
Abstract
The indolent character of squamous cell carcinoma of the foot can be misleading and might result in unwarranted excisions or delayed treatment.
Introduction
This case highlights the importance of increased index of suspicion for malignancy and need for early biopsy for non-healing wounds.
Case study
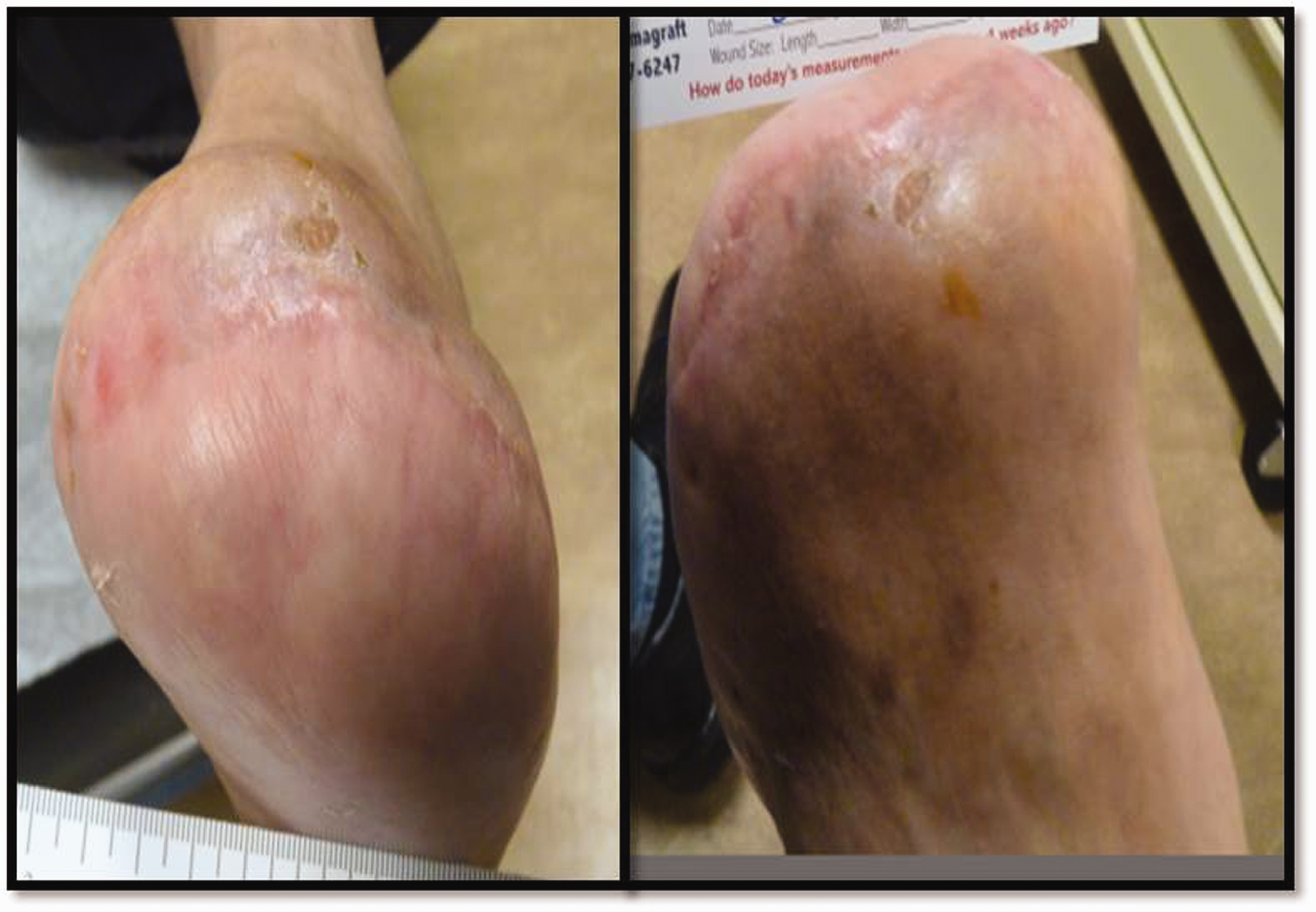
A 66-year-old male with coronary artery disease and hypertension was self-referred to Podiatry for 10-year history of bilateral painful calluses. The left foot plantar callus was ulcerated, associated with bleeding and pain. Wound, previously treated by a wound care certified specialist for nine months, with no reported biopsy, revealed a 5.0 × 5.5 cm left plantar forefoot fungating, raw, beefy granular, lobulated mass, 0.7 cm central depth and irregular thickened borders. The lesion extended from the metatarsal heads to the arch, distal to the sulcus of the second, third and fourth toes. A 1.0 × 1.5 cm lateral cystic lesion exuded cheese-like material (Figure 1), without malodor, erythema, undermining or purulence. A 4-mm punch biopsy, sent for microbiology, mycology, histopathology and radiographs of the foot were obtained.
Clinical photographs of the left foot lesion before (left) and after (right) biopsies.
Biopsy showed acute and chronic inflammation with reactive changes to the squamous epithelium with negative acid-fast stain. Wound cultures grew Serratia and Stenotrophomonas species that were sensitive to Ciprofloxacin. Mycology testing was negative. There was no evidence of bone destruction on plain radiograph (Figure 2). The magnetic resonance imaging showed a 6.2 cm lobulated, polycystic mass along the plantar aspect of the foot, centred over the metatarsophalangeal joints. The tumour extended cephalad along the lateral aspect of the first metatarsal, with a 4.8 cm multiloculated cystic tumour between the first and second metatarsal heads and distal shafts. There was no evidence of bone invasion. The heterogeneity and irregular growth pattern of the lesion were concerning for malignancy (Figure 3). Deeper incisional biopsies revealed invasive squamous cell carcinoma with positive margins. A multidisciplinary tumour board recommended amputation and alternatively radiation therapy. Given radiation estimated control rate of 20%, potential complications of chronic foot pain due to fat pad loss, and non-healing wound, the patient opted for surgical resection. Intraoperatively, there was malodorous liquefaction detritus plantarly invading the intermetatarsal space, consistent with the magnetic resonance imaging. These findings prompted metatarsals disarticulation and precluded salvage of the peroneal brevis tendon or Sanders’ modification. As a result, a Lisfranc amputation and sentinel lymph node biopsy were performed. Histopathology confirmed a diagnosis of squamous cell carcinoma, with 2.5 mm maximum tumour thickness. There was no lymphovascular or perineural invasion, and surgical margins were free of malignancy (Figure 4), corresponding to pT2N0Mx staging by the American Joint Commission on Cancer (8th edition) criteria.
1
Bone, tissue margins and lymph node did not reveal any evidence of malignancy.
Plain radiograph of the left foot. Increased soft tissue prominence at the plantar aspect of the left forefoot without evidence of bone destruction (arrowheads on right panel). Magnetic resonance imaging of the left foot with coronal (left) and sagittal (right) views. Heterogeneous appearing mass with multiloculated cystic lesion between the distal and the second metatarsals. Clinical photographs of the left foot status post Lisfranc amputation.


The patient had an uneventful post-operative course (Figures 5 and 6). He was fitted with carbon composite toe off/ankle foot orthosis and custom moulded boots (Figure 7). Specifically, the Orthotist transformed an ‘off-the-shelf’ Blue Rocker-type, carbon fibre, spring assist ankle foot orthosis with appropriate padding, socket and filler that conformed well into the patient's athletic shoes and work boots. At his six-year follow-up period, the patient is tumour-free without pressure ulcers. He has returned to his previous construction work, climbing ladders, motorcycling, hiking and maintaining his mountain farm with very limited biomechanical impairment.
Histopathology of the excised specimen. The epidermal surface is papillated and expanded by interconnecting cords and lobules of atypical keratinocytes (left). The atypical keratinocytes extend into the dermis and subcutis in a polycystic fashion (right) (Haematoxylin and eosin, ×20). Clinical photographs of the left foot at 45 days postoperative follow-up. Photograph of patient’s customised orthotics and ankle foot orthosis brace.

Discussion
Squamous cell carcinoma accounts for 20% of non-melanoma skin cancer, while the majority of non-melanoma skin cancer is attributed to basal cell carcinoma.2–5 Ultraviolet light from sun exposure causes DNA damage in tumour suppressor genes, which leads to cancer.2–5 Thus, the higher occurrence of squamous cell carcinoma with increasing latitude.2,3 Other aetiologies include ionising radiation, human papilloma virus infection, chemical agents, immunocompromised patients, genetic conditions, traumatised skin and non-healing skin also known as Marjolin’s ulcer.2–6
Squamous cell carcinoma is the most frequently encountered malignancy of the distal lower extremity, as opposed to basal cell carcinoma, melanoma or sarcomas.2–6 The differential diagnosis for foot squamous cell carcinoma includes actinic keratosis, keratoacanthoma, squamous cell carcinoma in situ or Bowen’s disease, basal cell carcinoma, eccrine poroma, verruca plantaris, reactive hyperplasia, pyogenic granulomas, psoriasis, repetitive trauma, bacterial or fungal infection, sweat gland carcinoma, amelanotic melanoma, sarcoma and Hodgkin’s disease.2–6 The clinical presentation can be variable ranging from a small nodule, ulcerating sloughing plaque or an exophytic lesion.2–6 Although the American Joint Commission on Cancer uses a TNM classification, there is no current staging system for cutaneous squamous cell carcinoma outside the head and neck. 1 Because squamous cell carcinoma of the lower extremity has a high likelihood for metastases (up to 30%), early diagnosis is critical.2–7 The five-year recurrence rate of primary lesion is 8% with a good prognosis, while the five-year rate of metastasis is 5%5,8 with a poorer prognosis, in particular with regional lymph node involvement, which occurs in 85% of cases.2–5,8 Plain film radiography of any limb squamous cell carcinoma is crucial to assess for bone involvement. Magnetic resonance imaging and computed tomography are additional tools to define tumour margins and relationship to adjacent anatomic structures. 7 Therapies include electrodessication and curettage, cryosurgery, wide surgical excision, Mohs micrographic surgery, fractionated radiotherapy alone or in combination with other treatments.2,4,5 The goal of management is tissue excision with functional preservation. The level of amputation depends on the tumour grade and size. Perineural invasion increases the risk of tumour recurrence and metastasis. In the presence of metastasis, lymph node biopsy or dissection is warranted.2,9,10
Studies on squamous cell carcinoma of the foot reported different aetiologies,5,10 inadequate treatment, 10 ranging from 4 to 50 years before the diagnosis of squamous cell carcinoma. 10 Treatments included wide excision,5,10 partial or complete toe amputation, 10 transtibial-,5,10 Syme amputations.5,10 The average follow-up intervals were 24 to 105 months 5 and 68 months, respectively. 10
Although the patient had a favourable outcome, a less proximal amputation and a more stable foot may have resulted had the lesion been diagnosed earlier. Indeed, careful examination of longstanding wounds and diagnostic biopsies are essential when treating patients for extended time.
Consulting an expert Pedorthist was critical to help stabilise the patient's foot postoperatively. The patient's compliance and commitment significantly contributed to his own success story. Finally, all of the aforementioned allowed the patient to have decent functionality and gratifying quality of life.
Conclusion
This case highlights the importance of increased index of suspicion for malignancy and the need for early biopsy for non-healing and atypical wounds. It emphasises the value and need of a multi-specialty team approach to maximising limb preservation and successful long-term outcomes of lower extremity wound care.
Footnotes
Declarations
Acknowledgements
We sincerely thank our patient for his cooperation.
Provenance
Not commissioned; peer-reviewed by Rowena Vicencio Venneuguès.