
Abstract
Objective
To understand the ethnic differences in coronary heart disease risk among inpatients with diabetes following acute coronary syndrome.
Design
Single-centre retrospective cohort-analysis of patients with type II diabetes over a six-year period receiving standard care.
Setting
Birmingham, UK.
Participants
One thousand and one hundred and five patients with type II diabetes from a multi-ethnic background.
Main outcome measures
Odds ratios of coronary heart disease events among three ethnic groups.
Results
The prevalence of coronary heart disease events was 20.7% in Asian, 13.2% in Caucasian and 7.7% in Afro-Caribbean patients. Asian patients were younger at diagnosis of diabetes (−5.1 years p < 0.001 versus Afro-Caribbeans and −7.1 years p < 0.001 versus Caucasians). The mean number of events was highest amongst Asian (1.2) compared to Caucasian (1.1) and Afro-Caribbean (1.0) patients (p = 0.04). The mean age at first event was 61.3 years for Asians, 62.5 years and 65.8 for Afro-Caribbeans and Caucasians, respectively (analysis of variance F[2,131] = 2.36 p = 0.09). Un-adjusted odds ratios for at least one coronary heart disease event were highest among Asian men (OR 5.04; 95% CI 2.31–11.01; p < 0.0001) with Afro-Caribbean women as baseline (OR 1.0). The odds ratios remain largely unchanged (1.0 Afro-Caribbeans [baseline], 1.27 [p = 0.56] Caucasians and 3.2 [p = 0.001] for Asians) when corrected for age, gender, duration of diabetes, insulin dependency, mean low-density lipoprotein-cholesterol, triglycerides and high-density lipoprotein-cholesterol, mean glycated haemoglobin, mean systolic and diastolic blood pressure (logistic regression; ROC: 79% AUC). Afro-Caribbean patients had the highest mean high-density lipoprotein-cholesterol (1.6 mmol/L) and the lowest risk for coronary heart disease events.
Conclusions
Asian patients were younger at their first event and diagnosed earlier with diabetes. Asian men had the highest risk of coronary heart disease event which correlated with the lowest levels of high-density lipoprotein-cholesterol.
Keywords
Introduction
Atherosclerotic cardiovascular disease is the leading cause of morbidity and mortality in patients with type II diabetes. 1 Hypertension and dyslipidaemia are risk factors for the development of atherosclerotic cardiovascular disease and often co-exist in patients with type II diabetes; additionally, diabetes is itself an independent risk factor for the development of atherosclerotic cardiovascular disease in both men and women. 2 The inherent protection that premenopausal women get from atherosclerotic cardiovascular disease is lost in the presence of diabetes.3,4 Analysis of the Framingham cohort revealed that the presence of diabetes doubled the age-adjusted risk for cardiovascular disease in men and tripled it in women. 2 Data from the prospective Nurses’ Health Study collected over 20 years found that the risk for developing diabetes in women, corrected for body mass index, was increased for Asians, Hispanics and African Americans (relative risk 2.26, 1.86 and 1.34, respectively) compared with whites. Similarly in the UK the risk of diabetes is four- to six-fold higher in south Asians compared to white indigenous population. 5 Whilst ethnic origin of an individual has an influence on the development of type II diabetes, equally it appears to modulate the risk of atherosclerotic cardiovascular disease in these individuals based on epidemiological studies.6–8 In the UK, it is estimated that mortality from coronary heart disease is 50% higher among south Asians compared to the indigenous white population largely due to higher prevalence of type II diabetes within this ethnic group. 9 The majority of these studies have been based on population screening of primary care databases and have focussed on cardiovascular mortality in multi-ethnic communities.10,11 Whilst the adverse effects of cigarette smoking on cardiovascular disease are well established, the complex interaction of ethnicity, hypertension, dyslipidaemia, renal dysfunction and diabetes remain poorly understood.
The city of Birmingham (UK) has a varied representation from all ethnic communities. The present study is a retrospective cohort analysis of coronary heart disease events (acute coronary syndrome, acute myocardial infarction) in patients with type II diabetes among the three main ethnic groups (Asian, Afro-Caribbean, Caucasian) presenting to the hospital cardiology unit over a six-year period. The fact that all patients had type II diabetes helped us eliminate the confounding effect that diabetes would have on coronary heart disease. The purpose was to understand the impact of cardiovascular risk factors on the development of acute coronary heart disease events in those admitted to hospital, which has a direct bearing on inpatient services.
Methods
This was a single-centre hospital-based retrospective cohort analysis of patients with type II diabetes defined as diabetes not requiring insulin within one year of diagnosis. The diagnosis of diabetes had been made adhering to national/international guidelines. The cohort extended over a six-year period (2004–2010) and included a random sample of patients attending the hospital diabetes clinic over that time. All patients were above 18 years old. All patients received standard care that would be in line with best clinical practice as would occur in a real-world setting. The analyses focussed on the coronary heart disease events occurring in individuals from the three main ethnic groups residing in the United Kingdom – Asians, white Caucasians and black Afro-Caribbeans – whilst they were receiving standard diabetes care. The data on ethnicity were ascertained through self-identification. Patients who died during this period were excluded from the final analyses as data for their cause of death were not available. Clinical and laboratory data were retrieved from the hospital clinical information systems for the period. All biochemical analyses had been undertaken in the same laboratory under similar conditions using the same assays. The number of attendances to hospital for diabetes care was not captured. The mean values for the subjects’ glycated haemoglobin, triglycerides, high-density lipoprotein-cholesterol, estimated glomerular filtration rate, body mass index and blood pressure (systolic and diastolic) were used in the analyses. The mean values for low-density lipoprotein-cholesterols were calculated using the Friedewald equation: low-density lipoprotein-cholesterol (mmol/l) = (total cholesterol − high-density lipoprotein-cholesterol) − (triglycerides/2.2). 12 The cohort therefore included patients with coronary heart disease and those without, the latter serving as a control group.
Statistical analyses
All statistical analyses were undertaken using STATA MP14 (StataCorp, Texas, USA). Frequency data are presented as n (%). Continuous variables are presented as mean (±standard deviation) or median with inter-quartile range. These include values for glycated haemoglobin, high-density lipoprotein-cholesterol, triglycerides, low-density lipoprotein-cholesterol, estimated glomerular filtration rate, body mass index, systolic and diastolic blood pressures. For baseline univariate analyses, analysis of variance was used to compare mean values between the three ethnic groups. The Bonferroni method was used for post hoc contrasts to quantify the magnitude of the difference between means after analysis of variance. Ordinary least-squares regression was used to model the effect of continuous dependent variables from sets of independent variables. Semi-partial correlation was used to quantify the influence of individual variables within the regression models. Logistic regression analyses were undertaken to calculate adjusted odds ratio for coronary heart disease events among different ethnic groups and identify variables that might have an influence on the overall model. The Wald chi-square statistic was used to quantify the difference. The nested regression method was used both for ordinary least-squares and logistic regressions to study the impact of a predetermined cluster of variables taken together. Ninety-five per cent confidence intervals were used as measure of estimate and consequently a p value of 0.05 was considered to indicate statistical significance.
Results
Patient characteristics.

Calculated using Friedewald equation (see manuscript). Data expressed as mean(standard deviation) unless specified.
Asian patients were younger at diagnosis of diabetes compared to the other two ethnic groups (−5.1 years p < 0.0001 versus Afro-Caribbeans and −7.1 years p < 0.0001 versus Caucasians). There was no significant difference between Caucasian and Afro-Caribbean patients (−2.0 years p = 0.181). Despite a strong positive correlation between time taken to start insulin therapy from diagnosis and the duration of diabetes (r = 0.64; p < 0.0001), there were no differences between the three ethnic groups after adjusting for age at diagnosis, body mass index and gender. Asian patients appeared to go onto insulin sooner, but this difference was not statistically significant. The calculated low-density lipoprotein-cholesterol was highest among Afro-Caribbean patients with statistically significant differences between the groups. Afro-Caribbean patients also had the highest mean high-density lipoprotein-cholesterol (1.58 mmol/l) compared to Asian (1.28 mmol/l) and Caucasian (1.36 mmol/l) patients (analysis of variance F[2,1063] = 56.86 p < 0.0001 for between group differences) with univariate analysis. This trend was maintained across the ethnic groups when adjusted for mean triglycerides, the presence or absence of coronary heart disease and gender, although the magnitude of the difference was altered, with highest levels among Afro-Caribbean patients (versus Caucasian −0.1 p = 0.016; versus Asians −0.2 p < 0.0001). Black women had a significantly higher high-density lipoprotein-cholesterol, than their male counterparts in this multivariate analysis (p < 0.0001). The body mass index was statistically lower in Asian patients compared to Caucasian patients and this contributed to statistical significance between the groups. The absolute difference in the mean values is given in the accompanying supplementary files (see Table: analysis of variance post-hoc contrasts [Bonferroni]).
The prevalence of coronary heart disease events within the different ethnic groups was 20.7% amongst Asian, 13.2% in Caucasian and 7.7% in Afro-Caribbean patients. Overall men had more coronary heart disease events compared to women except in case of Afro-Caribbean patients, where the sex ratio was reversed with a higher prevalence among women. The total number of events was highest amongst the Asians (88), less among the Caucasians (31) and least among the Afro-Caribbean (15) patients. The mean number of events amongst individuals with at least one event was highest amongst Asian (1.2) compared to Caucasian (1.1) and Afro-Caribbean (1.0) patients and this difference reached statistical significance (p = 0.04). The mean age at first event was 61.3 years for Asians, 62.5 years and 65.8 for Afro-Caribbeans and Caucasians, respectively. This difference was not found to be statistically significant (analyses, analysis of variance F[2,131] = 2.36 p = 0.09).
The prevalence of coronary heart disease events peaked between 60 and 70 years amongst the different ethnic groups: Asian 37.5%, Afro-Caribbean 60% and Caucasian 51.6%. For Asian patients, the vast majority of events happened by the sixth decade – Asian 45.5%, Afro-Caribbean 26.7% and Caucasian 22.6%. Further, by 50 years 15% of Asians had had their first coronary heart disease event compared to 6.5% of Caucasian and 6.7% of Afro-Caribbean patients (see supplementary files). The median time to first coronary heart disease event for the entire cohort was 12 years (inter-quartile range: 11 years). However, there was a negative linear correlation between the time to first coronary heart disease event and the age at diagnosis of diabetes (r = −0.48; p < 0.0001); those that had diabetes diagnosed early in life took longer to have their first coronary heart disease event. This relationship was maintained even after correcting for lipid levels, body mass index, blood pressure (systolic and diastolic), gender and ethnicity.
Unadjusted odds ratios of at least one event categorised by gender and ethnicity.

Chi 2 trend p < 0.00001.
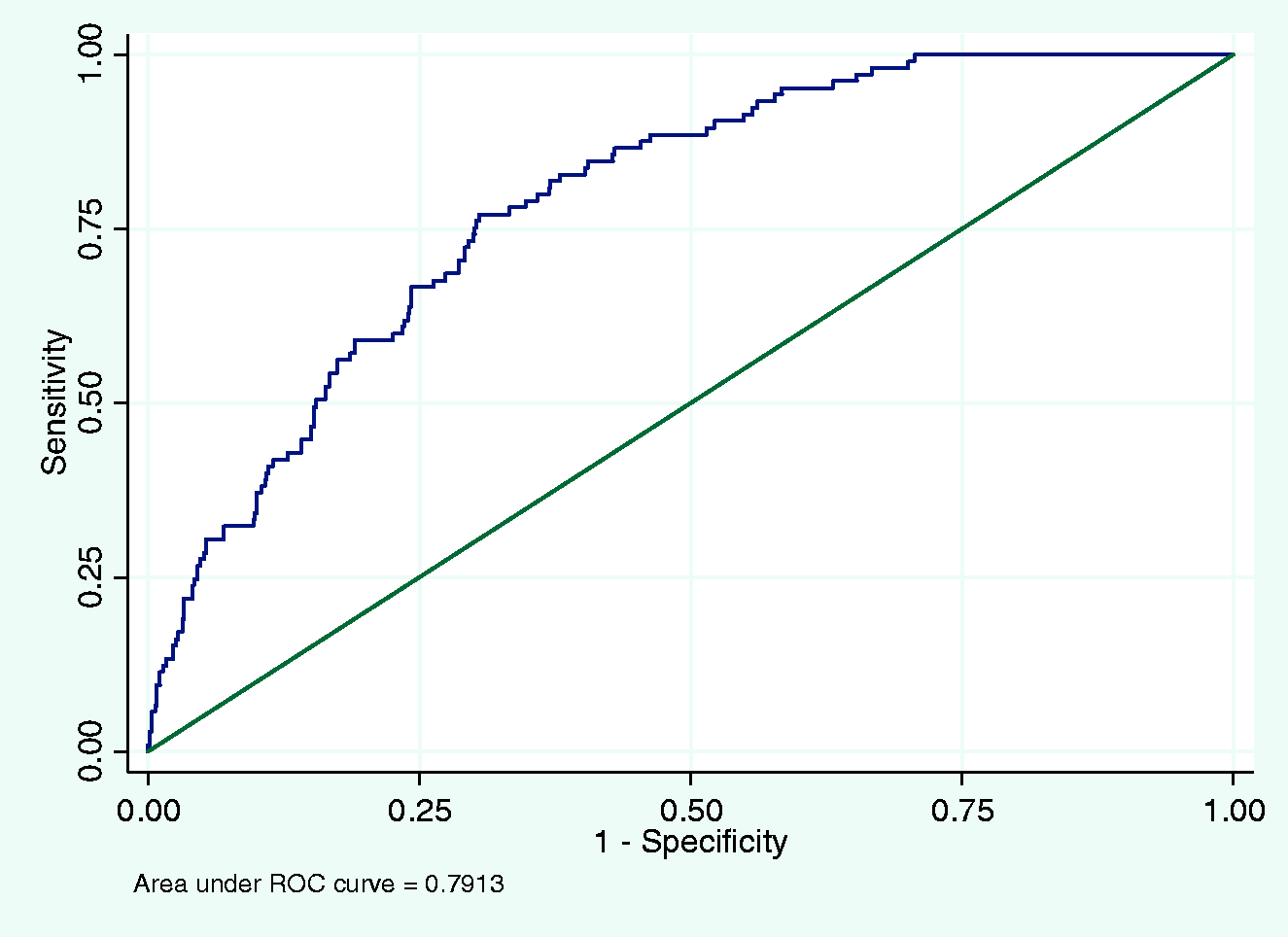
Receiver-operating characteristic curve for logistic regression model.
Discussion
Main findings
The present observational study based on data obtained from inpatient healthcare records reaffirms the high risk of coronary heart disease events witnessed among Asian patients in line with other epidemiological studies. Asian patients in this study appeared to be younger at diagnosis of diabetes as has been previously published. 13 Asians in our study had poorer metabolic control as evidenced by a higher glycated haemoglobin and lower mean high-density lipoprotein-cholesterol. They also had their first coronary heart disease event at a younger age; nearly half of the group (45.5%) suffered their first event by 60 years of age. An early age at diagnosis of diabetes is likely to expose individuals to longer period of deranged metabolic milieu that would aggravate pre-existing atherosclerosis. The majority of patients in this cohort independent of their ethnicity had diabetes diagnosed before their first coronary heart disease event, supporting this argument.
The prevalence of coronary heart disease was noted to be higher among Afro-Caribbean women compared to men, but this may reflect the small number of coronary heart disease events in our group as a whole. Afro-Caribbean women, on the contrary, had the lowest risk of having a coronary heart disease event with the highest risk among Asian men after correcting for available risk factors (ROC: 79% AUC); this correlated with the high high-density lipoprotein levels in this group (r = −0.9; p = 0.03) (Figure 2). The low risk was despite a high low-density lipoprotein-cholesterol suggesting that the high high-density lipoprotein-cholesterol appeared to be conferring a protective effect from coronary heart disease. This has been demonstrated previously.
14
Scattergram of high-density lipoprotein-cholesterol levels and odds ratio for CVD risk by ethnicity.
Comparison with existing literature
The presence of type II diabetes confers increased risk of cardiovascular events among all ethnic groups compared to the general population. This excess mortality has been shown to be disproportionately higher in Asians with diabetes – a three-fold increase in coronary heart disease-related deaths compared to a 1.5-fold increase in Asians without diabetes. 9 Although Afro-Caribbean patients have higher blood pressure, which may explain the higher mortality from stroke, this paradoxically has not shown to increase their risk of heart disease. 14 Coronary calcification appears to be an independent risk factor for coronary heart disease. Ethnic differences in coronary calcification have also been reported with higher calcium scores among whites compared to blacks. 15 In an excellent review, Barnett et al. 5 postulated that the underpinning mechanisms that might confer this differential risk to south Asians living in the UK may be altered insulin sensitivity, a high fat diet, and a sedentary lifestyle with limited exercise in the presence of abnormal lipid profiles – low high-density lipoprotein-cholesterol and high triglycerides. The United Kingdom Prospective Diabetes Study cohort was broadly representative of the UK demographic profile at the time and was able to follow up patients from the onset of type II diabetes to the development of micro- and macrovascular complications whilst receiving standard treatment for glycaemia and blood pressure.13,16,17 In the United Kingdom Prospective Diabetes Study, Afro-Caribbean patients were found to have a highly significant reduction (70%) in risk for coronary heart disease events predominantly fatal and non-fatal myocardial infarction relative to Caucasian patients even after adjusting for major cardiovascular risk factors. 16 The fact that there were no consistent between-group differences in blood pressure or glycaemia during the course of the United Kingdom Prospective Diabetes Study may lend further support to the view that other factors such as higher high-density lipoprotein-cholesterol and lower insulin resistance may be providing protection from coronary heart disease in Afro-Caribbean patients. Plasma lipid profiles were similar in Caucasian and Asian patients in the United Kingdom Prospective Diabetes Study but Afro-Caribbean patients had a much higher high-density lipoprotein-cholesterol and lower triglyceride levels than the other two groups and this paralleled their higher insulin sensitivity. 18 Our study similarly adds to this pool of existing literature validating the differential risk in atherosclerotic cardiovascular disease among different ethnic groups that is also reflected in hospital inpatients.
As the prevalence of type II diabetes increases globally International Diabetes Federation Diabetes Atlas Eighth Edition 2017 at http://www.diabetesatlas.org/, the combined effects of diabetes and atherosclerotic cardiovascular disease will inevitably place a significant demand on healthcare resources in the future and perhaps more so among high-risk ethnic groups. Whilst aggressive management of atherosclerotic cardiovascular disease risk factors with multi-factorial intervention in both type I and type II diabetes has shown to be effective,19–22 preventive strategies developed around healthy diet and lifestyle which have been of proven value both in delaying the onset of diabetes23,24 and protecting from cardiovascular disease 25 must be the best way forward in addressing the impending pandemic.
Limitations of our work
There are certain limitations to our work. It was retrospective and observational and therefore may not have been fully adjusted for confounders. However, the AUC of 79% did indicate a good overall fit of the model. Overall, the data represent real-world experience within the NHS and can easily be extrapolated elsewhere; the findings are in keeping with published evidence. The data extend between 2004 and 2010. We strongly feel that the results would be reproducible if this study were to be repeated under similar conditions largely because the demographics of the population at risk have not altered in any way.
Summary
This retrospective analysis among inpatient groups from the three ethnic groups is the first of its kind in the medical literature that we are aware. It demonstrates that Asian patients with diabetes are younger and at a higher risk of acute coronary heart disease events. They may also present with poorer metabolic control and, as is known, with an unfavourable lipid profile. This rekindles the prospect for health-economic modelling to ascertain the impact that the burgeoning incidence of type II diabetes would have on hospital cardiovascular services in the future. Although much has been postulated around the differential cardiovascular risk among ethnic communities and that high-density lipoprotein-cholesterol may be the missing link, further research is required to confirm or refute this argument. If ethnicity is to have a significant modulating influence on atherosclerotic cardiovascular disease outcomes, then one can envisage future healthcare risk-stratification strategies being suitably modelled around multi-ethnic populations groups. Every CVD event has a direct impact on an individual’s health and future well-being. It also impacts on hospital services as all patients with suspected or proven acute coronary syndrome Lindemann R, Romero L, Hundley R, Allen A, Liang H, Baumgartner R, et. al. attend hospital for emergency care. It follows that inner-city hospitals that serve a high population of ethnic minority communities will have a higher demand placed on their healthcare resources.
Footnotes
Authors’ note
Availability of data and material: The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declarations
Acknowledgements
We would like to acknowledge the Cardiology department at City Hospital to allow access to data on acute coronary events on the diabetic patients included in this study.
Provenance
Not commissioned; peer-reviewed by Padmanabhan Badrinath.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.