
Abstract
Mycobacterium avium intracellulare infection or colonization should be considered in the differential diagnosis of hypercalcemia, especially in immunocompromised individuals, in the appropriate clinical context.
Keywords
Introduction
Hypercalcaemia has been widely described in granulomatous pulmonary diseases. Mycobacterium avium-intracellulare-induced hypercalcaemia is a recognised cause based on case reports, although is considerably rare compared to other aetiologies. Hypercalcaemia related to Mycobacterium avium-intracellulare infection has been reported in immunocompromised hosts, particularly those with AIDS. We describe a case of hypercalcaemia secondary to Mycobacterium avium-intracellulare infection in a patient without AIDS or malignancy.
Case report
Serum laboratory studies at baseline, presentation, hospitalisation and follow-up.
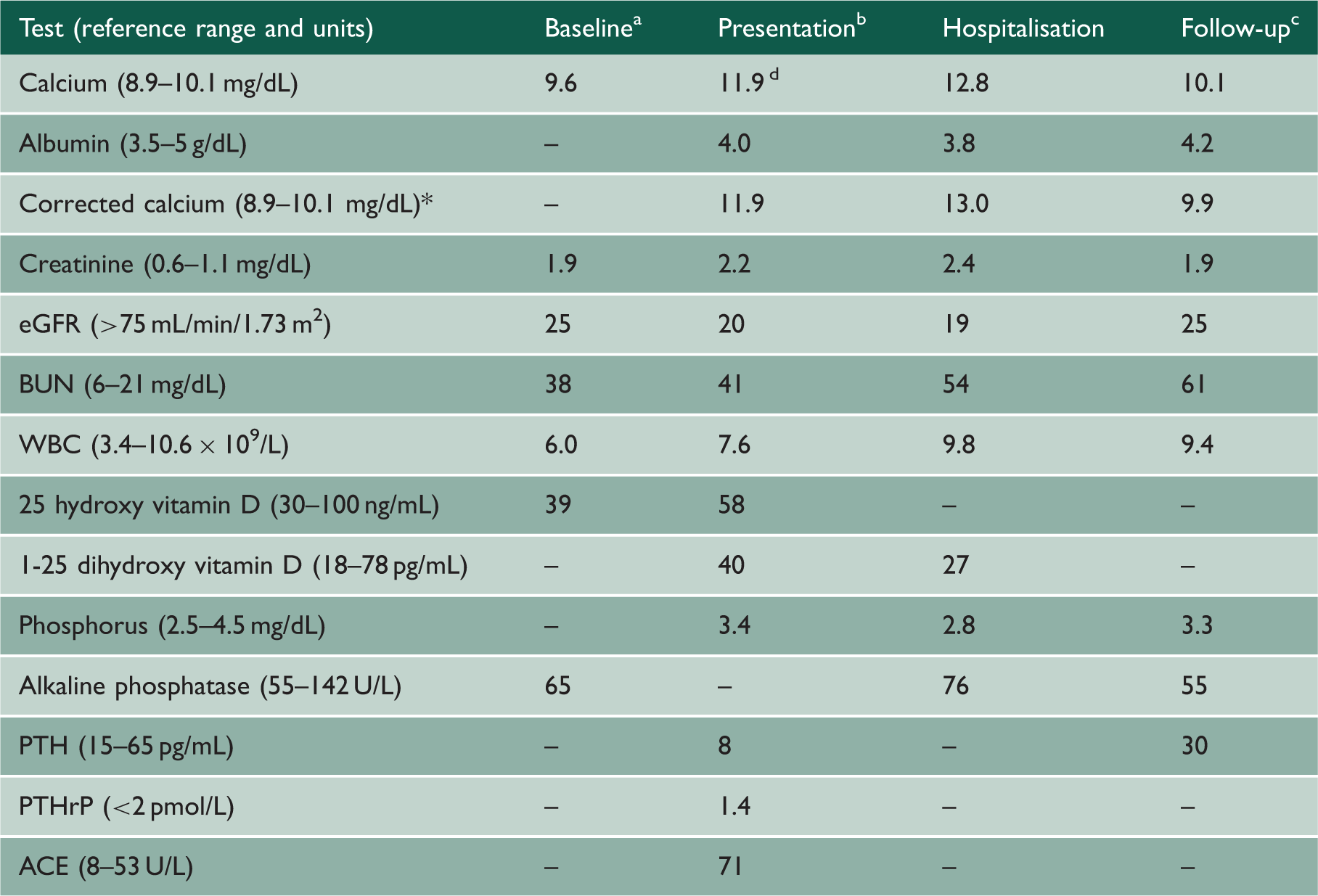
ACE: angiotensin converting enzyme; eGFR: estimated glomerular filtration rate; PTH: parathyroid hormone; PTHrP: parathyroid hormone-related peptide.
Seven months prior to hospitalisation.
One month prior to hospitalisation.
Six months after hospitalisation.
Highest recorded serum calcium prior to hospitalisation. *The corrected calcium was derived by accounting for a 0.8 mg/dL decrease in total serum calcium for each 1 g/dL reduction in serum albumin concentration (where a normal serum albumin is 4 g/dL).
Her home medications were carvedilol, vitamin B12, duloxetine, fentanyl patch, hydrocodone/acetaminophen, furosemide, potassium chloride and a multivitamin. She had scattered crackles on pulmonary examination and normal oxygen saturation on room air. Serum calcium level at admission was 12.8 mg/dL. Other notable initial laboratory findings included creatinine 2.4 mg/dL and BUN 54 mg/dL. Serum white blood cell count and alkaline phosphatase were normal. Initial chest X-ray (Figure 1(a)) showed diffuse patchy opacities. Computed tomography chest (Figure 1(b)) showed extensive tree-in-bud-type micronodularity predominantly in the upper lobes, as well as a 1-cm nodule in the right upper lobe, and underlying bronchiectasis and bronchiolectasis. Computed tomography abdomen/pelvis was grossly unremarkable and not indicative of any malignancy. Serum and urine electrophoresis and skeletal survey were unremarkable. Twenty-four hour urine calcium level was within normal limits. Bronchoscopy was performed and bronchoalveolar lavage (BAL) cultures grew Mycobacterium avium complex, with biopsies showing some non-necrotising granulomas. Other bronchoalveolar lavage studies, including Coccidioidomycosis polymerase chain reaction, Mycobacterium tuberculosis Polymerase chain reaction and Nocardia smear, were negative. The patient was treated with prednisone and her calcium normalised. She was discharged on gradual prednisone taper and required continued low dose prednisone outpatient to suppress her hypercalcaemia. She was not treated for atypical mycobacterial disease given her lack of pulmonary symptoms in the setting of multiple comorbidities.
(a) Chest radiograph posterior-anterior and lateral showing patchy, multifocal pleural parenchymal scarring and upper lobe nodularity, greatest at the right upper lobe apical and posterior segments, with coarse appearance to the interstitium. (b) Computed tomography scan of the chest with two axial slices of the upper lobes showing extensive “tree-in-bud-type” micronodularity with bronchiectasis and bronchiolectasis. Findings involved all lobes of both lungs, but were particularly prominent in the upper lobes.
Discussion
The current vignette describes a patient with hypercalcaemia presumed secondary to Mycobacterium avium-intracellulare infection or colonisation. This is the second case described to our knowledge of Mycobacterium avium-intracellulare-induced hypercalcaemia in a patient without human immunodeficiency virus or lymphoma. Significant testing was undertaken to rule out malignant and other causes. Angiotensin converting enzyme level was mildly elevated, but this was thought secondary to pneumonitis rather than sarcoid given the imaging findings and clinical picture. Mycobacterium avium-intracellulare infection was demonstrated through bronchoscopy cultures. The other reported case describes hypercalcaemia mediated by elevated 1,25 dihydroxyvitamin D secondary to Mycobacterium avium-intracellulare hypersensitivity pneumonitis. 1 The present case is associated with normal activated vitamin D levels.
Hypercalcaemia has an established correlation with granulomatous diseases such as sarcoidosis and tuberculosis and has only relatively recently been recognised in association with Mycobacterium avium-intracellulare. Both in conjunction and independent of Mycobacterium avium-intracellulare, hypercalcaemia has been described in a number of patients with AIDS and lymphomas.2–6 The most likely mechanisms for hypercalcaemia in these populations are related to increased 1,25 dihydroxyvitamin D production from granulomas and parathyroid hormone-related peptide or lymphokines secreted by lymphomas. 7 Enhanced conversion of 25 hydroxyvitamin D to its active form, 1,25 dihydroxyvitamin D, via extra-renal 1 -α hydroxylase activity is thought to underlie the pathophysiology of hypercalcaemia associated with granulomatous disease.
The present case is also interesting in that the 1,25 dihydroxyvitamin D level was normal. Renal 1-α hydroxylase is regulated by parathyroid hormone, calcium, phosphorus and 1,25 dihydroxyvitamin D, whereas 1 -α hydroxylase in activated macrophages is not responsive to such feedback mechanisms. There is a case report of sarcoid-related hypercalcaemia and a case of Mycobacterium avium-intracellulare-related hypercalcaemia in a patient with human immunodeficiency virus, both describing normal vitamin D metabolites, suggesting that relative excess 1,25 dihydroxyvitamin D levels can be sufficient to cause hypercalcaemia. 8 The authors described an “inappropriately normal” vitamin D level given a decreased parathyroid hormone. 8 In the present case, parathyroid hormone is also appropriately suppressed.
Glucocorticoids, such as prednisone, are an effective treatment for Mycobacterium avium-intracellulare-associated hypercalcaemia. They suppress both the inflammatory process involved in granuloma formation and 1 -α hydroxylase activity. 1 Antimicrobial therapy was not required in another case of Mycobacterium avium-intracellulare-associated hypercalcaemia 1 and has not shown obvious additional benefit in treating the granulomatous inflammation associated with Mycobacterium avium-intracellulare hypersensitivity pneumonitis (hot tub lung). 9 Furthermore, prolonged duration of treatment and associated toxicity in typical comorbid patients often preclude treatment of Mycobacterium avium-intracellulare infection or colonisation, particularly given the often indolent disease course. 10 Thus, less symptomatic patients can be observed before initiating therapy. Treatment entails combination therapy with azithromycin or clarithromycin, rifampin or rifabutin, and ethambutol with or without an intravenous aminoglycoside for one year or often longer after sputum cultures become negative. 10
In cases of unexplained hypercalcaemia associated with pulmonary infiltrates, physicians can consider underlying Mycobacterium avium-intracellulare infection, primarily in patients with AIDS and lymphoma. This is notably a rare aetiology and thorough work-up for other sources should be completed to help establish causation. Mycobacterium avium-intracellulare-associated hypercalcaemia in immunocompetent hosts seems exceedingly rare. The present case appears to be the second reported and the first associated with a normal activated vitamin D level. Although it is demonstrably uncommon, physicians can be cognizant of Mycobacterium avium-intracellulare-induced hypercalcaemia as a potential diagnosis during their evaluations.
Footnotes
Declarations
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by Peddasomayajula Subrahmanyam.