
Abstract
Summary
The Zephyr (PulmonX Inc., Redwood, CA) endobronchial valve (EBV), predominantly designed for lung volume reduction in emphysema, can also be used to close a spontaneous or post-operative prolonged air leak (PAL). We describe a previously unreported complication of cutaneous migration of an EBV, inserted for management of a PAL from a postoperative bronchopleural fistula (BPF), in a 62-year-old male following a right upper lobe posterior-apical (S1,2) segmentectomy. His PAL resulted in a chronic empyema which failed to respond to surgical debridement, anterior cavernostomy and pectoral myoplasty. Bronchoscopic closure of the air leak by EBV insertion resulted in clinical improvement but there was a residual chronic wound sinus through which the patient reported protrusion of a foreign body that was causing irritation. It was the EBV. We hypothesise that the BPF healed beneath the EBV causing it to dislodge but its route to the skin remains a mystery.
Introduction
The Zephyr (PulmonX Inc., Redwood, CA) endobronchial valve (EBV), predominantly designed for lung volume reduction in emphysema, can also be used to close a spontaneous or post-operative prolonged air leak (PAL). 1 Recognised complications related to EBV insertion include valve expectoration; mucus plugging or granulation tissue infiltration. We describe a previously unreported complication of cutaneous migration of an EBV, inserted for management of a PAL from a postoperative bronchopleural fistula (BPF).
Case report
A 62-year-old man with emphysema and reduced respiratory reserve underwent a diagnostic right upper lobe apico-posterior (S1,2) segmentectomy for a suspected small lung cancer. Histology revealed chronic fibrosis only but his post-operative recovery was complicated by PAL resulting in prolonged chest drainage, a persistent apical space and empyema. The empyema was surgically debrided via an axillary thoracostomy but in order to close the air leak, an anterior cavernostomy with resection of the 3rd rib and pectoral myoplasty was required. Unfortunately, the PAL continued requiring prolonged tube drainage and dyspnoea. Fibreoptic bronchoscopy demonstrated a peripheral BPF from a subsegmental bronchus of the remaining anterior segment into the cavity. A size 4 Zephyr EBV (PulmonX Inc., Redwood, CA) was inserted into the bronchus peripherally with significant reduction in the visible chest drain air leak. The patient made a symptomatic recovery allowing drain removal after 2 weeks. Despite long-term antimicrobial and antifungal treatment his myoplasty wound was slow to heal with chronic sinus formation. At a subsequent wound review after 11 weeks the patient complained wound irritation and a foreign body was found to be protruding through the sinus (Figure 1). It was the EBV! Radiological review confirmed the dislodgement of the EBV and caudal migration (Figure 2). The wound subsequently healed and the patient was discharged from follow up.

(A) chronic anterior chest wall sinus (B) removal of subcutaneous endobronchial valve (EBV).
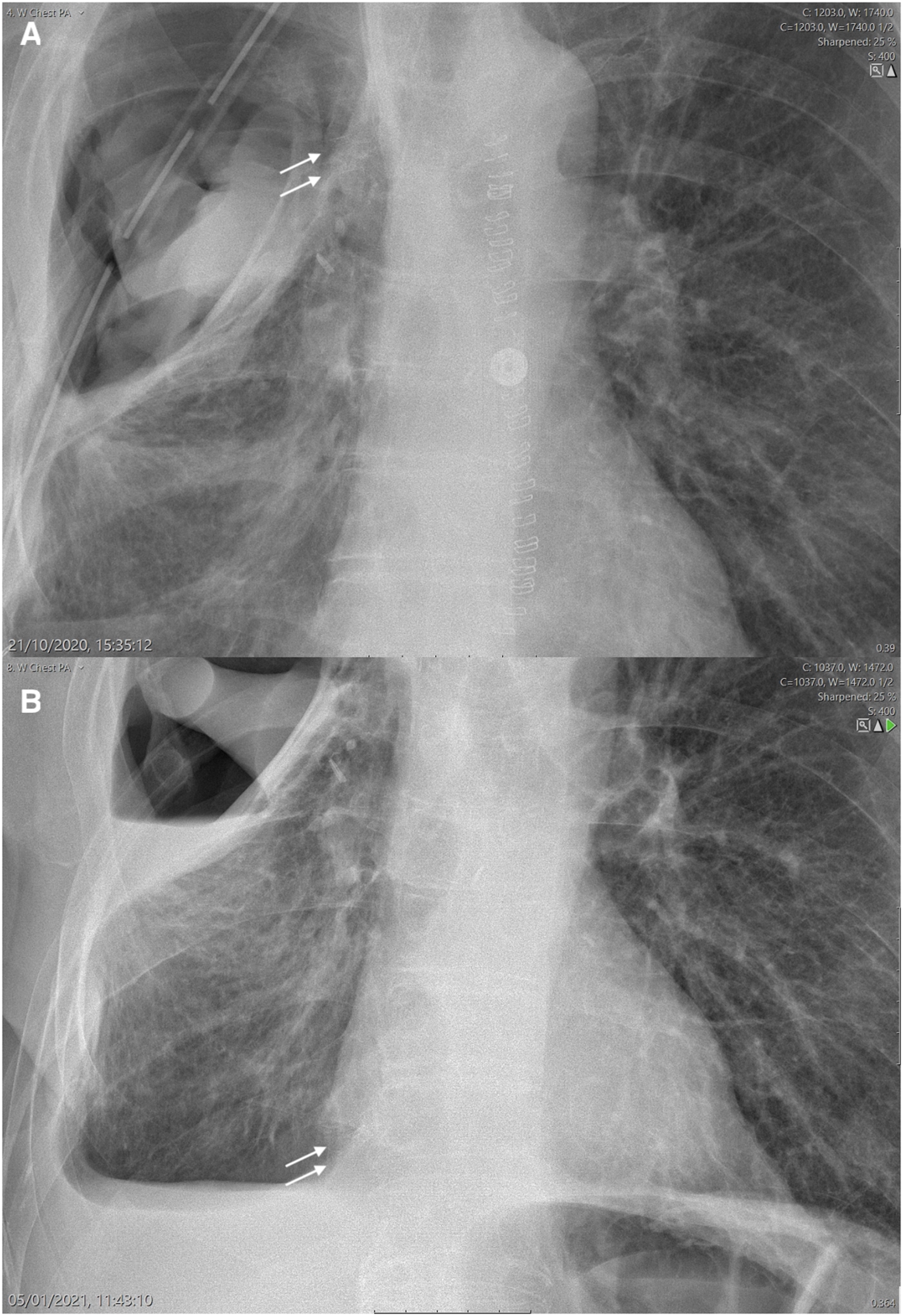
Radiographic migration of endobronchial valve (EBV) (white arrow)
Discussion
The Zephyr EBV is a self-expanding one way valve which was originally designed to achieve lobar collapse and therapeutic lung volume reduction in severe emphysema. The indication for EBV placement has been extended into the management of patients with PAL from a peripheral alveolar-pleural fistula or a more central post lobectomy or post pneumonectomy BPF. By achieving lobar collapse, it is thought that cessation of airflow through the fistula may allow healing and closure. 2
The commonest direct complications from EBV in the first 24 months post-insertion include displacement and expectoration; mucus plugging and granulation tissue infiltration. 3 Intraluminal EBV migration has been reported previously but not leading to expectoration via the subcutaneous route.4,5
A possible cause of EBV migrations include placement of inaccurate size of valves and therefore correct size and placement of valves should be reinforced by an experienced surgeon. Valve migration has been reported in the lower lobes more often, probably due to more collapse of the bronchi compared to the upper lobes. 6 Therefore, although it may be tempting to place a single valve in the lower lobes, it is recommended to place more valves distally in the individual segments. 1 Early detection of valve migration is highly suggestive by clinical signs. When the patients present with acute loss of initial effect and increased dyspnoea, they should be further evaluated radiologically by a chest x-ray or a CT scan. If there is suspicion of dislocation or migration of valves, a bronchoscopy can be performed to evaluate and replace the affected valves. It indicates the need for close follow up and a low threshold for re-intervention on clinical grounds alone, if the initial outcome is suboptimal.
We accept that this was an unusual indication for EBV insertion in a peripheral segmental BPF leading into an infected postoperative cavity with underlying lung tissue. We hypothesise that as EBV migration correlated with resolution of the PAL that proximal healing and remodelling beneath the valve facilitated its displacement from the small airway. Whilst the exact route to the skin remains a mystery, we presume the EBV followed the chronic post infective tract through the thoracic cavity. It is fortunate that the EBV did not become embedded within the residual cavity with unknown consequences.
This case illustrates that the use of EBV for direct closure of peripheral BPF in sublobar airways should proceed with caution. Regular radiographic surveillance is required if this technique is chosen since direct bronchoscopic removal, as is recommended for indirect closure of peripheral leaks by central occlusion, may not be possible. The role of EBV in delayed wound healing is thought to be below clinical significance.
Conclusion
Whilst the use of endobronchial valve occlusion has been shown to have many therapeutic benefits across a wide range of situations this case illustrates that caution must be applied to extended indications.
Presented at Royal Society of Medicine (RSM) 2021
Footnotes
Ethical statement
The patient has given a consent to publication of images and information.
Data availability
The data underlying this article are available in the article and in its online supplementary material.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.