
Abstract
Objective
Major changes in the design and delivery of clinical academic training in the United Kingdom have occurred yet there has been little exploration of the perceptions of integrated clinic academic trainees or educators. We obtained the views of a range of key stakeholders involved in clinical academic training in the East Midlands.
Design
A qualitative study with inductive iterative thematic content analysis of findings from trainee surveys and facilitated focus groups.
Setting
The East Midlands School of Clinical Academic Training.
Participants
Integrated Clinical Academic Trainees, clinical and academic educators involved in clinical academic training.
Main outcome measures
The experience, opinions and beliefs of key stakeholders about barriers and enablers in the delivery of clinical academic training.
Results
We identified key themes many shared by both trainees and educators. These highlighted issues in the systems and process of the integrated academic pathways, career pathways, supervision and support, the assessment process and the balance between clinical and academic training.
Conclusions
Our findings help inform the future development of integrated academic training programmes.
Background
The East Midlands School of Clinical Academic Training is responsible for approximately 80 Clinical Academic Trainees (typically 16–20 and 6–7 National Institute for Health Research-funded ACFs and ACLs per year and similar numbers of locally funded matched posts) working in close partnership with the Universities of Leicester and Nottingham and local National Health Service trusts. We recognise the importance of a firm understanding of possible barriers and enablers in delivering successful integrated clinical academic training programmes and to increasing overall participation in academic training. The relative infancy of National Institute for Health Research integrated training programmes and the annual General Medical Council trainee survey's lack of reporting on findings specific to academic posts or comparisons between clinical and academic training limit the information available in this field. We therefore designed a qualitative study which aimed to explore and understand the perspectives of key stakeholders on the delivery of successful Integrated Clinical Academic Training Programmes and the support of academic training across the region.
Methods
We explored the perceptions, experiences, concerns and suggestions of clinical academic trainees, trainers and other key stakeholders by running a series of moderated focus groups and an online trainee survey.
Trainee survey
A bespoke online survey was designed to assess trainees’ views of the quality, barriers and enablers of all aspects of their training. The survey questions were agreed and piloted by a small group of trainers and trainees to confirm the survey feasibility. Trainees of all grades, enrolled in a National Institute for Health Research or locally funded Integrated Clinical Academic Training, were invited to participate anonymously via a link to the online survey. The survey was repeated one year later with modification of some questions in light of previous responses (Appendix 1).
Focus groups
Participants: Educator focus groups
We held three focus groups of 6–8 educators, facilitated by the same experienced moderator. A range of clinical and academic educators in all specialities across the region were invited to participate: clinical educational supervisors, academic supervisors, clinical training programme directors, TPDs, heads of university departments, Trust directors of medical education, university directors of clinical academic training and associate postgraduate deans. Participants were allocated to the three groups to best allow sufficient heterogeneity to promote discussion while maximising the opportunity for equal contribution.
Participants: Trainee focus group
We held a single focus group of seven integrated clinical academic trainees of different grades and specialities working across the region to follow up the results of the trainee survey. Since the information gathered from this focus group did not provide any additional themes we felt that further focus groups with trainees were not required.
Procedure
The Training Programme Director (RHG) or the Head of School (JB) opened each session with an overview of the study aims, then left to encourage honest discussion. The facilitator explored a framework of themes (Appendix 2) using a series of open questions with further probes as needed. Detailed contemporaneous notes were taken and anonymised although discussions were not recorded. A debrief meeting was held between the Training Programme Director (RHG) and facilitator (VE) reviewed the detailed notes alongside the facilitator’s own field notes (including, for example, the degree of within group consensus or dissent). Notes taken during the debrief were verified by the facilitator and included in the analysis.
Analysis
An inductive approach was adopted initiated by open coding during the facilitator debrief. Codes were allowed to emerge from the data to minimise pre-emptive bias. A process of ‘constant comparison’ of within-group data followed, and was repeated until all concepts had been recognised and categorised. This was repeated iteratively for each of the focus groups, and for the trainee survey free text responses, and the findings assimilated using further constant comparison of between-group data. On completion the list of categories was scrutinised and reduced either by omission (if they were not relevant to the study aims) or amalgamation. Finally categories were integrated and refined into common themes to complete a thematic content analysis of the data. Comparisons were made between emergent themes from the two types of focus groups and from the results of the trainee surveys.1,2
Results
A number of themes emerged relating to enablers and barriers to excellence in clinical academic training and to the role of the School of Integrated Clinical Academic Training.
Systems and processes
The process is problematic at all stages – very difficult to understand and priorities are unclear. (Academic Supervisor)
There was concern among both trainees and trainers that the processes involved in recruiting to and delivering National Institute for Health Research Integrated Clinical Academic training programmes were complex, rigid and poorly understood. It was generally felt that having academic posts was desirable since they came with their own funding and had the potential to attract high-calibre trainees from outside of the region. However some trainers, particularly academic supervisors and university representatives, expressed the view that opportunities to recruit to posts were not always transparent or consistent which lead to a sense of frustration and injustice. It was also felt that opportunities to recruit to Academic Clinical Fellow and Academic Clinical Lecturer posts did not always align to local priorities, either academic or clinical. It was recognised that tensions between the priorities of university departments, clinical academics and National Health Service employed supervisors could influence the allocation of academic training opportunities. Trainees reported frustration that their roles were not always understood or valued either by university departments or by clinical teams. Better communication between hospital trusts and universities and between clinical and academic teams was described as a key priority.
Career pathways
There should be rigorous assessments to facilitate flexible exits – we need to think about honourable escape routes for those not suited to continue an academic career and recognise that the skills they have acquired are useful in their own right. (Academic Supervisor)
Trainee survey responses and information collected at all the focus groups raised considerable anxieties about career pathways for future clinical academics in the face of a changing health service and reconfiguration of postgraduate medical training. Educators believed that it was crucial to recruit potential academics very early on in their careers, even at undergraduate level, and to focus on long-term planning, both for individual trainees and for the management of both the academic and clinical programme. One striking difficulty mentioned by several participants was an apparent disconnect between academic foundation programmes and the rest of the academic training pathway. This was described as a major threat to the retention of potentially excellent local academic trainees. Indeed some respondents to the online trainee survey stated that lack of support and integration into the wider academic community during academic foundation placements had led them to look elsewhere for subsequent training.
Trainees worried that academic career pathways were inflexible, with bottlenecks at various stages hindering their progression, a concern that was shared by many of the educators. There was a general perception that trainees who experience delays in progression through the pathway or reverted to purely clinical training (e.g. on completion of an academic clinical fellowship programme) had failed to realise their potential. Given the difficulties in obtaining personal fellowships to complete a higher degree (an entry requirement to an Academic Clinical Lecturer post) this was a significant source of stress for academic trainees who were generally considered to be ‘high fliers’ with no previous experience of ‘failure’. Furthermore, some educators felt that this may even prevent some talented candidates from considering an academic career, since failure to progress through an academic pathway may be seen more negatively than not having embarked on it in the first place. Increased investment at the key transition points, particularly improved funding for fellowships to bridge the gap between Academic Clinical Fellow and Academic Clinical Lecturer posts, was felt to be crucial to overcome these concerns.
The rigid structure of Academic Clinical Lecturer (ACL) posts was raised as a particular issue. Strict entry requirements (unlikely to be achieved until the latter stages of clinical training) combined with a requirement to relinquish the post on completion of clinical training led to the belief that Academic Clinical Lecturer posts often provided insufficient time to maximise the chances of obtaining a Clinician Scientist Fellowship. This was felt to be particularly unfortunate given the competitive nature of these awards and the lack of alternative opportunities for transition to a senior academic position. Some educators including clinical and academic supervisors and training programme directors expressed a lack of confidence in their ability to provide accurate careers advice due to limited understanding of the options and insufficient information regarding alternative ‘exit points’. This was reflected by trainees’ responses with several identifying careers advice as an area for improvement.
Some educators were concerned about the rates of attrition, which were considered higher at earlier stages in the pathway, and raised the possibility that this was due to inappropriate selection and recruitment of Academic Clinical Fellows.
Comments were raised about the difficulty in completing both clinical and academic training for doctors with caring responsibilities. It was suggested that the School should be closely linked to the Athena Swan programme to facilitate improvement.
Supervision and support
The quality and commitment of supervisors is crucial as is the need for well thought out projects – finding the right project can be quite a skill. (Educator)
It was recognised by both educators and trainees that academic supervision can be challenging and requires different skills than those required by clinical supervisors. The identification of suitable projects which are both relevant and feasible for clinical academic trainees was said to require particular expertise which was not always evident.
Considerable variation in the availability and quality of academic supervision was raised during the focus group and highlighted by a few trainees completing the survey. One potential explanation for this was a lack of clear guidelines of the roles and responsibilities for the various levels of supervision necessitated by these integrated programmes. The particular challenges faced by integrated clinical academic trainees sometimes meant they felt isolated and they were keen to explore options for mentoring, peer and pastoral support. There was some frustration that fellow academics did not offer guidance unless they shared common research interests. Educators also recognised variation in the experience and commitment of academic supervisors and suggested that sharing areas of best practice in academic supervision may help to drive up standards. Likewise it was recognised that clinical supervisors were not always positive about academic training which sometimes caused tension.
Assessment procedures
Clinical supervisors would recommend clarification from academic supervisors and vice versa. I feel involving clinical and academic supervisors/TPDs in both ARCPs for academic trainees would benefit us immensely. (Academic Clinical Lecturer)
The one area that raised much more concern for trainees than for their supervisors and educators was the assessment process. Trainers did comment on the need for rigorous process of assessment, particularly to ensure that clinical competences were maintained during periods of reduced clinical exposure and to ensure that trainees knew what was expected of them at each stage: ‘Some trainees appear clueless’ (Training Programme Director). Trainees also raised the issue that they were not always given clear expectations and they found this stressful.
The other major area of concern over the assessment process for trainees was the lack of understanding of Annual Review of Competence Progression panels and the lack of communication between clinical and academic supervisors about their progress. Trainees recognised that they could take the initiative by maintaining regular contact with their TPDs and helping to facilitate communication between supervisors. The Annual Review of Competence Progression panels have often failed to understand what I am trying to do however the program directors have been able to direct the panels. I would suggest that all academic trainees are encouraged to develop a good working relationship with their program directors and not just leave this to a yearly Annual Review of Competence Progression feedback session.
The balance between clinical and academic training
I am simultaneously disappointed and impressed with myself. (Academic Clinical Fellow commenting on how they manage the demands of the role)
In parallel with the strategic tensions between clinical and academic departments, there was universal recognition that achieving a working balance between the competing yet equally important demands of clinical and academic training was particularly difficult. It was acknowledged that the various supervisors did not always appreciate this. It was suggested that this may be a particular issue where trainers had not previously been exposed to integrated academic training programmes and therefore may not understand them. Trainees felt that they had to be highly motivated to reach their potential given the heavy workload. There were very practical concerns about the delivery of clinical duties from the staffing of on-call rotas to the tension of being called away from research labs to acute clinical emergencies. It was felt by educators that academic trainees, particularly early in their career, often felt embarrassed or guilty if they were not always seen to be ‘on the shop floor’. This worry was further exacerbated by a shortage of clinical staff; very many trainees reported that failures to recruit to clinical posts leaving gaps on rotas made a significant impact on what was expected from them. Trainees commented that they were just about able to manage the challenges of their dual role until they experienced difficulties that were out of their control such as covering for colleagues’ absences.
Trainees also reported their perceptions of an academic culture where failure to respond to email messages immediately may be seen negatively as a neglect of duty, making some feel as though they were ‘on duty’ 24 hours a day.
It was suggested that a shift in opinion was needed to improve the credibility of these posts among clinical supervisors and peers. A limited understanding of the roles and responsibilities of academic trainees among administrative staff was also highlighted. Some educators questioned whether it was possible to successfully achieve all the required clinical competences without an extension to training; this was considered a particular issue for craft specialities.
Discussion
A series of commentaries in the early 2000s highlighted the risks facing the advancement of healthcare due to a decline in academic medicine across Europe.3–6 This led to the publication of the Walport report in 2005 7 which paved the way for the development of the National Institute for Health Research-integrated clinical academic training programmes 8 as the best chance of reversing the decline in clinical academic medicine in the UK. The aim of our study was to ascertain the views and experiences of trainees participating in, and educators delivering, these programmes. We believe that our study provides valuable insights into areas for development and some good practice and is important since limited work has been done to address the impact of the development of integrated clinical academic pathways. While participants in our study clearly valued attempts at developing transparent, structured and carefully governed integrated training programmes, concerns were raised across groups about the flexibility of entry into and exit from academic training, the balance between clinical and academic commitments and the opportunities for career progression on completion of training. This suggests that more work is still needed to fully overcome the key deterrents to a clinical academic career described by Walport. The Walport 10th Anniversary Symposium 9 rejected the need for a further formal review of integrated academic training but accepted that a number of important issues remained, recommending that work be done to identify areas of concern along with the dissemination of aspects of good practice. We hope that our findings may usefully contribute to this work. Our results should help in planning the development of our educator faculty, encourage the development of tools by which we can assess and benchmark the quality of academic supervision and raise awareness of the challenges of combined clinical and academic training. In the light of the new junior doctors’ contract which emphasises the need for effective job planning to include educational time, there is an even more pressing requirement to increase the understanding of the issues facing this group of doctors. The Guardians of safe working, for example, will need a good understanding of interrelationships between the academic and clinical aspects in academic training.
There are little available data in the public domain with which to compare our findings. The Medical Research Council, in collaboration with the Academy of Medical Sciences, British Heart Foundation, Cancer Research UK, National Institute for Health Research and Wellcome Trust published a qualitative review of enablers and barriers to progression in early career clinical academics. 10
This review reported some similarities and some differences to our findings, possibly due to differences in aims and scope. In contrast to our study, the cross-funder review recruited participants who had applied for either a Clinician Scientist Fellowship or a Research Training Fellowship, both of which predate and are distinct from the National Institute for Health Research-integrated academic training scheme. While our study had a much narrower focus, common themes did emerge. The cross-funded study supported the importance of developing an academic interest at an early stage. While early selection for academic training was also highlighted by our findings, there are potential disadvantages to this approach which warrant discussion. It may be difficult to accurately assess the academic potential of trainees at such an early stage in their clinical career and, as one senior educator warned, those trainees who develop academic motivation later in their careers may be effectively excluded. The review analysed the career progression of academics finding that despite failing to obtain clinician scientist or senior fellowship awards, most academic trainees were still active in research. This supports the concern raised among our study participants about the need for alternative ‘exit points’ along the pathway – failure to complete the entire clinical academic training pathway does not appear to predict those who do not demonstrate activity in research longer term. Whether their greater interest continues, and influences either their clinical practice, their support of research and their advocacy of academic training, is not known.
The review also highlighted the problems of working across different organisations, the difficult balance between clinical and academic commitments and the inconsistencies in the level of academic support. Our findings of perceived enablers to clinical academic training closely reflected those reported in the cross-funded study including improvements in structures and processes, support and mentoring, better integration between clinical and academic departments and clarity and flexibility in career pathways. The significant challenges of completing both clinical and academic training alongside the desire for more control and flexibility in career progression identified by our work suggest that it may be time to debate the value of extending overall training time for this group.
Our study has limitations. While we opened the survey to all eligible trainees and invited wide ranges of educators and trainees to focus groups, those participating may have engaged because of wanting to express a particular view leading to a degree of selection bias. The similarity between our findings and those in the cross-funded review suggests this was not a major concern. We did not directly transcribe respondents’ comments to facilitate the flow of discussion, anonymity and to focus on core concepts. We recognise the limitations to this approach and that we may have therefore missed particular nuances or applied our own interpretations of what was said. We cannot be sure that our findings could be generalised to other areas where integrated clinical academic training occurs since the relationships between clinical services, academics and universities are likely to be unique, often based on historical contexts. Nevertheless, we found no major differences in any of the key themes between trainees linked to the Universities of Nottingham or Leicester.
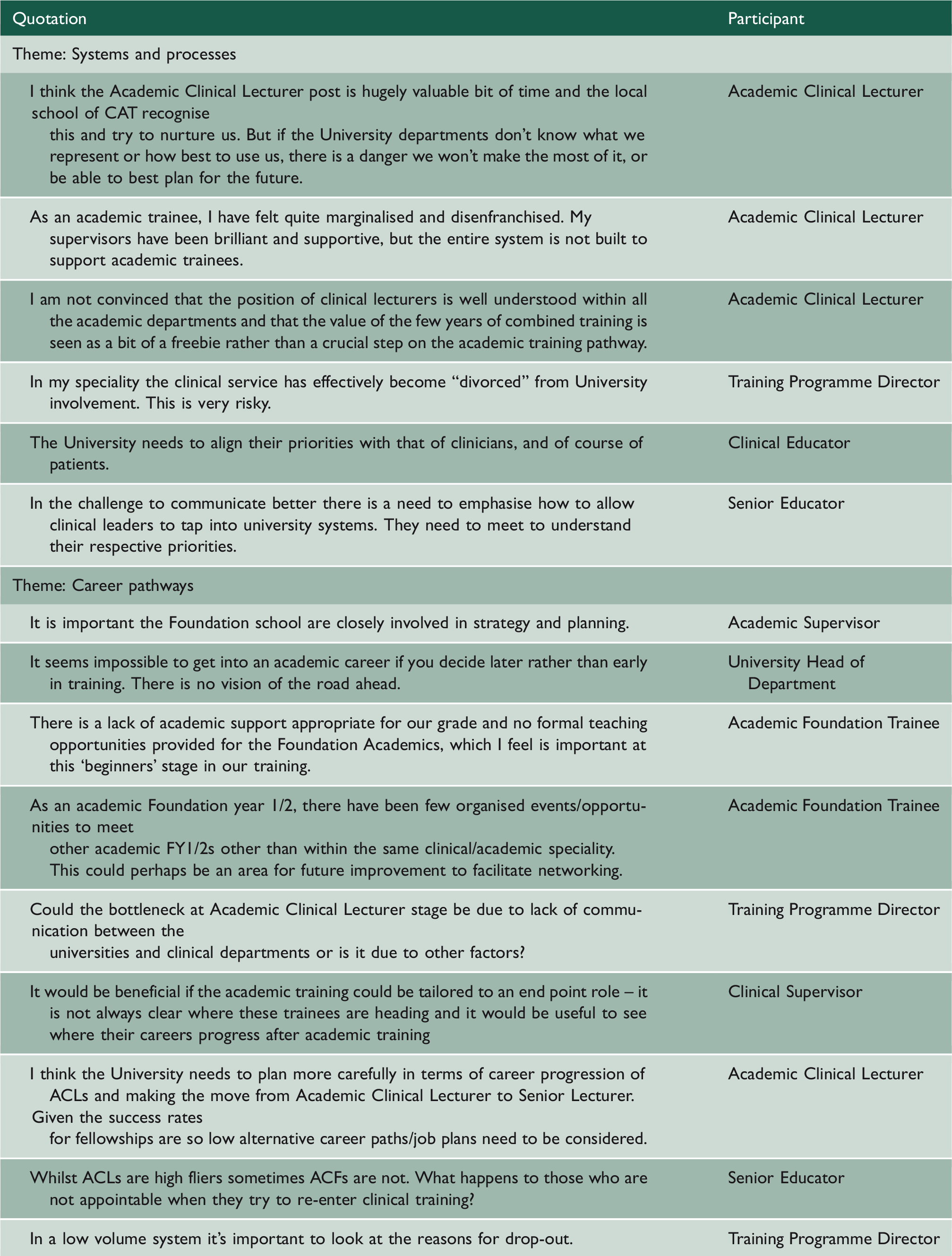
Examples of verbatim quotations for each theme.
Conclusions
Integrated Clinical Academic Training provides unique opportunities for individual trainees and clinical academic departments and is vital to identify, nurture and encourage the clinical academics of the future. Successful expansion of these programmes may attract high-calibre trainees and help to support important areas of clinical research, which in turn should both enhance clinical training programmes and improve patient care. With the opportunities come a number of challenges, both for the individual trainee (who is required to juggle commitments and develop clinical and academic skills in parallel), and for educators who deliver and administer the training pathways (who need to ensure that research opportunities align with clinical priorities, provide appropriate projects, support and mentorship and ensure that objectives and assessment processes are transparent and achievable). We have demonstrated that a programme of stakeholder engagement is a useful and feasible method of identifying areas for development in the governance of integrated academic training. Our findings will provide a practical framework on which to build our future programmes to maximise the benefits of clinical academic training for the benefit of the profession and patients alike.
Footnotes
Declarations
Acknowledgements
We would like to thank all those who participated in the surveys and focus groups, Professor Helen Budge (University of Nottingham), Lesley Clissold (University of Leicester) and Kate Bell (Health Education England working across the East Midlands) for their help with arranging the focus group sessions.
Provenance
Not commissioned; peer-reviewed by Faidon-Marios Laskaratos
Appendix 1 Clinical Academic Trainee survey questions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.