very rare case of idiopathic left ovarian vein thrombosis (OVT). OVT is a rare disease that affects the right ovarian vein in 70–90% of the cases. It occurs in 0.05–0.18% of births after vaginal delivery and in 2% of births by Caesarean section.1,2 Idiopathic OVT is a rare occurrence and is associated with malignancy, prior pelvic surgery, and pelvic inflammatory disease.3–5 Recently, OVT has been associated with COVID 19 infection, presumably because of a hypercoagulable state caused by the virus.6,7
In this paper, we report a case of a 27-year-old woman with familial hypercholesterolemia (FH) presenting with abdominal pain suspected of ovarian torsion, which turned out to be left OVT found during laparoscopy. We found only three other case reports describing left idiopathic OVT,8–10 and no articles describing OVT in patients diagnosed with FH.
Case report
A 27-year-old woman presented with abdominal pain. The pain commenced one week earlier in the lower left abdominal quadrant, increased over time, and spread throughout the whole abdominal area. She was nauseated, without vomiting. The patient had already taken a substantial number of painkillers: acetaminophen, diclofenac and tramadol.
In her medical history she was diagnosed with familial hypercholesterolemia based on the P664L exon 14 mutation (heterozygous). She used a hormonal intrauterine device as contraceptive (progesterone only). She had a body mass index (BMI) of 21.6 and did not smoke. On examination she was normotensive with a blood pressure of 125/80 mmHg, a heart rate of 76 bpm, and a temperature of 36.8°C. Abdominal examination was painful, especially in the hypogastric region, lower right quadrant and left upper quadrant.
Laboratory studies were normal. There was no leukocytosis (white cell count: 8.1 × 109/L), the C reactive protein level was not elevated (<1 mg/L; cut-off value: <5 mg/L) and beta-HCG was low (<1 IU/L; cur-off value: <5 IU/L). Urine examination and culture were negative.
Transvaginal ultrasound examination revealed a small cyst (3.8 cm x 3.6 cm x 4.1 cm) in the right ovarium. There were no other relevant findings.
The diagnosis of ovarian torsion was suspected and a diagnostic laparoscopy was performed. Serous fluid was aspirated from the cyst but there were no signs of an ovarian torsion. The vein in the left infundibulopelvic ligament was congested and had a thrombotic appearance (see Figure 1). This finding suggested an ovarian vein thrombosis.
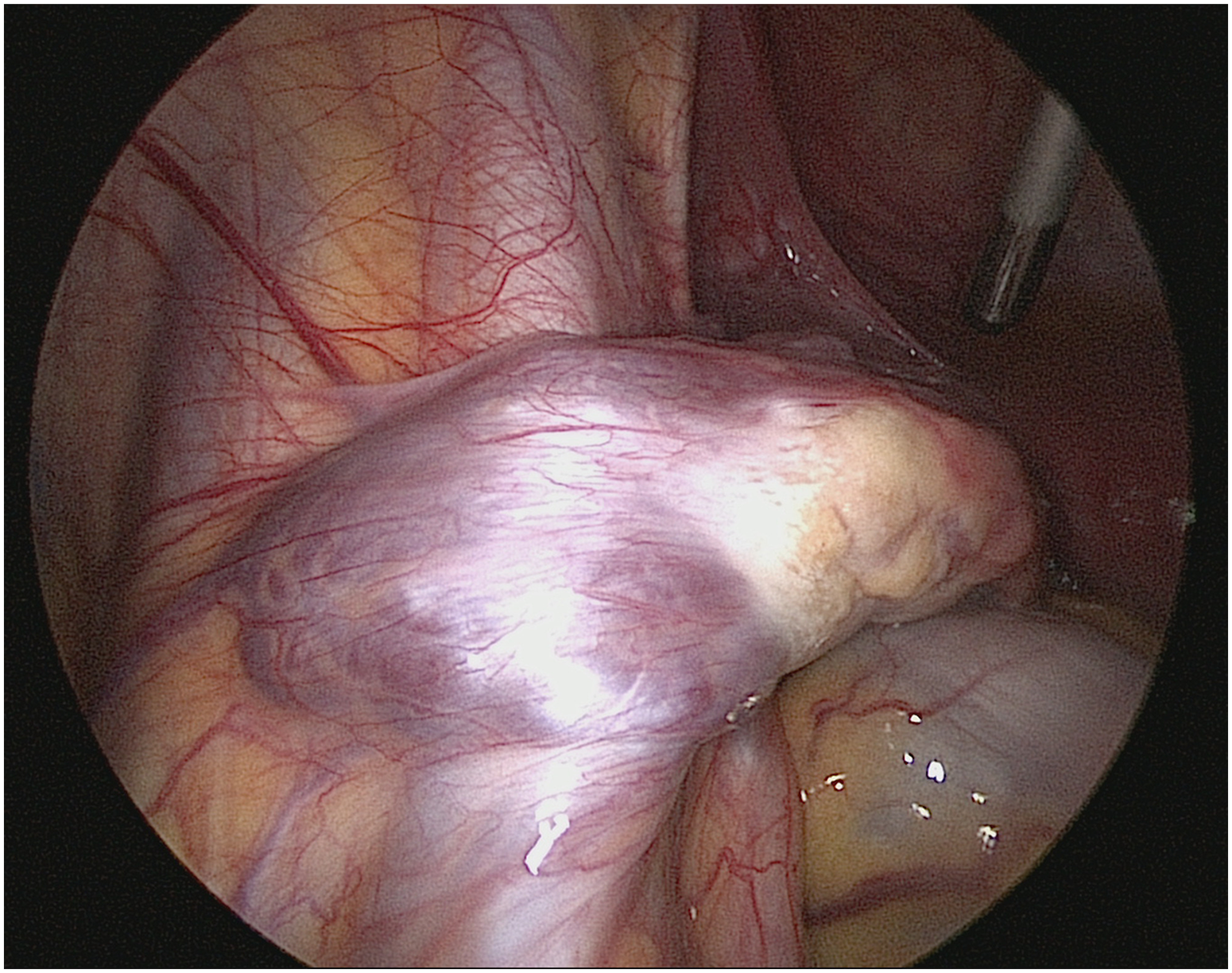
Laparoscopic evaluation showed the left infudibulopelvic ligament was congested and had a thrombotic appearance.
D-dimer levels, measured after laparoscopy, were not elevated (0.30 mg/mL; cut-off value: 0.50 mg/mL). The case was discussed with a radiologist who suggested to perform an abdominopelvic computed tomography (CT) scan with contrast. The CT scan showed pelvic congestion syndrome with a thrombus in the left ovarian vein (see Figure 2). There was no thrombus in the right ovarian vein.

Coronal plane of abdominal CT. The encircled area shows the presence of a thrombus in the left ovarian vein.
Additional abdominal magnetic resonance imaging (MRI) was performed because of the discrepancy between normal D-dimer levels and images of an ovarian vein thrombosis on the CT scan. MRI revealed a small intramural myoma, less than 1 cm in diameter but no other abnormalities. There were no signs of an abdominal or pelvic mass and there were no enlarged lymph nodes.
Treatment consisted of systemic anticoagulation therapy (apixaban 10 mg every 12 h for 7 days, followed by apixaban 5 mg every 12 h for 3 months). The pain decreased within 24 h after starting anticoagulation therapy and the patient became asymptomatic 96 h after starting anticoagulant therapy.
The patient was referred to a hematologist and clinical follow-up was done in 3 months. Laboratory studies showed normal levels of Apo-lipoprotein B100 (0.92 g/L; range 0.55–1.25 g/L), total cholesterol (5.3 mmol/L; range: 5.0–6.5 mmol/L), LDL-cholesterol (3.5 mmol/L; range: 3.5–4.4 mmol/L), HDL-cholesterol (1.51 mmol/L; cut-off value > 1.1 mmol/L), and triglycerides (0.64 mmol/L; cut-off value: < 1.7 mmol/L). The patient did not start with statin therapy. In addition, laboratory findings showed normal levels of TSH (2.82 mIU/L; range 0.35–4.94 mIU/L) and free T4 (13.1 pmol/L; range 9–19 pmol).
No additional thrombophilia tests were performed.
Discussion
OVT is an uncommon disease that most often occurs during pregnancy and the postpartum period. OVT occurs in 0.05–0.18% of births after vaginal delivery and in 2% of births by Caesarean section.1,2 OVT has also been associated with malignancy, prior pelvic surgery, and pelvic inflammatory disease.3–5 The right ovarian vein is involved in 70–90% of the cases. 1 This can be explained by incompetent valves and the anatomic course of the right ovarian vein, terminating in the inferior vena cava (the left ovarian vein terminates in the left renal vein).11,12
Symptoms of OVT are often nonspecific and include lower abdominal pain and fever. Common clinical and laboratory findings include tachycardia, nausea, vomiting, and leukocytosis. 13 Diagnosing OVT can be difficult, since other gynecological and surgical diagnoses can present with similar signs and symptoms and laboratory findings (e.g. appendicitis, endometriosis, tubo-ovarian abscess, and adnexal torsion).13–15 If left untreated, OVT can lead to life-threatening complications, such as an pulmonary embolism and extension of the thrombus into the inferior vena cava. 12
Imaging is the cornerstone to diagnose OVT, since it is difficult to diagnose because of the nonspecific symptoms and absence of specific laboratory findings. CT is the imaging technique of choice, with high sensitivity and specificity rates.11,16,17 MRI forms a useful alternative with high sensitivity rates.3,11 Ultrasonography is less sensitive than CT or MRI, since it might be difficult to scan the entire length of the ovarian vein, and imaging can be hampered by bowel gas and overlying structures.3,11
Treatment of OVT consists of anticoagulation with direct oral anticoagulants. The recommended use of anticoagulants in the literature ranges from three to six months.8,18 Surgical treatment might be necessary in persistent cases despite optimal approach.8,10
In this particular case, the diagnosis was made accidentally during laparoscopy on the appearance of a congested thrombotic ovarian vein in the left infundibulopelvic ligament. Moreover, the cause of OVT in this patient is not clear. Studies indicate that patients with FH have an increased chance of cardiovascular disease and have an increased coagulation. 19 It remains unclear, however, if this might be the cause of OVT in our patient, since she was heterozygous for the P664L exon 14 mutation and did not have elevated cholesterol and triglyceride levels.
Learning points/take home messages
Idiopathic ovarian vein thrombosis is a rare but potentially life-threatening diagnosis.
During laparoscopy, performed in women with acute abdominal pain, the veins in the infundibulopelvic ligaments should be inspected. Especially in the absence of an alternative explanation for the signs and symptoms in the particular case.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Written informed consent for patient information and images to be published was provided by the patient.