
Abstract
Early diagnosis and treatment of endophthalmitis will optimise visual prognosis. Blood culture sensitivities should tailor antibiotic choice.
Background
Endophthalmitis is an ophthalmic emergency, resulting from intraocular infection. Most cases are exogenous with an external route of entry for organisms, secondary to trauma, surgery or infected cornea. Approximately 2–8% of cases are endogenous, a consequence of haematogenous spread of pathogens from a primary site of infection to intraocular tissue. 1 Causative pathogens identified include Staphylococcus aureus, Streptococcus pneumonia, Streptococcus agalactiae, Clostridium perfringens, Moraxella spp, Neissiera meningitides, Escherichia coli, Klebsiella spp, Serratia marcescens and Candida albicans.2,3 Presentation with a subretinal abscess is even rarer. It results from accumulation of microbial organisms in the subretinal space after travelling via the circulation to the choroid, Bruch’s membrane and retinal pigment epithelium. 4 Vitreous aspiration is used to confirm diagnosis. Imaging of ocular tissue using B-scans can be used to identify the extent of infection and any complications such as subretinal abscess. Early administration and treatment is associated with a favourable outcome.5,6
Case presentation
On 29 March 2016, a 41-year-old man presented to the acute medical admissions unit of a district general hospital complaining of a five-day history of lethargy, fatigue, reduced oral intake, reduced vision and pain in the left eye. He had a past medical history of chronic pancreatitis, pancreatic pseudocyst drainage, Whipple’s procedure, appendicectomy and vitamin D deficiency. Ocular history was unremarkable, with no history of trauma or ocular surgery. He was an independent man, usually mobile and self-caring.
Following a thorough history and examination, a full septic screen was completed as he showed signs of sepsis, which included a chest X-ray, urine dipstick, blood cultures and a CT brain scan. He was commenced on broad spectrum intravenous antibiotics on admission to treat sepsis of unknown origin as per antimicrobial formulary–gentamicin, metronidazole and amoxicillin. In addition, an urgent referral was made to ophthalmology and he was seen on the same day. On ocular examination, it was noted that his visual acuity was 6/15 OD and hand movements OS. Anterior segment examination of the left eye showed ciliary congestion, corneal haze, 4+ cells in the anterior chamber, 2 mm hypopyon and a poorly reactive pupil. Fundal view was very hazy and a poor red reflex was noted. Right eye examination was unremarkable. The patient was provisionally treated as an endogenous endophthalmitis with an urgent left intravitreal tap followed by injection of intravitreal vancomycin 1 mg/0.1 ml and ceftazidime 2.25 mg/0.1 ml. Post-operatively he was given topical antibiotics, steroid and cycloplegic drops.
One day following initial assessment, pain began to improve in the left eye. However, hypopyon was still present and there was no improvement in remaining examination findings including visual acuity. Thus, an additional injection of intravitreal vancomycin and ceftazidime was given two days after the first one. Vitreal cultures showed no growth but were positive for white cells. A B-scan was requested to visualise the posterior segment as fundal view remained hazy, which showed a dome shaped lesion at the posterior pole indicative of a subretinal abscess.
The patient was stepped down to oral antibiotics approximately a week following admission, despite a source of sepsis not being identified, as inflammatory markers were settling and the patient was improving clinically.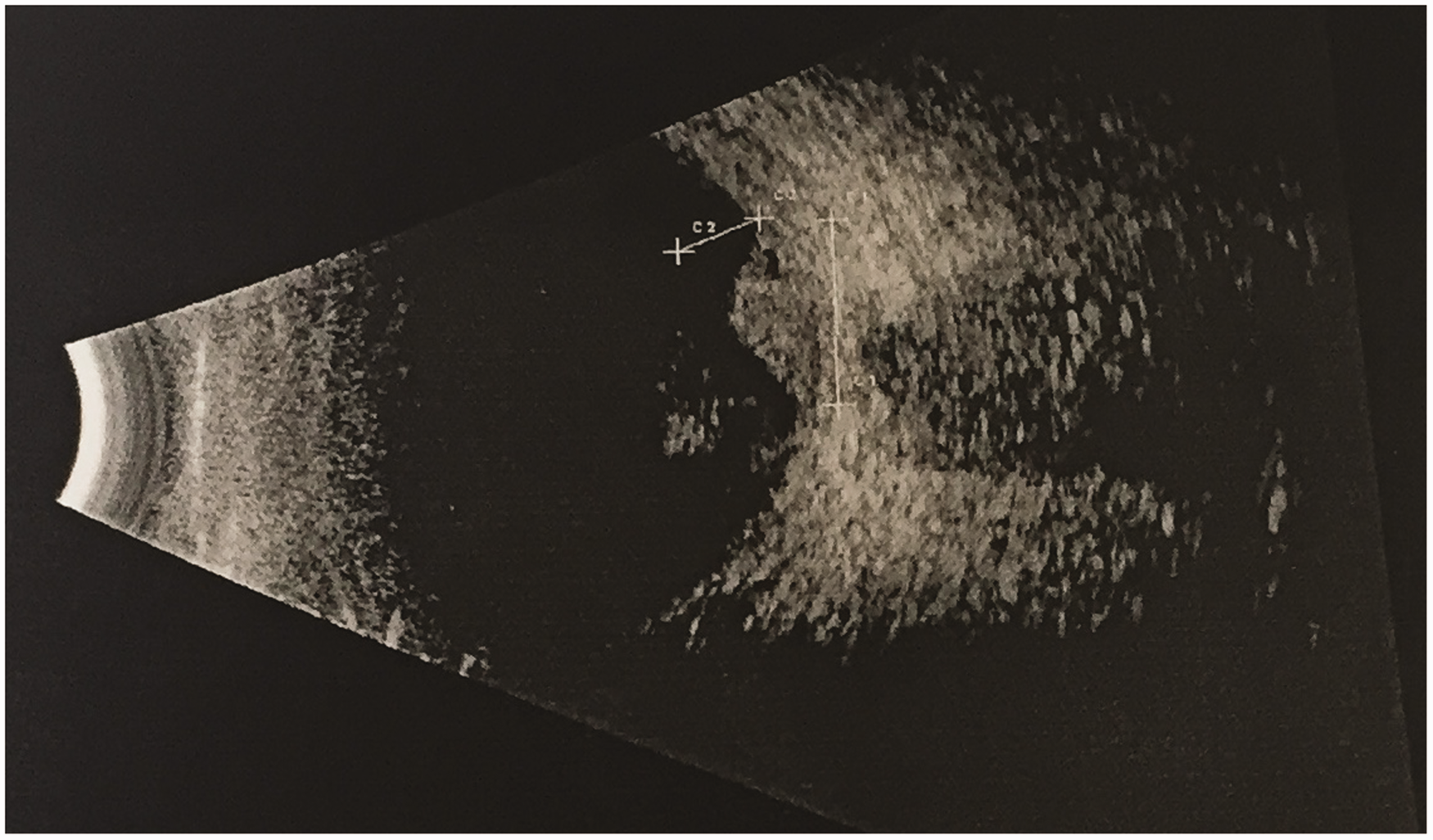
However, within 24 hours the patient deteriorated and an urgent CT abdomen and pelvis was requested. Imaging showed multiple splenic abscesses with few small pockets of retroperitoneal air suggestive of localised splenic abscess perforation, which is the likely origin of the infection seeding to the eye. A splenic abscess drain was placed by the surgeons and antibiotics were changed to linezolid, meropenem and fluconazole following results of the repeat blood cultures sensitivities which grew Proteus mirabilis, Enterococcus faecium and E. coli, reflective of the abdominal origin of infection.
Outcome and follow-up
Patient recovered well systemically with antibiotics and drainage of the splenic abscess. There was no improvement in vision in the left eye, however inflammation has settled. He continued the eye drops and was referred to the vireo retinal surgeons shortly after the second intravitreal injection to determine if a vitrectomy would be beneficial. It was concluded that as a result of retinal scarring he would not benefit from a vitrectomy so no further intervention was advised. He was discharged with a follow-up appointment in eye clinic with a B-scan to review the status of the subretinal abscess. Unfortunately, the patient passed away a few months later, following further hospital admissions for sepsis, bowel ischaemia and bowel obstruction.
Discussion
Subretinal abscess, a yellow-white lesion with haemorrhages in the overlying retina of the posterior fundus, is a rare presentation of endogenous endophthalmitis, accounting for 5% of cases. 3 The bacterial organism commonly associated with subretinal abscess is Nocardia, and is mostly seen in immunosuppressed patients.2,7 However, this gentleman’s blood cultures grew P. mirabilis, E. faecium and E. coli, organisms which have not previously been reported in cases of endogenous endophthalmitis complicated by subretinal abscess. Due to its rarity, there are no treatment guidelines available at present which specifically address the management of endophthalmitis complicated by subretinal abscess. However, there are individual case reports which have demonstrated beneficial outcomes with a combination of systemic and intravitreal antibiotics. In addition, vitrectomy and retinectomy may be considered in severe cases.8,9

Footnotes
Declarations
Funding
None declared
Ethics approval
Written informed consent for publication was obtained from the patient.
Guarantor
VM
Contributorship
VM wrote and completed the research for the case report. CS reviewed and edited it.
Acknowledgements
None
Provenance
Not commisisoned; peer-reviewed by Sudeshna Patra and R Ismail.