
Abstract
Lesson
Computed tomography scanning could be safely used in later pregnancy to aid diagnosis and target management of the acute abdomen.
Introduction
Dermoid cysts have been described as embryological cysts that develop along the lines of fusion with trapped ectodermal elements hence the macroscopic presence of hair, nails, teeth etc. They are usually unilateral, but bilateral cysts have also been described in women between the ages of 15 to 40 with no particular racial predilection.1,2 These cystic tumours have the potential to grow, become inflamed, tort, strangulate, perforate and at times form fistulous tracts with surrounding viscera. Hence patients can present with variable symptoms based on organ involvement.3,4 Usually Dermoid cysts < 6cm are not expected to change size in pregnancy and complications are very rare.5 Although described as being epidemiologically rare, their association with the ovary is described as a benign cystic teratoma that have on occasion turned malignant.6 A literature review was performed using MeSH terms cystic, teratoma, ovary and pregnancy that revealed 61 results from which only 35 were found to be relevant. This is the first case report of a spontaneous rupture of a cystic teratoma of the ovary leading to diffuse peritonitis in the third trimester.
A 33-year-old, 25-week pregnant patient with three previous live births presented with acute onset of diffuse abdominal pain without any abnormal vaginal discharge to the triage around midnight. Physical examination revealed a blood pressure of 110/60 mm Hg and pulse of 110/min accompanied with diffuse abdominal tenderness and a normal uterine height for gestation. The foetal cardiotocography was within normal limits and blood tests revealed a white cell count of 2.8 × 109/L, neutrophil count of 1.6 × 109/L, platelet count of 148 × 109/L and a C-reactive protein of 122. The urea, electrolytes, liver function tests and amylase were within normal limits. Blood gas showed metabolic acidosis with a pH of 7.2 and a base excess of 18. The urine dip stick test was unremarkable. The differential diagnosis included appendicitis, cholecystitis, pancreatitis, mesenteric thrombosis, visceral perforation, uterine rupture, placental abruption and adnexal torsion. After administration of intravenous fluids and broad-spectrum antibiotics, an ultrasound was performed to assess the viability of the foetus and image the pelvic and abdominal viscera for likely causes. A pelvic mass with extensive free fluid was identified in the left adnexa (Figures 1, 2 and 3). Fluid was aspirated for biochemistry, cytology and microbiology. By this time, the patient’s condition deteriorated further and having failed to identify an obvious obstetric or gynaecological cause for her condition the on-call surgical team was contacted and a decision was made to proceed to an emergency laparoscopy.
At laparoscopy, there was widespread murky fluid in all four quadrants associated with fibrinous exudate on the small bowel. There was no evidence of any gastrointestinal pathology as described above. The pelvic mass identified on ultrasound failed to appear to be the source of sepsis at preliminary examination but on further inspection there was evidence of a cystic structure with some boggy areas. The cause for murky free fluid remained unclear hence a decision was made to convert the operation to a laparotomy. It quickly became evident that this cystic structure had torted along with the left ovary, strangulated and ruptured
The fallopian tube, ovary and the cystic teratoma were excised en bloc and peritoneal lavage carried out. The patient was transferred to the high-dependency unit intubated. Unfortunately, the foetus did not survive and was delivered subsequently by uterine induction. The patient had a prolonged stay complicated by chest infection, pleural effusion and abdominal collections which needed percutaneous drainage.
Discussion
The management of an acute abdomen from non-obstetric causes during pregnancy poses a challenging scenario for the on-call general surgeon. Limitations of readily available safe radiological tests that could aid diagnosis and their interpretation is an additional challenge.
Apart from trauma, computed tomography scanning is rarely used to assess the acute abdomen due to the perceived risk posed to the developing foetus in both the short and long term. In a recent position statement, the American College of obstetricians and gynaecology has stated that the radiation doses commonly in use for computed tomography scanning are well below the 50 mGy7,8 safety limit and can be used safely in select situations. This evidence should spark discussion with the radiologist to help target treatment.
Ultrasound scanning is useful only for focused assessment. Magnetic resonance imaging scanning during pregnancy is considered safe but rarely performed due to limitations of availability out of hours and often requiring specialist reporting.
This patient proceeded to theatre without awaiting further radiological investigation due to clinical deterioration. Laparoscopy was chosen over laparotomy to aid diagnosis and potentially treat, as the surgeon was competent in dealing with common gastrointestinal pathology laparoscopically. However, difficulty in assessing the gravid pelvis should lead to a laparotomy as was the case in this patient.
Ensuring viability of the foetus after surgical treatment is often challenging, and in this scenario, maternal safety took priority. Although the foetus could be considered for premature delivery at 24 weeks, it would have added further physiological burden to the patient. Hence the obstetricians opted to monitor the pregnancy in the absence of foetal distress and delay delivery until further improvement in maternal health. The post-operative monitoring of foetal distress in the setting of a recent laparotomy is as challenging as the timing and modality adopted for delivery.
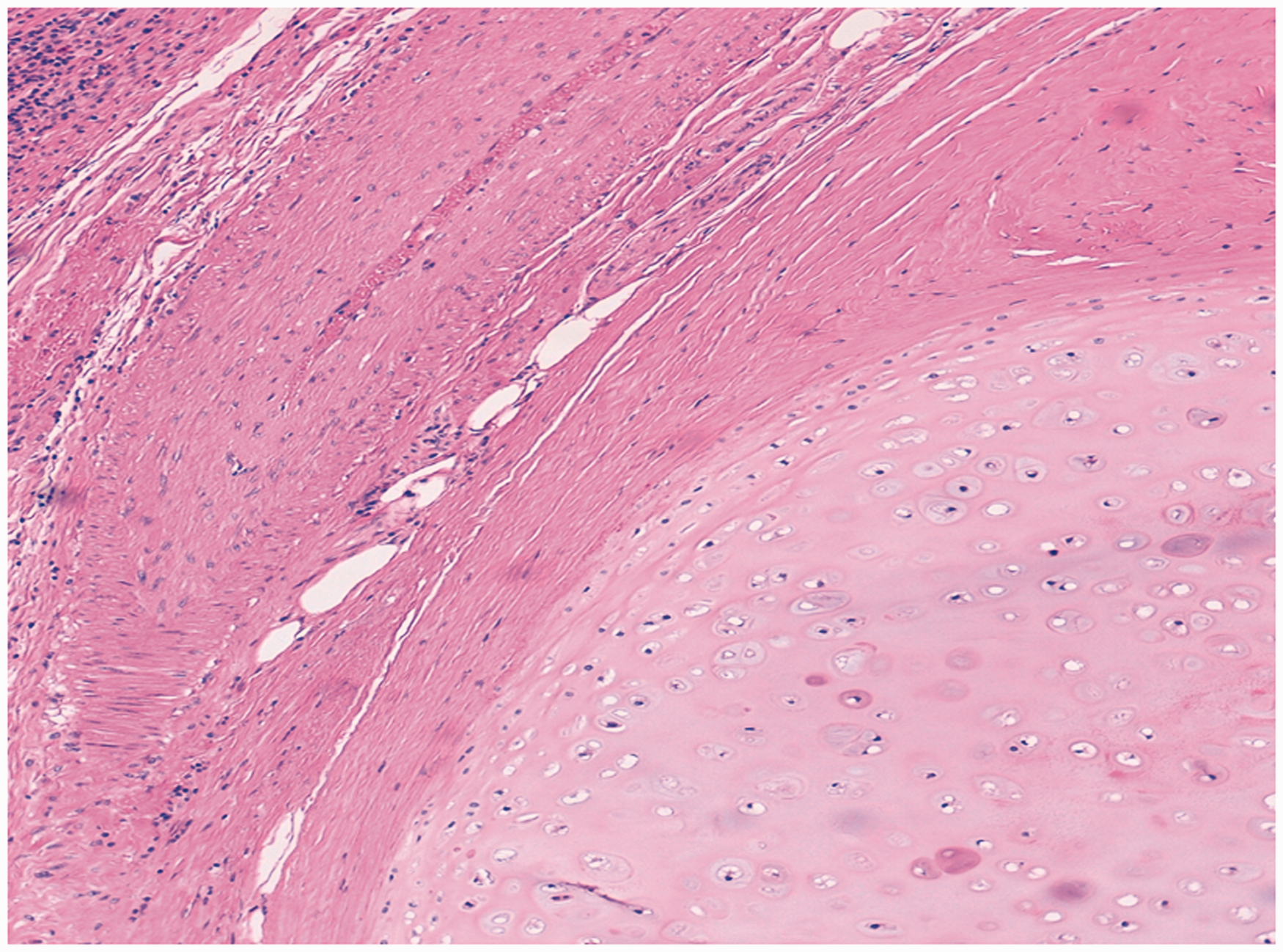
Ultrasound of left ovarian complex cyst. Showing stratified epithelium. Keratinocytes and sebaceous glands.

Footnotes
Declarations
Acknowledgements
none.
Provenance
Not commissioned; peer-reviewed by Jonathan Baum.