
Abstract
This article highlights a rare complication of syphilis infection and the importance of including syphilis and antiphospholipid antibody testing in the acute stroke screen..
Case
A 38-year-old man presented following a tonic clonic seizure at work. Neurological examination revealed a Glasgow Coma Score of 13/15 and reduced vision bilaterally. He had no medical history, no regular medications and no history of drug or alcohol abuse. CT head showed early changes of bilateral temporo-occipital infarction. CT angiography showed evidence of tapering and occlusion in both posterior cerebral arteries but not the basilar. There was no evidence of vertebral stenosis or dissection. As infarction was already established, he was not thrombolysed but commenced on aspirin (Figure 1). Subsequent CT and MRI showed additional infarction of the right thalamus. ECG and chest X-ray were unremarkable. Admission laboratory tests demonstrated a raised C-reactive protein of 42 mg/L and erythrocyte sedimentation rate of 44 mm/h. Cardiac investigations were normal including transthoracic and bubble contrast echocardiogram and 24 h ECG.
MRI head showing bilateral temporo-occipital infarcts.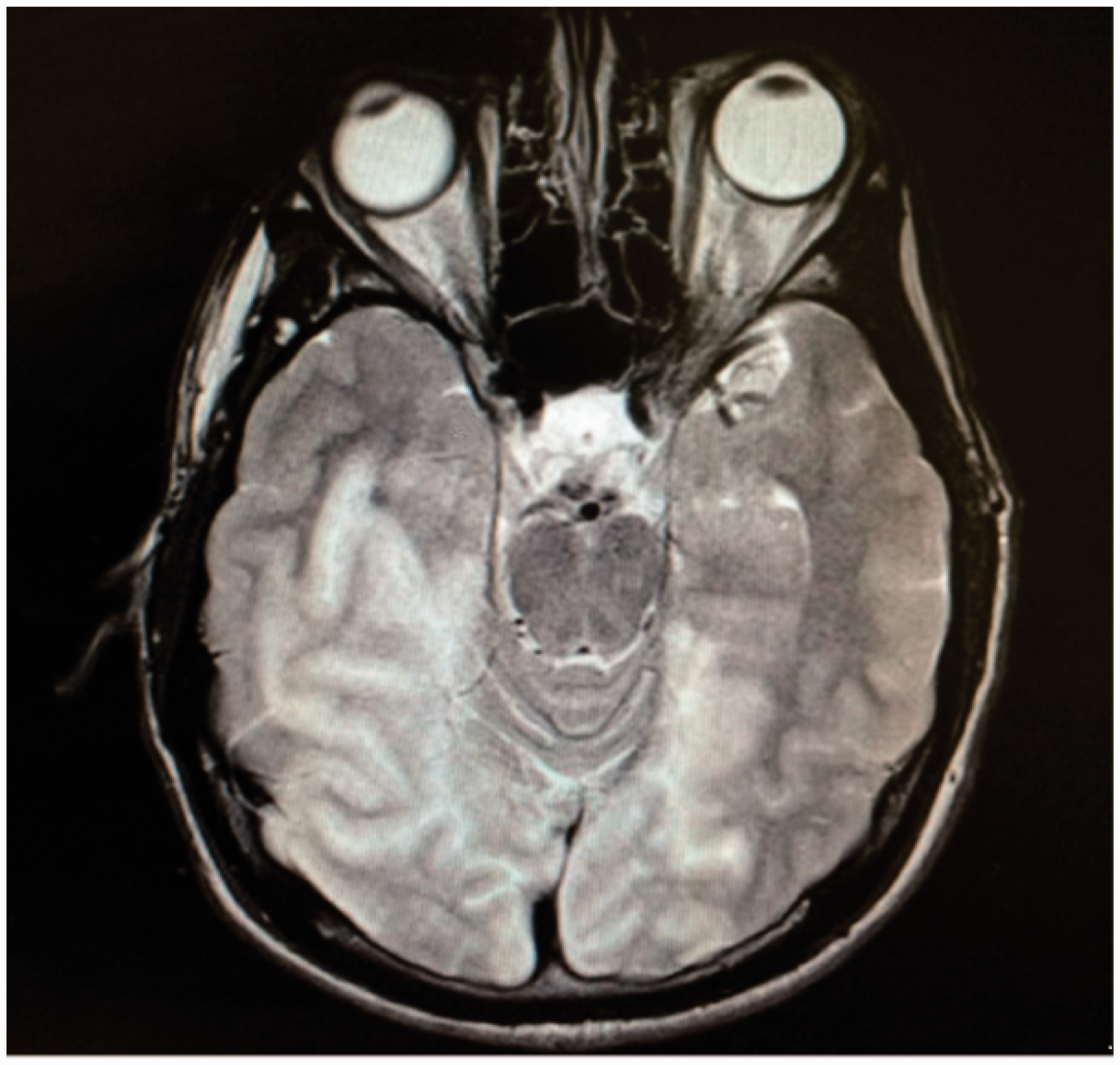
He was subsequently transferred to his local stroke unit for ongoing rehabilitation, where in addition to his cortical blindness, he was found to have profound short-term memory loss. He was also noted to be sexually disinhibited. His family reported this was a marked exaggeration of his usual personality. It was not clear whether the behaviour was the result of the stroke or related to the cause of the stroke. Tests for homocysteine, anti-neutrophil cytoplasmic antibody, autoantibodies, Lyme’s disease and HIV were normal or negative. Syphilis serology showed a positive rapid plasma reagin test of 1:16, with a positive treponemal IgM. His treponema pallidum particle agglutination assay was positive at 1:1280.
Further examination revealed that he had large anisocoric pupils that were non-reactive to light and poorly reactive to accommodation. MRI and MR angiography showed no specific features of a syphilitic vasculopathy. Lumbar puncture revealed a raised cerebrospinal fluid white cell count of 27 (90% lymphocytes), a raised protein at 912 mg/L. Cerebrospinal fluid treponema pallidum particle agglutination assay was positive 1:320, cerebrospinal fluid rapid plasma reagin was negative.
It was felt that there was enough clinical and serological evidence to make a presumed diagnosis of neurosyphilis, and he underwent treatment with 1.8 million units of procaine penicillin intramuscular once daily and 500 mg probenecid four times daily for 17 days. He was given a four-day course of prednisolone 40 mg to prevent a Jarisch-Herxheimer reaction. His sexually inappropriate and labile behaviour improved almost immediately. His repeat syphilis serology three weeks later showed an rapid plasma reagin of 1:8, and a year later, it was negative. Subsequent history emerged that the patient who was from Eastern Europe had been promiscuous in his youth and 10 years previously had consulted for urethral discharge and three years ago had an unknown papular lesion of his inner thigh which eventually disappeared. It transpired that his change in behaviour also pre-dated the stroke.
His thrombophilia screen was also abnormal. He had a mildly positive anticardiolipin antibody at 23 U/ml (<10 U/ml) and a lupus anticoagulant with a positive dilute Russell Viper Venom ratio of 1.61 and 1.74 (<1.2 ratio) on two separate occasions which corrected more than 12%. He was commenced on anticoagulation to treat a possible co-existing or syphilis-induced antiphospholipid syndrome.
Discussion
This case highlights a number of interesting points. Firstly, sexual disinhibition after stroke can be from the stroke itself or related to the cause of the stroke. There are reports of frontal lobe, temporal lobe and thalamic strokes being associated with sexual disinhibition. 1 In this case, the fact it resolved so quickly after treatment for syphilis does suggest it may have been related to neurosyphilis rather than the stroke itself.
The diagnosis of neurosyphilis was considered presumptive; for although the cerebrospinal fluid rapid plasma reagin was negative and a cerebrospinal fluid treponema pallidum particle agglutination assay titre less than the more suggestive level of 1:640, there was strong supportive evidence with cerebrospinal fluid pleocytosis and high protein, the pupillary changes and the behavioural change which improved on treatment.
Neurosyphilis can occur at any stage of the infection so which type did he have? Possibly meningovascular with the stroke, cerebrospinal fluid changes and the latency of 2–12 years. There was no imaging evidence of vasculitis, but sometimes this cannot be shown. Behavioural and pupillary abnormalities may be expected in parenchymatous syphilis but against it would be the timing and response to treatment. 2
A diagnostic conundrum can occur as in this case when both tests for syphilis and antiphospholipid syndrome are positive. The positive anticardiolipin antibody test could be expected in syphilis due to the cross-reactivity of the reagin antibodies found in syphilis with cardiolipin. Similarly, rapid plasma reagin can be positive in the presence of anticardiolipin antibodies in antiphospholipid syndrome. However, it is much rarer to have positive treponemal tests in antiphospholipid syndrome, 3 and not reported that an lupus anticoagulant is found in syphilis. 4 It was felt that positive lupus anticoagulant on two occasions was confirmatory of an active antiphospholipid syndrome. It was concluded he had dual, possibly interlinked pathology, a syphilis-induced antiphospholipid syndrome which may have had an aetiological role in the stroke through thrombosis rather than a direct vasculitic mechanism. A finding described in other infections but not previously described in syphilis. 5
Syphilis has been on the rise in England since the late 1990s particularly in London where in 2015 the number of cases accounted for 56% of all cases in England. 6 Most cases are seen in individuals co-infected with HIV and an increase in diagnosis is seen largely due to more risky sexual behaviours and increased awareness and testing. 7
As a learning point, syphilis should be part of the screen for acute stroke and antiphospholipid syndrome tests should always be done in conjunction. 8
Footnotes
Declarations
Acknowledgement
None
Provenance
Not commissioned; peer-reviewed by Herbert Budka.