
Abstract
In multifocal findings, the possibility of multifocal osteoid osteomas should be considered and this case helps us to be attentive for the unusual radiographical presentation of osteoid osteoma.
Keywords
Introduction
Osteoid osteomas are one of the most common benign bone tumours which have a wide variation in terms of their occurrence. Osteoid osteoma is presented as the third most common benign bone tumour, after osteochondroma and non-ossifying fibroma. They are more prevalent in males. They usually occur during the second and third decades of life, with pain, swelling and local tenderness. Pain is worse at nights and relieved by non-steroidal anti-inflammatory drugs. The duration of symptoms varies from weeks to years before seeking medical attention. Osteoid osteomas usually form solitary lesions; but in only rare cases they may also be multifocal. This article describes a case of a medullary osteoid osteoma in the distal radius involving two nidi.
Case presentation
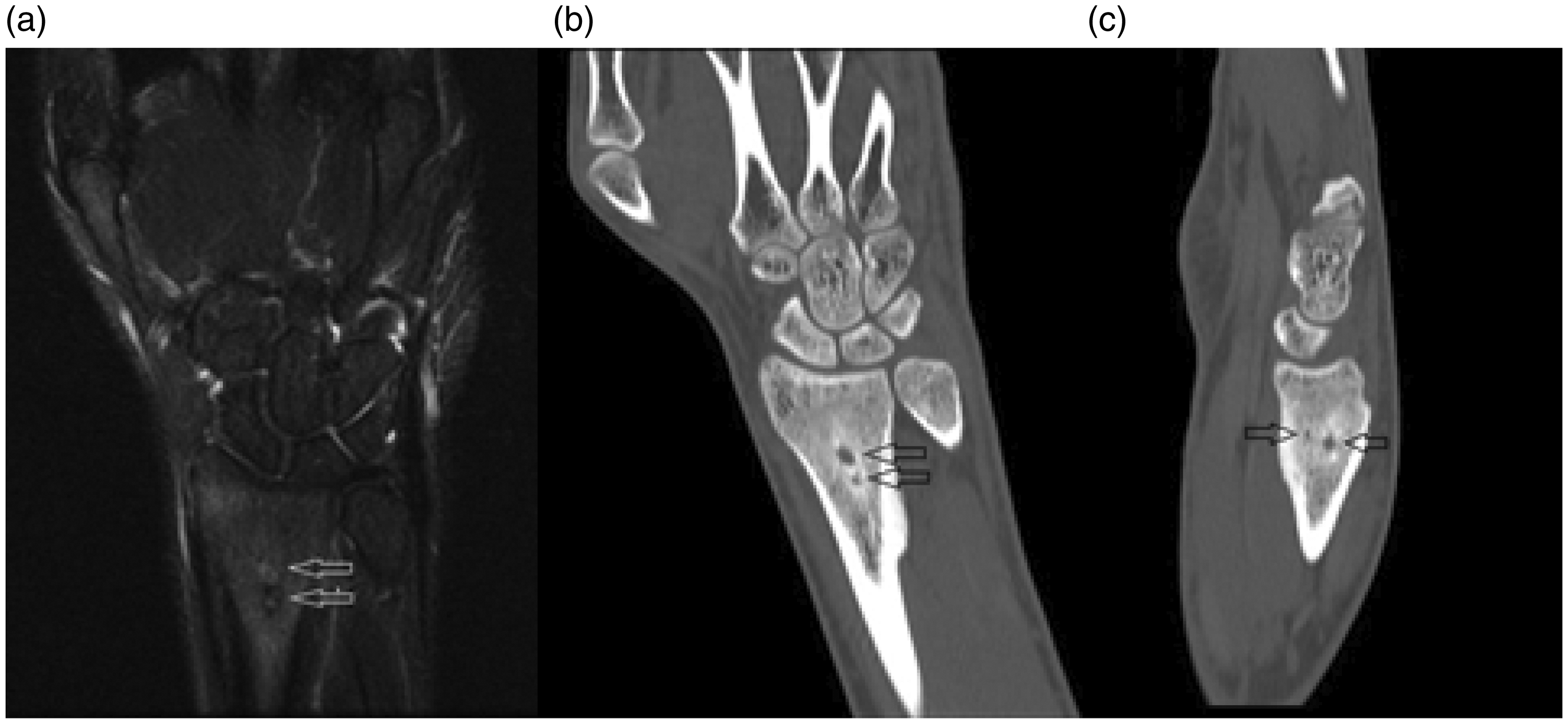
A 24-year-old male patient with pain in his left wrist for four months was seen in our orthopaedic clinics. During this time period, he started using non-steroidal anti-inflammatory drugs as a self-medication. Usually the pain was increasing during the night and decreasing after the anti-inflammatory medication. His past medical history was unremarkable, including no history of trauma or infection. Mild soft tissue swelling on the dorsal side of the left wrist was realised in inspection. His range of motion was full, but there was an intense pain with hyperflexion and hyperextension. A solid periosteal reaction with cortical thickening and fusiform expansion was seen on the plain X-rays of the left wrist (Figure 1). Both nidi were hardly visible as a well-circumscribed lucent region in the distal radius metaphyseal region. Intramedullary nidi associated with sclerosis around and cortical expansion were delineated on the computed tomography images (Figure 2(b) and (c)). Tumour nidi of low signal intensity with the surrounding oedema were also detected on T2-weighted images on magnetic resonance imaging (Figure 2(a)).
Preoperative radiographs (a and b) showing cortical expansion of distal radius with two radiolucencies (arrows). T2-weighted images of magnetic resonance imaging showing mild soft tissue oedema, tumour nidi (arrows) with surrounding oedema in medullary canal. Coronal (b), sagittal (c) computed tomography images showing two nidi (arrows) which are located in medullary canal.
Under axillary brachial plexus blockade, tourniquet was applied without using Esmarch bandage. A distal radial longitudinal approach was chosen for the left wrist. A cortical window on the distal radial bone was opened using a high-speed power burr and then the lesion was curettaged and the material was sent to pathology. The curetted cavity was filled with tri-calcium phosphate as a bone substitute. Absorbable haemostatic sponge was used to reduce the bleeding. Skin was closed and a short arm splint was applied. After postoperative radiological control (Figure 3(a)), patient was discharged from hospital on the following day. Pathologic examination showed delineated oval, reddish, gritty nodules within the spongy marrow measuring 0.2–0.5 cm in diameter which on histologic examination showed osteoid tissue with trabeculae of new bone in a vascular stroma. The pathologic findings were consistent with multifocal osteoid osteoma.
Postoperative computed tomography (a) showing the filled cavity with tri-calcium phosphate after curettage. Postoperative 11th month AP radiograph (b) and sagittal computed tomography (c).
Patient was seen in the clinics at the first, second and 11th month postoperatively. No pain and no limited range of motion were found in his orthopaedic examination.
Discussion
Osteoid osteoma was described by Bergstrand in 1930 and the definition as a clinical and pathological entity was first used by Jaffe in 1935. 1 Osteoid osteoma is a bone-forming neoplasm accounting for about 13% of all benign bone tumours. They can be described basically with characteristic clinical presentation, distinctive roentgenographic features and unmistakable pathological findings. The most common sites of involvement are usually the metaphysis and diaphysis of the long bones. 2 Osteoid osteomas are small tumours (<20 mm) usually located in the tubular bones, especially occurring in the femur and tibia (50–60%). Less common sites include humerus, foot and spine. 3 Osteoid osteoma of the wrist and hand is extremely rare. The exact location of the nidus may be obscured because of extensive cortical thickening. 1 The lesional tissue of an osteoid osteoma, known as a nidus, is always 1 cm or less in diameter. Despite its small size, nidus causes intense pain and causes an exuberant periosteal reaction. 4
Prostaglandin levels in the nidus are usually 100–1000 times higher than a normal bone and are thought to be the main reason of pain. Non-steroidal anti-inflammatory drugs inhibit the prostaglandin production and constitute the basic action of relieving the pain. As in our case, prostaglandins lead to vasodilatation and oedema in the surrounding medullary tissues, reflected as hyperintense areas on T2-weighted sequences on magnetic resonance imaging. Intra-articular prostaglandins are thought to be responsible for the related lymphofollicular synovitis. 5
Multifocal osteoid osteoma refers to the presence of more than one lesion within the same bone whereas synchronous multicentric osteoid osteoma describes the presence of osteoid osteoma in two different bones at the same time. According to the literature the multiple occurrences of osteoid osteomas have been observed in 1% of cases. Discrete synchronous multifocal osteoid osteoma is defined as different lesions in a bone that is separated by normal tissue occurring at the same time.
Osteoid osteomas have typical radiographic appearance. A small radiolucent nidus is surrounded by dense reactive bone. The location of the nidus may be subperiosteal, intracortical or subcortical. On rare occasions, the nidus is deep in the medullary canal as in our case. 4
Medullary osteoid osteomas are often seen in the femoral neck, hands, feet and posterior elements of the spine. Medullary lesions generally show mild to moderate reactive sclerosis, which may be remote from the nidus, and cause difficulty to identify the lesion radiologically. In other words, intramedullary nidus may not be apparent significantly on the plain X-rays because of minimal reactive sclerosis around the nidus. 2
Osteoblastoma, brodie abscess, chondroblastoma, eosinophilic granuloma, fibrous dysplasia, intraosseous lipoma can mimic osteoid osteoma’s radiologic appearance. Osteoblastoma can occur as an osteolytic lesion associated with extensive bone marrow oedema as well as periosteal reaction. Intramedullary and epiphyseal location of children can help differentiate chondroblastomas from osteoid osteomas. Osteoblastomas are larger (>20 mm) than osteoid osteomas and they exhibit greater osteoid production and vascularity. Osteoblastomas are most frequently located in axial skeleton and the pain is usually not worse at night and is less likely to be relieved with non-steroidal anti-inflammatory drugs. Also osteoblastomas are more likely to recur after surgery comparing to osteoid osteomas. Small osteoblastomas often contain a central calcification, similar to osteoid osteomas. 6 Histopathologically, the lesion showed uniform, osteoblastic cells with pale-staining nuclei, minimal pleomorphism and minimal mitotic activity. 7
A Brodie abscess of chronic osteomyelitis can occur with a radiolucent centre and surrounding reactive sclerosis. Also bone enlargement in long bones can be seen radiologically. Erythrocyte sedimentation rate and C-reactive protein levels are elevated in roughly half of the cases and may indicate active infection. Microscopic evaluation of the abscess material usually reveals necrotic tissue with an acute or chronic inflammatory infiltrate. 3
Intraosseous lipoma is a benign bone tumour seen at any age with a peak frequency in the fourth decade. Most of the cases involve the lower limb. The radiologic appearance is a geographic area of osteolysis with well-defined margins and a partial or complete marginal sclerosis in 45% of the cases. An intralesional calcification or ossification, usually in a central location, was present in 42% of the cases. Computed tomography or magnetic resonance imaging demonstrates the characteristic fat content. 8
Cartilaginous tumours often demonstrate multiple minute calcifications. Only small chondromas are likely to appear as a lytic lesion with a single central calcification. Histologic features include lobules of hyaline cartilage with frequent areas of hypercellularity, binucleate chondrocytes and focal mild cytologic atypia. 9
Langerhans cell histiocytosis manifests in a variety of ways, the most common being the eosinophilic granuloma, a localised and often solitary bone lesion that occurs predominantly in the paediatric age group. Although solitary Langerhans cell histiocytosis can arise in any bone, more than half of the cases occur in the skull, pelvis, mandible or ribs. Long and flat bones can be affected in children, and patients older than 20 years. Only a few cases manifest as an osteolytic lesion of the left pubic bone containing a central minute sequestrum with a cortical endosteal scalloping. Histologic features include dense or scattered foci of mononuclear histiocytes. 10
Non-surgical management of osteoid osteoma involves the use of aspirin and non-steroidal anti-inflammatory drugs for pain management. Over time, the lesion may burn out and pain symptoms can resolve. This process may take several years to occur. Radiofrequency ablation is one of the treatments for osteoid osteoma. But radiofrequency ablation requires a safe margin of distance from neurovascular structures to prevent iatrogenic thermal damage. Proximity to neurovascular structures may result in insufficient treatment. Surgical management, excision of the nidus by using fluoroscopy is usually curative but bone grafting may be required to fill the bone defects. 8 Surgical excision carries the risk of pathological fracture as the cortical defect acts as a stress riser. Multifocal osteoid osteomas can weaken the bone further and the effected limb may need to be protected until the cortical healing occurs.
Conclusion
Multifocal osteoid osteoma is an extremely rare bone lesion. In multifocal lesions, the possibility of multifocal osteoid osteomas should be considered in differential diagnosis. This case may help us to be attentive for the unusual radiographical presentation of osteoid osteoma, as their early recognition is important to guide an appropriate management.
Footnotes
Declarations
Acknowledgements
None
Provenance
Not commissioned; peer-reviewed by Hisanori Fukunaga