
Abstract
Objective
We investigate whether physicians in secondary care in the English NHS receive adequate training to recognise and appropriately refer for services those persons suspected to be victims of human trafficking.
Design
Freedom of Information requests were sent to the 105 England’s NHS Trusts delivering acute care in England.
Setting
NHS Trusts providing secondary care in England.
Participants
English NHS Trusts.
Main outcome measures
We requested data about the training provided on human trafficking to clinicians, including the nature, delivery, and format of any education, and any planned training.
Results
A total of 89.5% of the 105 Trusts responded. Of these Trusts, 69% provide education to physicians on human trafficking, and a further 6% provide training but did not specify who received it. The majority of Trusts providing training did so within wider safeguarding provision (91%). Only one trust reported that it provides stand-alone training on trafficking to all its staff, including physicians. Within training offered by Trusts, 54% observed best practice providing training on the clinical indicators of trafficking, while 16% referenced the National Referral Mechanism. Amongst those not providing training, 39% of Trusts report provision is in development.
Conclusions
Our results find that 25% of NHS Foundation Trusts appear to lack training for physicians around human trafficking. It is also of concern that of the Trusts who currently do not provide training, only 39% are developing training or planning to do so. There is an urgent need to review and update the scope of available training and bring it into alignment with current legislation.
Background
Human trafficking – now known in the United Kingdom (UK) often by the broader term ‘modern slavery’ – is a growing and abhorrent crime, involving the exploitation of both adults and children. 1 At present, individuals are exploited in the sex trade (including in prostitution, escort work, and pornography), in forced labour (across the manufacturing, farming, construction, entertainment, and tourism industries), through organ harvesting, and in domestic servitude, amongst other trades.1,2
Human trafficking is an escalating problem in the UK and the rest of Europe. There is scant data on its actual scale, but in England between 10,000 and 13,000 individuals are believed to be trafficked each year. 3 The vast majority of trafficked persons remain unassisted, a failure that has deleterious consequences for mental and physical health. Alongside the on-going refugee crises and recent Brexit vote which looks to restrict legal migration routes, there is a danger that trafficking within and to the UK will increase.4,5
The broad spectrum of abuse categories that fall under the ‘trafficking’ term leads to a wide variety of physical and psychological sequelae. The heterogeneity of clinical presentation amongst victims of human trafficking presents a great challenge to healthcare workers seeking to identify and treat them. Health problems can reflect the type or types of abuse suffered: for example victims of sexual exploitation suffer higher rates of sexually transmitted infections such as HIV and Hepatitis B. 6 However, general health trends amongst this population have been observed: they include an increased risk of suffering traumatic injuries such as fractures, bruising, and bleeding; increased risk of chronic pain; exacerbation of pre-existing chronic disease; dental and nutritional problems; and mental health disorders such as depression, personality disorders, and anxiety disorders such as Post-Traumatic Stress Disorder (PTSD), as well as an increased risk of suicide and self-harm.7–13
Additionally, due to the nature of human trafficking as a crime that relies on the isolation and disempowerment of its victims, several barriers exist to their engaging with healthcare professionals, for example language difficulties, controlling behaviour by traffickers, and a lack of awareness of entitlement on the part of the victim. 14 The nature of the clinical presentation of such individuals, coupled with these unique barriers to engagement, constitutes a significant challenge to healthcare professionals who come into contact with them. And yet, research and policy widely acknowledge that healthcare professionals are advantageously positioned to identify and assist trafficked individuals, sometimes uniquely and exclusively so.15–17 In its 2015–2017 ‘Strategic Plan’, the UK Independent Anti-Slavery Commissioner has confirmed that healthcare professionals, including doctors, play a vital role in victim identification. 15
For this to happen physicians must first be aware of risk factors, clinical indicators, and appropriate response strategies. Clinical indicators include, for example, traumatic injuries consistent with manual labour or physical and/or sexual abuse, the presence of a ‘minder’, inability to speak the local language, evidence of international migration, and work in a job sector associated with trafficking. 18 Victims of trafficking can present to both primary and secondary care. 14
Until recently, scant research had been done in the UK on the context and scale of contact between healthcare professionals and trafficked individuals. Recent studies have observed that such contact occurs in both primary and secondary care settings.7,14 Despite this, however, the UK response to trafficking, until recently, neglected to involve consistent training and engagement with the health sector. 19 In the setting of secondary care it has been shown that victims of trafficking can present to a wide variety of specialties and services, including emergency medicine, sexual health, maternity services, paediatrics, gynaecology, as well as other general medical specialties.14,16 However, it is speculated that current physician training is inadequate. One recent cross-sectional survey of 782 NHS professionals in secondary care settings found that 86.8% of participants reported lacking knowledge of how to identify potential victims of human trafficking, and 78.3% reported they lacked the knowledge and confidence to assist trafficked people. 7 This gap likely arises from inadequacies in training available. Indeed, the same study concluded that better training provision for healthcare workers would improve their ability and preparedness to identify and appropriately treat and refer victims of human trafficking who might otherwise remain untreated. 7
We acknowledge that more research is needed in both primary and secondary care; the focus of this short study is on the latter; we ask whether England’s physicians in the setting of secondary care receive sufficient training to recognise and appropriately refer for services those persons suspected to be victims of human trafficking.
Methods
Information on training provision specific to human trafficking within NHS Trusts is not publicly available. We sent Freedom of Information requests to 105 NHS Foundation Trusts and Trusts providing acute hospital care in England in 2016 (see Appendix 1). These Trusts were identified via the NHS website, with information from the Quality Assurance Agency (QAA) and UK Government’s website,20–22 and represented all relevant Trusts providing acute secondary care. The scope of the study necessitated a focussed approach on secondary care, but the authors acknowledge the need for research in primary care also. According to the legislation, the Trusts have 20 business days to respond.
The request contained an initial closed question directed to identify provision of training on trafficking. Based on the answer of either ‘yes’ or ‘no’ to this initial question, further closed questions were then asked about the extent, content, and any planned future provision. For example, Trusts who answered ‘yes’ were asked whether they provided training to clinical staff, and in particular doctors at various levels of seniority. Trusts were not required to provide a breakdown of other clinical staff receiving training. Where responses did not follow the Freedom of Information structure or were ambiguous, to reduce bias, we sought clarification from the relevant information governance officer, or where possible entered data in line with the original Freedom of Information question structure.
Results
Out of 105 Trusts, 94 Trusts (89.5%) provided a response to the Freedom of Information, while 11 (10.5%) did not reply to the request or any follow-up in contravention of the Freedom of Information Act 2001. Of the 94 Trusts providing answers to the request, two declined to respond citing exemptions in the legislation, giving a response for analysis rate of 87.6%.
Provision of training
Figure 1 shows the results of the survey. Sixty-five Trusts (69%) responded that they provide training for physicians on human trafficking. Additionally, four Trusts (4%) stated that they provide training to clinical staff but did not specify which staff groups. In total, 69 Trusts (75%) responded that they provide training for some or all staff. Twenty-three Trusts (25%) do not provide any training, either indicating that they are only mentioning in passing the issue (8%, n = 7) or not providing any mention of the issue (17%, n = 16). Of those not offering training, 39% (n = 9) responded that training is in development. Two Trusts (2%) identified that they were considering requiring staff to complete the Human Trafficking Programme via Electronic Staff Record – a digital platform offering e-Learning for staff in the NHS. Next, we evaluated the content of training among those 69 Trusts that provide it.
NHS Trust provision.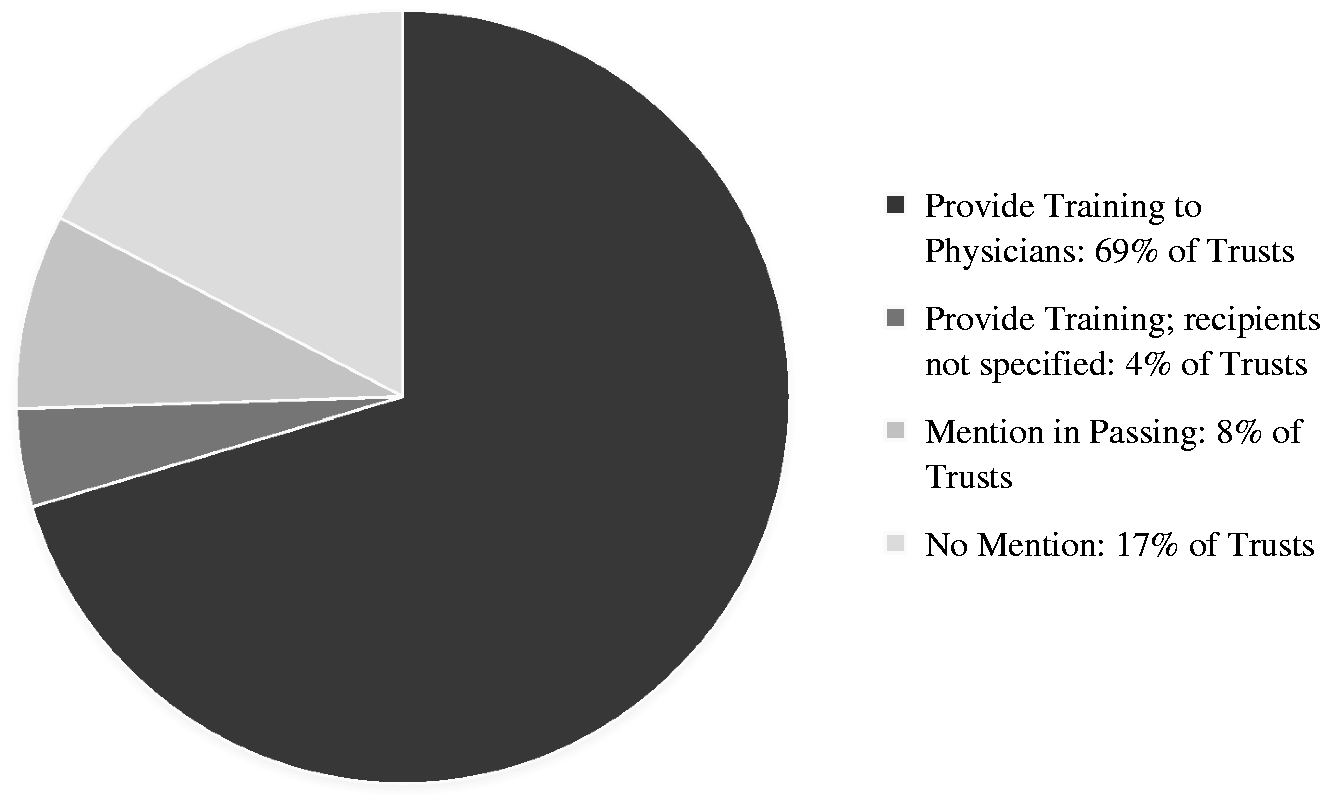
Training content
Of the 69 Trusts identified as providing training, 21 (30%) provided training to all their staff and 39 (57%) to all clinical staff, both of which criteria include physicians. Only two (3%) Trusts separated training by medical grade, and four (6%) provided training to only specific staff groups in certain specialties, namely those working in Emergency Medicine or those working with children. Of the Trusts that provide training to all clinical staff, two (3%) provide more focussed specialty specific training in addition to general provision. Four Trusts (6%) declined to specify.
The 69 Trusts identifying provision were asked to provide details on the training content and delivery. One Trust (1.5%) reported that they provide stand-alone training on the subject of human trafficking to all staff, while 63 Trusts (91.5%) provided training as part of safeguarding training – either safeguarding adults or children, or both. Notably, two Trusts also reported that alongside this general safeguarding training, stand-alone training is provided to specific key staff groups (e.g. A&E consultants and nurses). Five Trusts (7%) did not specify whether their training was standalone or not. Trusts were not asked if training was mandatory.
Of the training on human trafficking that was included in safeguarding by 63 Trusts, they differed as where in the general safeguarding provision such training was provided. For example, 30% (n = 19) of Trusts included trafficking training in the content on safeguarding adults, 8% (n = 5) included it only in safeguarding children, 30% (n = 19) included it within both safeguarding adults and children training, and 32% (n = 20) of Trusts did not respond on this question.
Trusts were asked whether the training they provided included reference to the clinical indicators of human trafficking, a key point in recognised best practice in training.17,23 Of the 69 Trusts providing training, 37 (54%) reported that their training contained content on clinical indicators, 26 (38%) reported that their training did not contain the relevant content, three (4%) stated they provide training to specific staff groups on clinical indicators, and three Trusts (4%) declined to answer the question (see Figure 2).
Training on clinical indicators. Training on the National Referral Mechanism.

Trusts were asked whether the training they provided included reference to the National Referral Mechanism, the official pathway for the identification and support of victims of human trafficking or modern slavery in the UK. Of the 69 Trusts providing training, 11 (16%) replied that the National Referral Mechanism is covered, 50 (72%) did not refer to the National Referral Mechanism, two (3%) said they provide training to specific staff groups, which referenced the National Referral Mechanism, and six (9%) declined to answer the question (see Figure 3).
Mechanism for training delivery
Trusts were also asked how they delivered their teaching on human trafficking, in light of recent findings that online only modules may have decreased efficacy, and that they may be being reproduced without adequate updating and evaluation.24,25 Of the 69 Trusts providing training, 28 Trusts offered combined methods of teaching, while 27 Trusts (39%) delivered face-to-face teaching, and three Trusts (4%) provided e-Learning delivery only. Three Trusts (4%) only used workbooks. One Trust (1%) used face-to-face teaching combined with workbooks. Eight Trusts (12%) declined to specify.
Of the non-providing Trusts, four (6%) said that they were considering requiring staff to complete the Human Trafficking Programme via e-Learning for Healthcare, an admirable national training platform delivered electronically via the Electronic Staff Record.
For full table of results, see Appendix 1.
Discussion
Our evidence reveals that training on human trafficking in hospitals in the NHS England is inconsistent, with gaps in training provision that are deeply concerning. Over one-fifth of Trusts appear to provide no training, either apart from or within safeguarding training. Of the Trusts providing training, about 40% do not adhere to best practices. These results help account for why healthcare workers lack the confidence and knowledge to address trafficking; a significant number of clinicians lack training. 7
The clinical implications of such a lack of training could constitute the failure of a duty of care on the part of the NHS to appropriately identify and treat victims of human trafficking, whose health needs are significant, and whose identification is challenging.7,14,16 One US study estimates that 28% of trafficking survivors came into contact with healthcare professionals at some point during captivity. 26 According to the UK’s newly appointed Independent Anti-Slavery Commissioner (IASC), such contact represents a crucial opportunity for intervention and constitutes a vital part of governmental strategy to combat modern slavery as a whole. 15 This is not to mention the profound beneficial impact that it could have upon victims of this crime.
As with all request approaches, our analysis has several limitations. Eleven Trusts did not reply to the request or subsequent emails, in contravention to the legislation, leaving us with an incomplete data set. We followed up these Trusts to improve compliance with future information requests. Also, some Trusts failed to answer the questions in alignment with the request, instead providing extended prose. We moved the data into alignment with the questions, which may have introduced bias through our classification. Additionally, because requests are sent to information governance officers who acquire data from other staff to answer to the request, there is also a chance these officers may have introduced bias when interpreting responses from safeguarding leads or training leads.
Our observations clearly, though, have implications for both policy development and NHS training provision. For policy, there is an urgent need to develop training in those 22 Trusts that appear to lack it. At present, the lack of training stands in contrast to legal requirements set out in the Care Act 2014 and Modern Slavery Act 2015 for safeguarding adults and children from abuse and neglect, including human trafficking. 27 The Independent Anti-Slavery Commissioner could liaise with these Trusts to help speed up the process and aid those Trusts with training in development.
For training, several Trusts’ training programmes did not adhere to best practices, which could be rectified in several ways. One area of development pertains to the indication that Trusts use or intend to use the e-Learning for Healthcare platform as a sole mechanism for delivery of training, which is concerning as this module is out of date following the inception of the Modern Slavery Act 2015, and fails to encourage completion of the MS1 form – a new anonymous data collection form directed to improve information on trafficking in the UK. 3 Additionally, several Trusts revealed in their responses to us that they do not have access for all staff to this platform due to human resource processes, so its use must be extended as well as revised.
A second area for training development is in providing specialised guidance and training on clinical indicators.7,17 This is important because persons subjected to trafficking can display a wide variety of health problems, as detailed above, or may have ‘no obvious risk factors or indicators of abuse’. 16 Clinicians should also proactively obtain information on vulnerable migrants, including trafficked persons, especially in the wake of recent national and regional developments.
Additionally, training needs to cover both adult and child trafficking. We found that 43% of training was exclusively geared towards one group only. This is troubling as when referring using the National Referral Mechanism, consent is required if the patient is an adult, but not if they are a child. 28 Limiting training to one framework may result in clinicians lacking awareness of the diversity of individuals covered by current charging exemptions and referral mechanisms. Vulnerable adult and child migrants may be missed, or may be inappropriately charged for their healthcare; a potential outcome that may compound the stress and harm they are already experiencing.
Results of FOI request.

ED: Emergency Department; ESR: Electronic Staff Record; HCA: Healthcare Assistant; OLM: OLM Systems – A group providing e-learning for healthcare; NRM: National Referral Mechanism; RCPCH: Royal College of Paediatrics and Child Health; SG: Safeguarding; FOI: Freedom of Information request.
Footnotes
Declarations
Acknowledgements
None
Provenance
Not commissioned; peer-reviewed by Rachel Bingham