
Abstract
Lesson
Consider life-threatening hyperkalaemia if the ECG shows high take-off with coved ST segment elevation and negative T wave in lead V1 superimposed on other ECG signs of hyperkalaemia and treat with calcium gluconate while waiting for blood chemistry results.
Case report
A 78-year-old patient presented with acute shortness of breath. She was too breathless to give a detailed history, though she did indicate on specific questioning that she had passed little urine in the previous week. Cardiac and respiratory examinations were normal. SpO2 was 98% on 8 l/min oxygen, with respiratory rate 20/min, heart rate 72/min and BP 160/70 mmHg. Her ECG (Figure 1) which was available before her blood chemistry showed tall T waves, loss of P wave, broad QRS complex together with high take-off >2 mm, coved ST segment elevation and T wave inversion in V1 (Brugada type 1 pattern). CXR showed clear lung fields.
Initial ECG when serum K was 9.5 mmol/l.
Suspecting hyperkalaemia, initial emergency treatment was with calcium gluconate 10 ml 10% IV, repeated twice, which led to narrowing of the QRS complex. Blood chemistry subsequently showed serum potassium 9.5 mmol/l with blood urea 72 mmol/l, serum creatinine 2200 µmol/l and H+ 120 nmol/l indicating advanced kidney injury and that her dyspnoea was likely due to acidosis. There were no recent blood results for comparison.
Subsequent treatment with dextrose and insulin, nebulised salbutamol and emergency dialysis lowered her serum potassium to 4.3 mmol/l. Her ECG had by this time returned to normal (Figure 2). Further investigations showed that the cause of her kidney injury was obstructive uropathy due to bilateral pelviureteric junction obstruction. We assumed this was a late presentation of an idiopathic pelviureteric junction obstruction as there was no evidence of stone or tumour on her scan. She received dialysis for six days, bilateral nephrostomies and then ureteric stents. When last seen at the clinic nine months after her initial presentation she was still feeling tired but otherwise well with serum potassium 3.9 mmol/l, blood urea 23.7 mmol/l and serum creatinine 545 µmol/l.
ECG following intravenous calcium, insulin, dextrose, nebulised salbutamol and emergency dialysis showing resolution of all changes. Serum K now 4.3 mmol/l.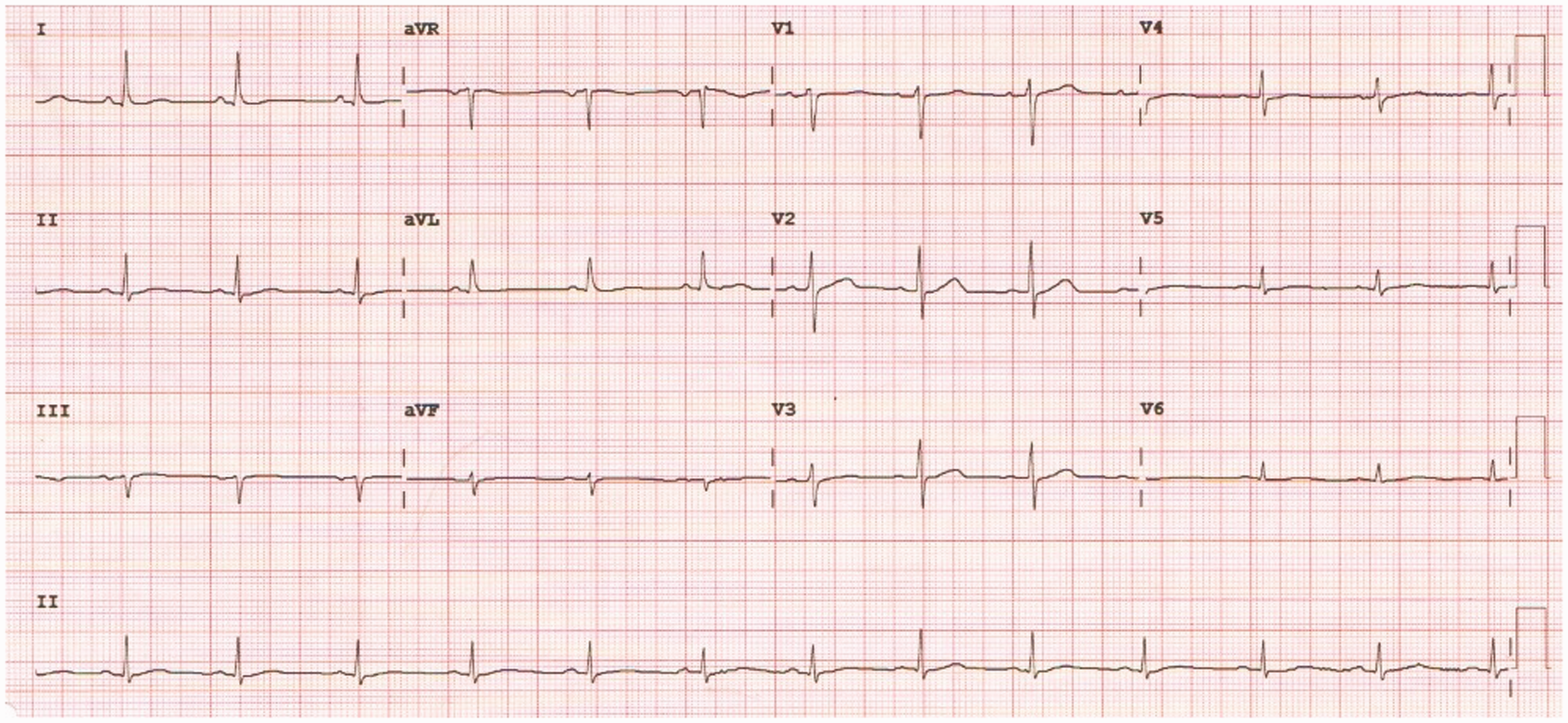
Discussion
Serious dysrhythmia is unlikely if serum potassium is less than 6 mmol/l, though risk depends not only on the level of potassium but also on the ECG changes and the likelihood that potassium will rise further. The sequence of changes is usually tall T waves then loss of P wave then broadening of the QRS complex before dysrhythmia which is usually asystole but can be ventricular fibrillation. 1 Our patient’s ECG demonstrated all of these changes and in addition a hyperkalaemic Brugada sign (high take-off > 2 mm with coved ST segment elevation and T wave inversion in lead V1). 2
Reviews of the treatment of hyperkalaemia generally start with the blood biochemistry before describing what should be done at different levels of serum potassium in the presence or absence of ECG changes. 3 This approach works well if the serum potassium is already known. In most emergency scenarios, however, a critically unwell patient is likely to have an ECG before the blood chemistry becomes available. Because the first clinical feature of hyperkalaemia may be sudden death it is important that doctors recognise the ECG features of hyperkalaemia and are confident enough to give intravenous calcium while waiting for the blood chemistry. The correct initial emergency treatment is calcium gluconate 10 ml 10% IV which can be repeated every 3–5 min until the QRS complex narrows. 3
Footnotes
Declarations
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by Oliver Lloyd.