
Abstract
Renal artery pseudoaneurysm is a rare complication following renal interventional procedures or, although it may be spontaneous as described in this case. Clinicians should have a low threshold for early computer tomography (CT) imaging in cases of diagnostic uncertainty.
Case
History and physical examination
A 29-year-old man of Asian origin was admitted with constant abdominal pain localising to the right upper quadrant with no radiation. There was no history of fever, haematuria, diarrhoea, vomiting or trauma. He had no significant past medical or family history. He had been a lifelong non-smoker, was not on any regular medications and had no known drug allergies. On examination, his vital observations and chest examination were normal. His abdomen was soft on palpation and right upper quadrant tenderness was elicited with no signs of peritonism.
Investigations
Erect chest and abdominal radiographs were unremarkable. Serum biochemistry showed normal renal and liver function while full blood count showed leucocytosis (total white cell count 21.3 × 109/L) and normocytic anaemia (haemoglobin concentration 10.2 g/dL). Urine dipstick showed trace of protein only. Computed tomography (CT) scan (contrast enhanced) of the abdomen and pelvis showed a mixed attenuation lesion associated with a large perinephric haematoma (Figures 1 and 2). The patient was initiated on intravenous antibiotics.
Coronal reconstruction of the contrast enhanced CT showing the mixed attenuation right lower kidney lesion and a large adjacent perinephric haematoma. Axial reconstruction of CT scan illustrated in Figure 1.

Initial management
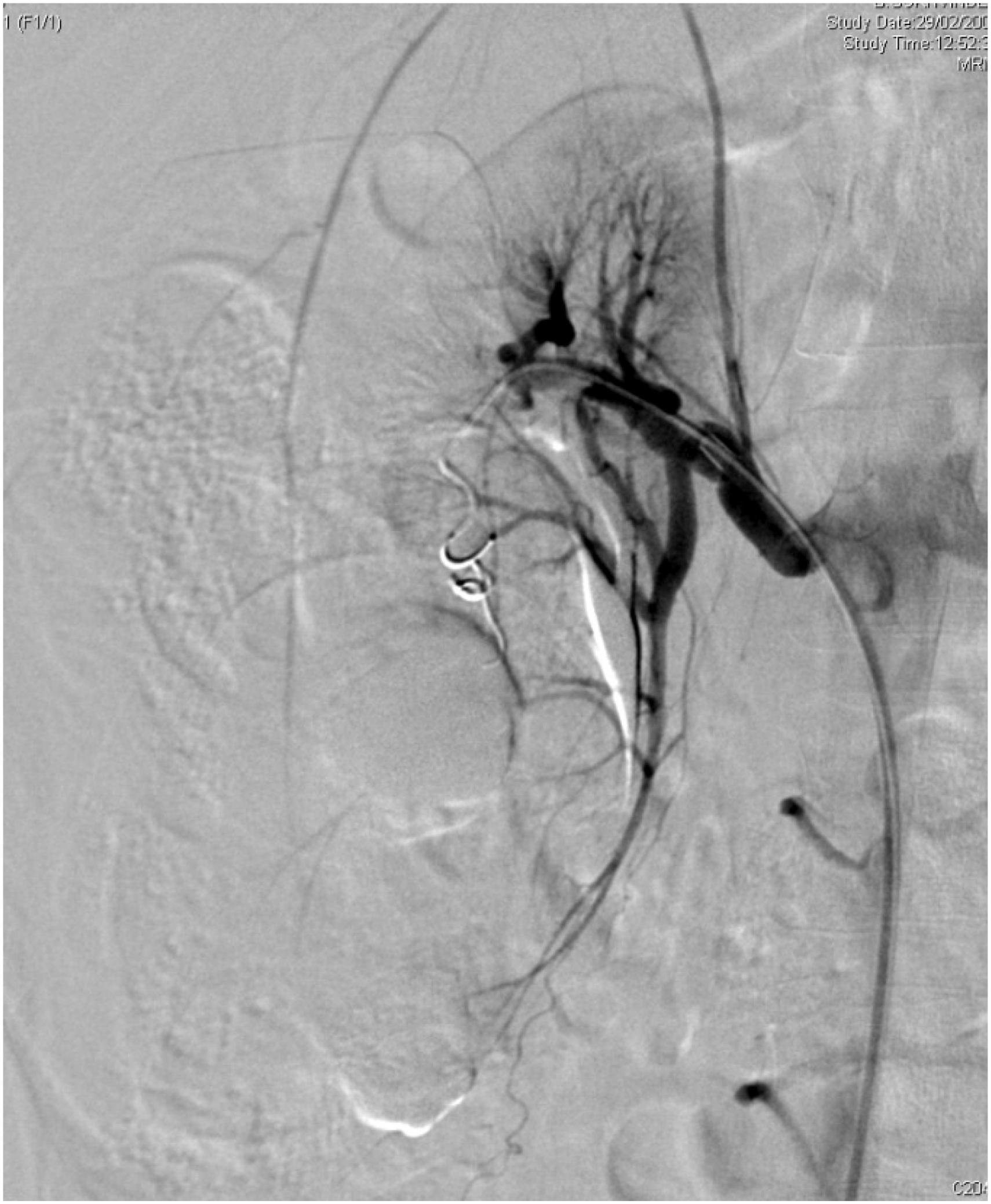
After 48 h, the patient remained apyrexial and pain was well controlled while inflammatory markers improved. Four days following admission, the patient experienced severe acute onset right upper abdominal pain. Repeat blood tests showed a significant drop in the haemoglobin concentration to 6.3 g/dL. After resuscitation and blood transfusion, a repeat CT scan (contrast enhanced) showed a pseudoaneurysm in the inferior branch of the right renal artery (Figure 3). The patient immediately underwent selective renal angiography confirming the presence of a bleeding 5.1 ×3.7 cm right renal artery pseudoaneurysm which was embolised successfully with two platinum coils (Figures 4 to 6).
Three-dimensional CT reconstruction of the abdominal aorta and the renal vessels. Note the pseudoaneurysm in the right lower renal pole (asterisk). Renal arteriogram immediately prior to pseudoaneurysm embolisation. Arteriogram with no subtraction clearly shows the pseudoaneurysm amidst the right kidney lower moiety haematoma compressing and medially displacing the collecting system. Final digital subtraction angiogram after the placement of the second platinum coil shows complete exclusion of the pseudoaneurysm with redistribution of the blood circulation and consequent visualisation of the renal capsule branch with haematoma-related renal capsule distension.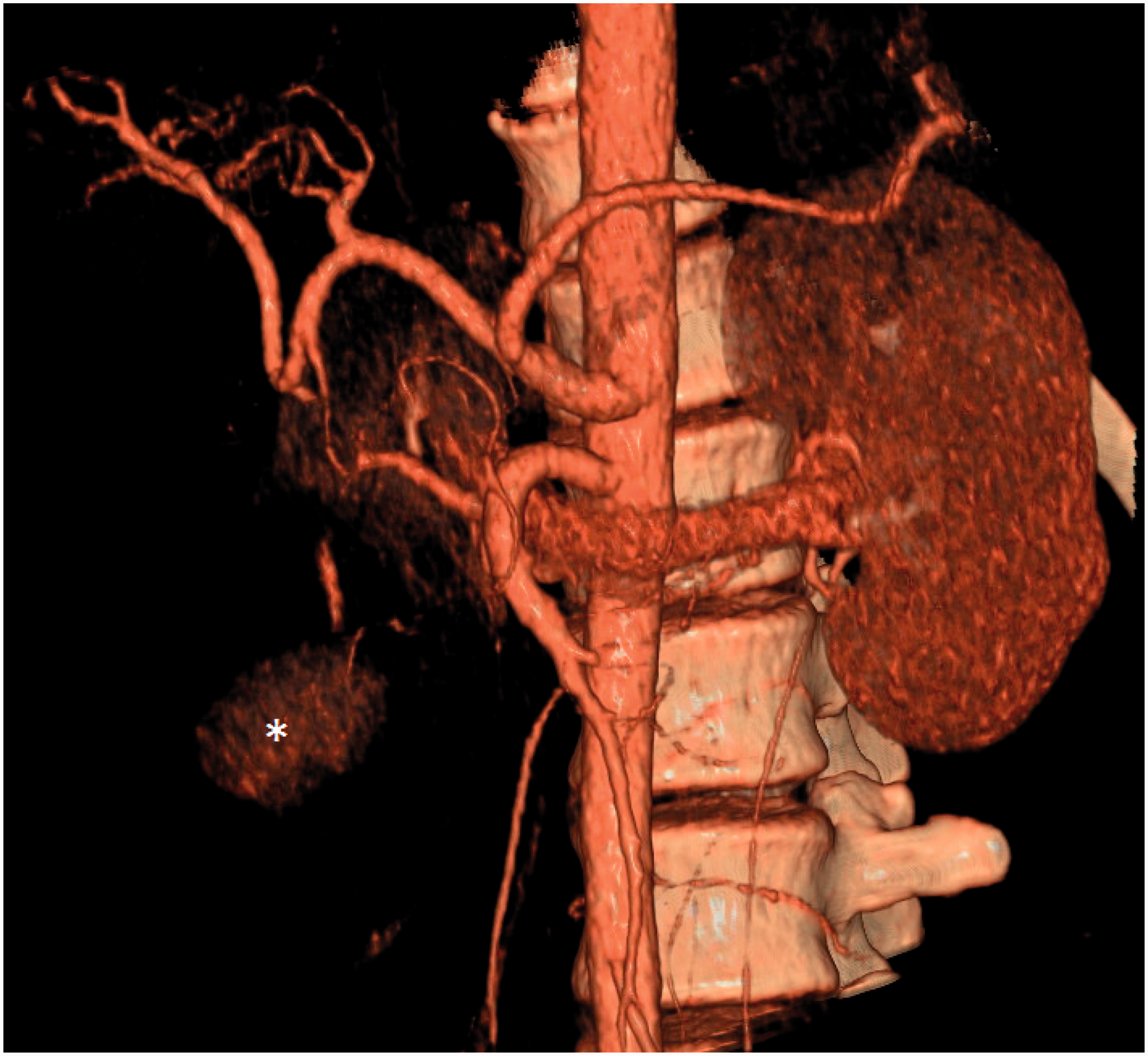


Subsequent management and follow-up
The patient was monitored for further 48 h during which his pain improved, haemoglobin concentration remained stable and he was discharged from hospital. There was no evidence of undiagnosed hypertension as he remained normotensive prior to embolisation and during the 48 h period following the procedure. There was no history of familial hypercholesterolaemia and his lipid profile was within normal range. There was no evidence of vascular calcifications on CT scan to suggest severe atherosclerosis. An magnetic resonance imaging scan of his head did not show any vascular abnormalities. Anti-nuclear antibody and anti-neutrophil cytoplasmic antibody tests were negative. Repeat CT scan at three months showed significant reduction in the size of the perinephric haematoma while the CT scan and the ultrasound at seven months and 19 months, respectively (Figures 7 and 8), showed almost complete resolution. Full blood count and renal function profile at 12 months were normal (haemoglobin 15.5 g/dL, serum creatinine 101 µmol/L, estimated glomerular filtration rate 75 mL/min/1.73 m2). Both the follow-up CT and ultrasound showed good recovery of the right kidney with good residual renal parenchymal reserve. The patient remained asymptomatic with normal blood pressure and was discharged to his GP.
CT (contrast enhanced) at 7 months following the endovascular procedure showing good perfusion of the right kidney residue. Ultrasound scan (USS) at 19 months following endovascular procedure showing almost complete resolution of the right renal parenchymal changes.

Discussion
Arterial aneurysms can be divided into true or false aneurysms (pseudoaneurysm). A true aneurysm involves all arterial wall layers while a pseudoaneurysm is a haematoma contained by the surrounding structures outside the vessel wall. Renal artery aneurysm is rare and was first described by Rouppe. 1 An aneurysm of the renal artery is defined as a segment of the artery with double the diameter of the normal. They occur in both men and women but the incidence of rupture is higher in women, especially if they are pregnant. Renal artery pseudoaneurysm has been reported as a result of blunt trauma 2 or deceleration 3 injury and following urological interventions such as partial nephrectomy, 4 percutaneous nephrolithotomy, 5 renal biopsy, 6 ureterorenoscopy for laser lithotripsy 7 and following renal transplantation. 8 Our case was unusual as there was no predisposing event associated with the renal artery pseudoaneurysm and subsequent rupture.
Renal artery aneurysms can be classified into four basic types: saccular, fusiform, dissecting and intrarenal with the saccular type constituting approximately 75% of all aneurysms. 9 Secondary atherosclerotic degeneration or intramural calcification is not uncommon. Presence of a ring-like calcification on plain abdominal radiography should raise the suspicion for diagnosis of renal artery pseudoaneurysm as these are present in approximately half of cases. 10 Incompletely calcified saccular aneurysms can be soft and thin between calcified zones, therefore these are at high risk of spontaneous rupture or eroding into vein to form an arteriovenous malformation. 10 Symptoms can include flank pain, hypertension, haematuria, rupture, ischemia or obstructive uropathy.
Renal artery aneurysms can be diagnosed by various imaging modalities including duplex ultrasound, CT scan, MR angiography and arteriography. Arteriography is useful in delineating anatomy but is used only in cases requiring intervention due to its invasive nature. In our case, the CT scan raised the possibility of right renal artery aneurysm which was confirmed by angiography.
Treatment options include conservative, minimally invasive and open surgical options. Well-calcified renal arterial aneurysms that are asymptomatic or < 2 cm can be managed conservatively with serial imaging to ensure no change in size. In iatrogenic injuries where conservative management fails, transarterial embolisation is recommended followed by repeat intervention if required. 11 In the elective setting, surgical intervention for renal artery aneurysm is indicated in symptomatic patients (pain or haematuria), hypertension or renal ischaemia, dissecting aneurysm, women of child-bearing age who are likely to conceive, radiographic evidence of aneurysm expansion or aneurysm containing thrombus detectable on angiography with evidence of distal embolisation. 10 Minimally invasive/endovascular interventions include balloon occlusion, vascular stenting or embolisation with detachable coils/balls or gel foam. The surgical methods are open repair, angioplasty, bypass of the aneurysm and nephrectomy. The endovascular embolisation with gel foam/platinum coils is now the treatment of choice and helps to control or prevent bleeding in > 80% of patients. 12
Conclusion
Renal artery pseudoaneurysms are rare but are well described following urological or radiological interventions to the kidney or as a result of trauma. Rupture of a renal aneurysm can cause catastrophic blood loss but can be treated, either by minimally invasive or open methods. In patients who present with renal angle pain and unexplained blood loss, especially with history of previous urological interventions, the differential diagnosis of renal artery pseudoaneurysm should be considered. To the best of our knowledge this is the first report of a spontaneous renal artery pseudoaneurysm rupture with no predisposing event and was managed by selective arteriography and embolisation using platinum coils.
Footnotes
Declarations
Funding
None declared.
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by Muhammad Khan.