
Abstract
Objective
To investigate recent (2011–2015) research productivity in clinical biochemistry and compare it with a previous audit (1994–1998).
Design
A retrospective audit of peer-reviewed academic papers published in Medline listed journals.
Setting
UK chemical pathology/clinical biochemistry laboratories and other clinical scientific staff working in departments of pathology.
Participants
Medically qualified chemical pathologists and clinical scientists.
Main outcome measures
Publications were identified from electronic databases for individuals and sites. Analyses were conducted for individuals, sites and regional educational groups.
Results
Clinical scientific staff numbers fell by 3.9% and medical staff by 17.4% from 1998 to 2015. Publication rates declined as publication count centiles rose between 1998 and 2015 (e.g. n = 5; 67th→84th centile; p < 0.001). A reduction in productivity was seen in medically qualified staff but less from clinical scientists. Regional staffing was 77 ± 37 (range 30–150) with university hospital laboratory staff accounting for 58 ± 19% (range 30–92%). Medically qualified staff comprised 20 ± 4% of staff with lowest numbers in some London regions. Publication rates varied widely with a median of 155 papers per region (range 98–1035) and 2.82 (1.21–8.62) papers/individual. The skew was attenuated, increasing the publication rate to 6.0 ± 2.73 papers (range 2.29–11.76)/individual after correction for the number of university hospital sites per region and was not related to numbers of trainees. High publication rates were associated with the presence of one highly research-active individual. Their activity correlated over their careers from recruitment to today (r2 = 0.45; p = 0.05). The productivity rates of recent cohorts of trainees are inferior to previous cohorts.
Conclusions
Research remains a minority interest in clinical biochemistry. A small and decreasing proportion of individuals publish 90% of the work. A reduction was seen in clinical scientist and especially medical research productivity. No correlation of training activity with research productivity was seen implying weak links with translational medicine.
Introduction
There is increasing concern about the relationship between science and medicine. Although the practice of medicine is increasingly evidence-based, there seems to be a decline in scientific publications from clinical departments and in pathology possibly driven by an increased focus on narrow measures of clinical productivity. 1 Pathology, being a laboratory-based scientific specialty, should be subject to lesser such pressures. Some sub-specialities of pathology such as clinical biochemistry combine input from scientific staff (often with previous doctorate-level degrees) as well as clinicians, many of whom have undertaken higher level scientific degrees as part of their clinical training. It is a requirement of training programmes that clinical scientific and medical staff should complete a research project lasting a period of one year. This is formally assessed as part of the Royal College of Pathologists’ examinations as being of publishable quality. Examination modules also include a section on scientific interpretation of peer-reviewed publications relevant to the field and annual training reviews also review clinical audits performed by trainees.2,3 The presence of publications from both scientist and physicians in training is assessed as part of the data returned in annual reviews of competence progression and public presentation and formal peer-reviewed publication of projects is encouraged.
In 2002, we reported a study of the publications by workers in chemical pathology/clinical biochemistry for 1994–1998. 4 Since that time, there have been many reports on clinical productivity in pathology, such as the Carter Reports which mandated the development of managed pathology networks5,6 and resulted in the proposed removal of £500 million from pathology budgets.5,7,8 It would be expected that removing funding from an area would reduce the amount of research that could be carried out. On the positive side, the National Institute for Health Research has been created which has resulted in improved funding for research infrastructure in the NHS. 9 In many hospitals, this has resulted in extra funding to allow support for research in clinical departments, but it is not clear whether this will have resulted in extra research being published by those working in pathology.
This study aimed to re-audit chemical pathology publications to identify whether the events of the last 20 years have had any significant impact on research productivity.
Methods
The methods used for this audit were identical to our previous publication. 4 Personnel to be literature searched were identified from the Association for Clinical Biochemistry Members’ Handbook (2012–2013) and through membership of the Royal College of Pathologists. Publications were identified using the Ovid search engine. 10 All searches were carried out for the period 1946 to 2018, selecting for the period 1 January 2011 to 31 December 2015. Searches were conducted using first and multiple initials and were evaluated manually for attribution based on hospital site. All searches in this audit were carried out by the same individual who had completed the searches in the first audit. Hospitals sites were classified by Higher Education England region (pre-2016), 11 and status as university/teaching hospital hub laboratory as defined by local sample referral patterns. Data were matched with data from the 1994–1998 survey so that trends in publication over a career could be evaluated.
Analyses were performed to determine numbers in each discipline in 1998 and in 2015 and their total numbers of publications. Total staff numbers (both fully qualified and trainees) were assessed as was the distribution between medically and scientifically qualified staff. Laboratories were grouped by NHS Health Education England region (pre-2016) and data re-analysed by region as opposed to site. University hospital sites were identified by the presence of a medical school physically located with the regional hub hospital. Regional laboratories and academic centres have access to specialist equipment and specialised staff and access to specialist clinical services. These are more likely to review unusual cases, be able to assemble cohort studies and being usually linked a medical school are likely to be able to publish novel data, so a further adjustment was performed for the status of the hospital as either a university or district hospital in the region. Numbers of trainees were ascertained by those joining speciality society/college registers with first stage qualifications (e.g. Fellowship of the Royal College of Pathologists) from 2010 to 2015 to allow for a one-year publication delay.
Data on individuals with substantial research productivity (>10 papers in the five audit period 2011–2015) were analysed using publication and bibliometric data 12 obtained from Web of Science 13 in five-year cohorts based on publication rates in the first five years after the date of joining the profession and for 2011–2015 in the same cohorts.
Statistical analysis
Differences between groups were assessed by non-parametric Spearman rank tests and distribution frequencies by the Kolmogorov–Smirnov test. Regionally grouped data were compared using correlation statistics and Pearson statistics. Categorical analysis was performed using Fisher exact test and Chi-square tests as appropriate for the number of groups.
Results
Staffing in chemical pathology
Baseline data sources identified 1170 chemical pathology staff (909 clinical scientists and 261 medically qualified) and 324 members in other pathology disciplines (genetics, immunology, haematology, microbiology or virology), compared with 1262 (946 clinical scientists and 316 medically qualified) and 243 other pathology disciplines in the first survey. This represented a 3.9% reduction in identifiable clinical scientist staff and a 17.4% reduction in medically qualified staff in chemical pathology.
Publications in chemical pathology
As previously, data on total publications showed a clear exponential distribution, with 90% of publications arising from 348 (23.3%) individuals, compared with 90% of publications arising from 237 (20.8%) individuals in the previous survey. The centiles at which specific numbers of publications were achieved are shown in Figure 1.
Centile at which a certain number of publications is achieved for different staff groups in clinical biochemistry and clinical scientists in other pathology disciplines for the periods 1994–1998 and 2011–2015.
Overall, the publication rates in the 1998 survey are very similar to those in the 2015 survey. Differences between groups are identifiable with medically qualified staff publishing the most and clinical scientists in biochemistry publishing the least. Rises in centiles at which publication rates are achieved were observed across all groups between 1998 and 2015. The greatest centile increase was seen in medically qualified staff (e.g. n = 5; previous 67th now 79th centile of group) and to a lesser extent in clinical scientific staff in biochemistry laboratories. In contrast, publication centile rates for non-biochemistry scientific staff were stable for 0–5 publications and only declined in higher publication groups (Figure 1).
Direct comparison of individual productivity at both time points
Distribution of publications by staff group for those staff members represented in both surveys: number of publications at specified centiles.
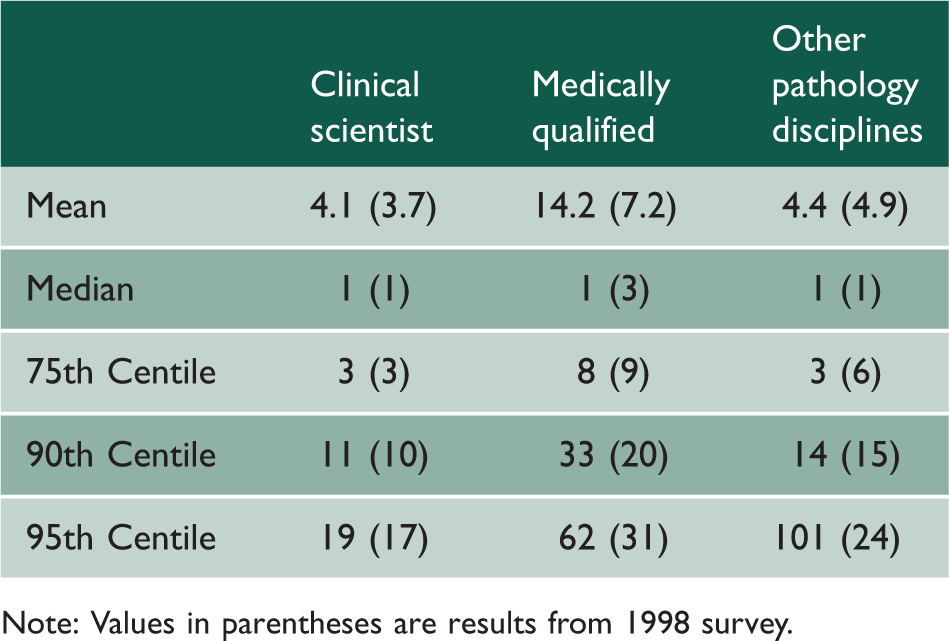
Note: Values in parentheses are results from 1998 survey.
Analysis by category of number of publications in surveys of research in 1994–1998 and 2011–2015 for individuals identified as working in both audit periods.

Regional comparisons and training
As chemical pathology training is provided on a regional basis, the data were re-classified into educational regions as present in 2015. Total staff numbers (both fully qualified and trainees) were assessed as was the distribution between medically and scientifically qualified staff. Publication rates for each region are shown in Figure 2 both as raw data and after adjustment for numbers of staff and numbers of staff in university hospital sites (as a proxy for the number of specialist laboratory services).
Publications in the audit period by clinically or scientifically qualified staff per individual identified and after adjustment for the number of university hospital (regional laboratory) sites.
Each region had 77 ± 37 (range 30–150) staff with university laboratory staff accounting for 58 ± 19% (range 30–92%) of staff. Medically qualified staff comprised 20 ± 4% of staff across all regions but lower numbers were found in the London North East (12%) and London Central (15%) regions. Publication rates varied widely with a median of 155 papers per region (range 98–1035) and 2.82 (1.21–8.62) papers/individual over the audit period. Adjustment by number of university hospital staff attenuated the skew in the distribution increasing the publication rate to 6.0 ± 2.73 papers (range 2.29–11.76) per nominal large laboratory site.
Further investigation of sites/regions with high publication rates showed the presence of one highly research-active individual as being responsible for most of the variance between each region. For example, in Scotland, London North West and London Central individuals with 457, 2797 and 1292 publications and an h-score2015 of 94, 149 and 72 accounted for most of the difference between regions. These research active individuals showed a reasonable correlation between their first five years' productivity on joining the profession with their activity in the 2011–2015 survey but with outlier variances (r2 = 0.45; p < 0.05). Reviewing publication rates by five-year cohorts suggested a decrease in publication rates after 1996 (Figure 3).
Average and median publication rates for 2011–2015 for different cohorts joining the profession at approximately five-year interval periods.
The number of trainees ranged from 0 to 30 (average 14; median 13) per region over the period 2010–2015 with no correlation with publication rates overall or within these for clinical scientist or medical sub-groups. Analysis of publication rates in the first five years after joining the profession by recruitment cohorts showed stability in average publication rates for cohorts (n = 2–5) from 1979 until 1996, a hiatus between 1996 and 2005 and then a return to previous rates for the 2006–2015 cohorts (Figure 4).
Average and median publication rates for new entrants for five years after joining the profession grouped in five-year cohorts of joining the profession.
Discussion
Pathology is a laboratory provided scientific service that is used in the clinical diagnosis and monitoring of patients. The importance of laboratory medicine and its role in implementing translational medicine has been recognised in a number of reports from the Royal College of Pathologists, 12 the Association of Clinical Biochemistry and the Department of Health Scientific Service. 1 Pathology is involved in 70% of diagnoses and 50% of all chronic monitoring. 12 However, pathology services have not been immune to wider developments in the NHS which have involved increased pressures on funding, automation of many commoner assays and emphasis on reorganisation and consolidation of services from units serving 300,000–500,000 individuals as single sites to ‘hub and spoke’ services serving catchments of 1.0–1.2 million.5–8 Budget cuts allied with the aging demographic profile of the workforce13,14 have led to substantial staff losses through retirement and non-replacement allied with consolidation.14,15 Changes in clinical and regulatory frameworks have also changed the job descriptions of staff. Medical staff are increasingly required to provide outpatient services in metabolic medicine with workloads increasing from approximately 1 clinic per week to 2–3. In many cases this has led to cross-site working and a reduction in medical laboratory time.5,15 Meanwhile, scientific staff have to cope with increased complexity of laboratory services, a significant increase in hospital governance requirements and far more detailed accreditation inspections required for ISO15189. 5
Laboratories in university hospitals have also seen changes in academic medicine. A number of new medical schools focused on undergraduate education became functional between 2010 and 2015, while within older establishments Research Assessment Exercises resulted in the reconfiguration and often concentration of academic disciplines in novel organisational formats that did not correspond with traditional clinical departments. 16 There have been changes in medical and scientific workforce planning with the introduction of a more widely based clinical scientific training through Modernising Scientific Careers 17 and reform of the pathways of clinical medical education with a greater emphasis on the demonstration of clinical competences in structured service training programmes to guide promotion to established career grades (consultant posts) rather than academic publications. 3 The research and clinical governance frameworks have also changed with increasing demands made by local and later Regional Ethics Committees, additional data and funding requirements by Research and Development departments with regard to legal sponsorship of investigational studies and formal reimbursement of hospital contributions to research in the NHS (Clinical Research Networks).
Substantial changes have occurred in departments of chemical pathology over the last 20 years. In comparison with the survey in 1998, by 2015 the number of clinical scientific staff had decreased by 4% but the number of medically qualified staff had fallen by 17%. However, the membership of the Association of Clinical Biochemistry has increased by 33% as a result of the incorporation of other pathology disciplines such as medical microbiology and increased membership in areas such as haematology or genetics as services have evolved.
Clinical biochemistry training includes a scientific research project and many individuals possess higher scientific degrees – at least an MSc and more usually a PhD or MD (the UK version available to clinically qualified staff involves a two-year supervised research qualification). 2 This survey highlights that many staff have no opportunity or desire to pursue any scientific work and 50–60% produced no peer-reviewed publications in 2011–2015 but this did not represent a significant change compared to 1994–1998. This may reflect life choices but may also be caused by laboratory consolidation and increasing service and managerial pressures on their time.18,19
Publication rates in the 2015 survey are similar to those in the 1998 survey with a highly skewed distribution and a clear reliance on a small number of highly research-active individuals to maintain the scientific profile of the discipline. As previously, 90% of the publications originated from 20% of the staff who were disproportionately located in university regional laboratories. The methods used in this and the previous audit relying on college or specialty association membership are likely to identify most members of the profession but a few who are members of neither organisation (for instance those are Members of the Royal College of Physicians only) would be missed. In contrast to pathology, other academic departments in the UK seem to have increased their output. 16 As previously, differences between groups are identifiable within clinical biochemistry with medically qualified staff publishing the most and clinical scientists in biochemistry publishing the least. Rises in centiles at which defined publication rates are achieved were observed across all groups between 1998 and 2015 and especially for medically qualified staff. In contrast, publication centile rates for non-biochemistry scientific staff were stable for 0–5 publications and only declined in higher publication groups possibly due to changes in staffing caused by the demographic profile of the profession.13,14 The life cycle of research-active staff in clinical biochemistry mirrors that of other clinical and non-clinical academic disciplines. Thus, individuals that begin to publish early in their career tend to continue and reach a plateau of high productivity during middle age 20 with some achieving hyper-productive levels. 21 This was also seen in chemical pathology comparing initial productivity (all before 2004) with papers published in 2011–2015 (r2 = 0.45; p = 0.05) which included three individuals with ultra-high academic productivity. Reviewing publication rates by five-year cohorts suggested a decrease in publication rates after 1996 which coincides with the start of reforms to both academic and clinical pathology departments. Publication rates in the first five years after joining the profession by recruitment cohorts showed stability in average publication rates for cohorts (n = 2–5) from 1979 until 1996, a hiatus between 1996 and 2005 and then a return to previous rates for the 2006–2015 cohorts, possibly reflecting the increased emphasis on recruiting clinicians with an interest in metabolic medicine who often have higher scientific degrees. This may reflect changes in recruitment, training programmes and opportunities to pursue scientific research as well as increases in clinical workload. 18 The reduction in clinical involvement in science and reduction in clinician-scientist programmes has been highlighted across many health systems including well-funded systems such as exist in the USA. 22
Concern exists about changes in rates of recruitment to medical specialties in the UK. 14 Some systematic research has been performed into career choices in medicine and in pathology.19,23 These have identified that poor visibility of smaller specialties following curriculum rearrangements in medical schools that reduce specialist education allied with generic training programmes post-qualification as factors that lead to low application rates. 23 The reduction in medical staff numbers and publications across clinical biochemistry would suggest an increased risk of academic atrophy in the future. For clinicians the rate of recruitment to career training posts in chemical pathology/metabolic medicine has averaged 20% over the last decade. Work in other systems has identified that high profile research active individuals and departments have an increased ability to recruit junior staffing in the USA. 24 However, no correlation was observed in this study between either clinical scientist or medical recruitment and research productivity in the UK in chemical pathology. This is not surprising as neither scientific nor medical recruitment for training is linked to the academic productivity of the departments or regions. The presence of active research programmes is not used to assess the continuing suitability of designated training centres in contrast to the requirement for exposure to a diverse range of clinical specialties and service laboratory techniques. However, this finding does suggest a risk of technical obsolescence for trainees in the system as they are not being consistently exposed to leading research techniques that later translate to clinical service uses.
This audit shows that publishing research remains a minority interest in clinical biochemistry. A small and decreasing proportion of active individuals publish 90% of the work. The trend over the last decade seems to be towards a reduction in clinical scientist and especially medical research productivity which worsens with the years. Given the translation of early performance into later productivity and dependence of regional centres on lone individuals for their scientific output, further efforts need to be made to foster academic chemical pathology and to link training to translational science.
Footnotes
Declarations
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by William Simpson and Patrick Twomey.