
Abstract
Objectives
To measure and establish a baseline assessment of the patient safety culture in the Palestinian hospitals.
Design
A cross-sectional descriptive study using the Arabic version of the Safety Attitude Questionnaire (Short Form 2006).
Participants
A total of 339 nurses and physicians returned the questionnaire out of 370 achieving a response rate of 91.6%.
Setting
Four public general hospitals in the Gaza Strip, Palestine.
Methods
Nurses and physicians were randomly selected using a proportionate random sampling. Data analysis performed using Statistical Package for the Social Sciences software version 20, and p value less than 0.05 was statistically significant.
Main outcomes measures
Current status of patient safety culture among healthcare providers and percentage of positive attitudes.
Results
Male to female ratio was 2.16:1, and mean age was 36.5 ± 9.4 years. The mean score of Arabic Safety Attitude Questionnaire across the six dimensions on 100-point scale ranged between 68.5 for Job Satisfaction and 48.5 for Working Condition. The percentage of respondents holding a positive attitude was 34.5% for Teamwork Climate, 28.4% for Safety Climate, 40.7% for Stress Recognition, 48.8% for Job Satisfaction, 11.3% for Working Conditions and 42.8% for Perception of Management. Healthcare workers holding positive attitudes had better collaboration with co-workers than those without positive attitudes.
Conclusion
Findings are useful to formulate a policy on patient safety culture and targeted a specific safety culture dimension to improve the safety of patients and improve the clinical outcomes within healthcare organisations.
Introduction
Errors are certain to happen in human life. 1 In health settings, work is complex in nature making it vulnerable to errors. The Institute of Medicine (IOM) disseminated an alarming report on practitioners’ errors in which most of them were preventable. 2 It suggested that promoting safety necessitates changes in the culture of work setting toward recognising errors as a guide for improvement not for blaming employees. After the ‘To Err is Human: Building a Safer Health System’ of IOM, the quality of care and patient safety have received extensive attention and became a priority in any healthcare system. 3 Safety culture is a fundamental element when seeking improvement or quality in healthcare. It is defined as shared values, attitudes and perceptions of safety within an organisation toward minimising patient harm. 4 It includes the following components: (1) recognising high-risk setting as errors prone in nature, (2) free blame environment, (3) management involvement in allocating resources for safety concern and (4) collaboration among disciplines to seek solutions. 5 Organisations with positive safety culture are characterised by mutual trust communication, shared perception around safety and by confidence of effectiveness of preventive measures. 6 This is compatible with Davies and his colleagues’ 7 presentation of culture ‘the way we do around here’.
Employees with positive safety culture are more likely to engage into safety-related behaviours when compared to those with perceived negative safety culture. 8 In healthcare, safety culture has been associated with quality, safety performance, safe practices and clinical outcomes including workplace accidents, falls and medication errors.8,9
Assessment of safety culture is used by healthcare organisations as an opportunity to determine areas for patient safety improvement, evaluate successful patient safety interventions, benchmark and meet regulatory requirements. 10
In order to promote the culture of safety around patients, it is fundamental to assess the safety culture first as a preliminary step toward looking for better outcomes. The body of literature shows that safety culture differs across hospital organisations and depends on organisation experience, size and function.11,12
In Palestine, one out of seven patients suffers harm. 13 To date, understanding safety culture and contributing affecting factors within the Palestinian public hospitals are limited. Studying the safety culture of an organisation can be useful to have knowledge and insight into patient safety. The aim of this study was to have a baseline data on patient safety culture among a representative sample of physicians and nurses from Palestinian public hospitals in the Gaza Strip. For these purposes, the Arabic version of the Safety Attitude Questionnaire was used. We hypothesised that nurses and physicians have different perceptions of safety culture and healthcare workers holding positive attitudes are more likely to exhibit good collaboration with their colleagues (nurses, physicians and pharmacists). Findings from this study could be a chance to better understand the extent to which patient safety attitudes are present in Palestine.
Materials and methods
Setting
This study was carried out in four public general hospitals selected randomly from a total of seven hospitals distributed in the four Gaza Strip governorates. Where a governorate had more than one hospital (North and South), randomisation was applied in order to have a representative sample from the entire Gaza Strip. All hospital inpatient wards were included in the study. The hospital wards were classified into surgical, internal medicine, maternity and intensive care unit.
Design and sample
A descriptive cross-sectional design was used to gather data from a total of 370 physicians and nurses. The total number of physicians and nurses in the four selected hospitals was 1294. A proportionate systematic sampling was followed to select the sample size. Subject recruitment was carried out by the researchers visiting each hospital administration. First, we explained the research aims and then asked for the exact number of nurses and physicians who met the criteria. They should be formal employees with at least six months’ working experience, and willing to participate in the study. Interns, volunteers and newly employed nurses or physicians were excluded. We calculated the exact proportion from total sample in each hospital and in wards then we wrote a list of eligible participants’ names in each ward to select the required number systematically. The Kth was equal to 4, and questionnaires were distributed accordingly. Epi Info program was used to calculate the sample size with 95% confidence interval which was estimated to be 370.
Measures
The Safety Attitude Questionnaire (SAQ) (Short Form 2006) developed by Sexton et al. 14 measures the perceptions and attitudes of frontline providers on patient safety. It covers six dimensions: Teamwork Climate, Safety Climate, Job Satisfaction, Stress Recognition, Perception of Management and Working Condition with a response scale ranging from 1 (disagree strongly) to 5 (agree strongly). Items 2 and 11 are reverse items.
The SAQ (Short Form 2006) was translated into Arabic and tested for psychometric properties. The Item content validity index and the scale content validity index ranged between 0.77 to 1.00 and 0.85 to 0.97, respectively. Internal consistency was measured with the Cronbach alpha and the half-split technique. Overall Cronbach alpha value was 77.7 (74.7–82.2). The half-split technique tested by the Intra-Class Correlation and Gutman split-half coefficient and were 0.846 and the results 0.927, respectively (0.669–0.919 and 0.727–0.927, respectively). Construct validity was tested by the confirmatory and the exploratory factor analysis and showed satisfactory model of fit.
The Arabic version was slightly modified; item 36 ‘Communication breakdowns that lead to delays in delivery of care are common’ was not part of the scale but was added to Working Condition, and item 29 ‘The levels of staffing in this clinical area are sufficient to handle the number of patients’ was moved to Working Condition because these items are essential elements of workplace safety in Palestinian culture. Extra items were added to identify respondents’ demographic information (gender, age, years of experience, place of work and department, education level and working hours). Items 33–35: ‘I experience good collaboration with staff physicians in this clinical area’; ‘I experience good collaboration with nurses in this clinical area’ and ‘I experience good collaboration with pharmacists in this clinical area’ which measure safety behaviours were added for research purposes.
Data collection
The Arabic SAQ was distributed to physicians, and nurses met the inclusion criteria. Face to face interview approach was followed to fill out the questionnaires through the help of six trained nursing students. Data collection lasted for 10 months from June 2013 to March 2014.
Ethical consideration
The study was approved by the Palestinian Helsinki Ethics Committee in the Gaza Strip (PHRC/HC/01/14). In addition, permission was obtained from the Palestinian Ministry of Health (HRD/231/10/14). Information about study objectives was provided to each participant. Participation was voluntary with the right to withdraw any time. Participants were asked to give their consent by signing on the cover page of the questionnaire. All answers were de-identified to maintain confidentiality and placed into close closet of the researchers.
Statistical analysis
Data collected from the survey were analysed with SPSS version 20. The demographic data and the scores of the patient safety culture dimensions were summarised using descriptive statistics. The three negatively worded items (2, 11 and 36) were reverse scored. Frequency analyses were performed to identify missing data and outliers. For each item, we calculated the mean score (5-point scale; 1 minimum; 5 maximum), the standard deviation of the mean, the percentage of positive score (percent of survey items receiving a score ≥ 4) and percentage of negative score.
A Chisquare test was used to examine the variation in the subscale scores across sites. Safety subscale scores were compared between professional groups (physicians vs. nurses). Each item was scored by converting the 5-point Likert scale to a 100-point scale, and positive responses in the positively worded survey items were ‘agree/strongly agree’, and those in the negatively worded items were ‘disagree/strongly disagree’.
One way ANOVA test was used to compare the mean scores of more than two categorical groups, and post hoc tests were conducted to identify the differences when the ANOVAs were significant. Wald Chi-square test was used to test the statistical significance between the Arabic SAQ dimensions and safety behaviour items. All analyses used a significance level of p < 0.05 and 95% confidence interval.
Results
Respondents’ characteristics
Socio-demographic characteristics of participants.

ICU: intensive care unit.
Assessment of the patient safety culture
Comparison of SAQ items mean and SD with different similar studies.

%MVs: percentage of missing values; M: mean score; SD: standard deviation; R*: reverse question; N/A: not available.
Item responses
Percentage of agree, disagree and neutral responses.

Variations in patient safety culture
Comparison of subscales of the safety attitude questionnaire (mean ± SD).

M: mean score, SD: standard deviation, p < 0.001.
Relationship with safety-related behaviours
Relationship between safety behaviours questions with SAQ dimensions.
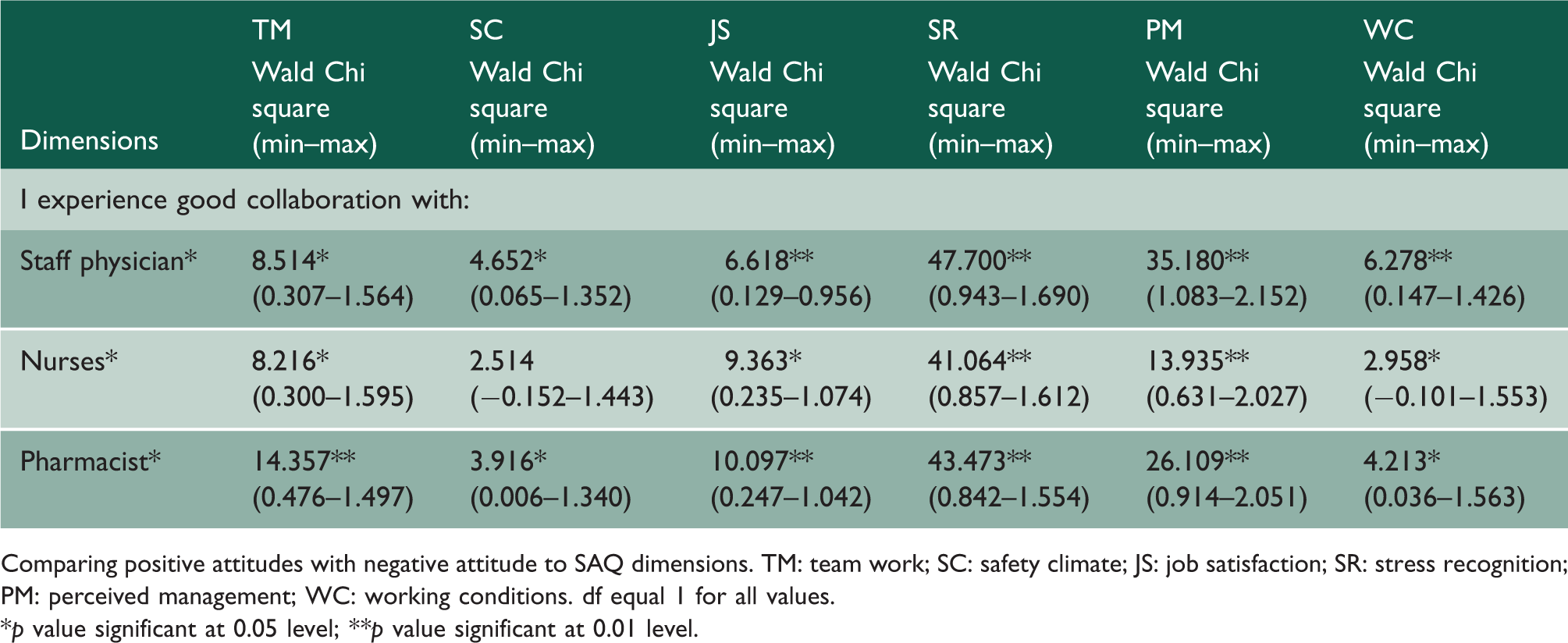
Comparing positive attitudes with negative attitude to SAQ dimensions. TM: team work; SC: safety climate; JS: job satisfaction; SR: stress recognition; PM: perceived management; WC: working conditions. df equal 1 for all values.
*p value significant at 0.05 level; **p value significant at 0.01 level.
Discussion
Key findings
We aimed to assess the safety culture status quo in the Palestinian hospitals, and we hypothesised that there is variation between nurses and physicians, and healthcare workers with a positive attitude are more likely to show good collaboration with their colleagues. Job Satisfaction was the most perceived factor influencing patient safety, followed by Teamwork Climate and the findings proved the hypotheses.
Comparison with prior literature
We found a significant variation in the overall safety culture and in the mean scores of each dimension among hospitals, wards and between professionals. This result is consistent with another finding. 18 Nurses scored higher than physicians, and the variation was significant across all dimensions but not for Stress Recognition, similar to Poley et al. 19 Possible explanation could be that the physicians are usually exposed to rigorous training and prolonged exposure to critical care interventions which may have probably contributed to higher stress resilience and are more aware of risk of error commitment when they are fatigued, despite the important role of nurses in patient care. The variation in scores between nurses and physicians may possibly be due to personal characteristics like level of education and nature of job in which nurses have more experience in dealing with patients’ medical conditions. Another explanation could be that the concept of patient safety is in the nurses’ minds and nurses are much more confident to deal with obstacles and difficulties related to safety issues, which is in line with Fitzpatrick et al., 20 who stated that nurses are usually more positive toward patient safety culture dimensions.
Overall, Job Satisfaction and Teamwork Climate were the two most highly rated subscales in our study, similar to previous studies.10,21 The substantial variability of safety culture study among front line caregivers was in Job Satisfaction, followed by Teamwork Climate as stated by Colla et al. 10 The positivity toward Job Satisfaction indicates that participants are reasonably satisfied with their job and will be positively involved towards accepting and implementing future Quality Improvement Initiatives. The importance of job satisfaction cannot be ignored because it is imperative, can improve staff enthusiasm, and stimulate productivity as well as quality of work. 22 Dissatisfaction may distract nurses and physicians from their patients, fail to provide proper care and increase turnover in the sector, which can also jeopardise patients.
The influence of teamwork should not be underestimated. Many studies had linked a concrete relation between teamwork and patient safety with regard to communication and collaboration between unit team and teamwork climate. Accumulating findings have demonstrated the improvement in teamwork can significantly improve patient outcomes and decrease avoidable errors.23,24 Teamwork Climate received the second highest mean score with 34.5% of positive responses which is lower than previous findings.18,25,26
One of the dimensions, ‘Working Conditions’, presented the biggest weakness in the professional evaluations. Nurses and physicians express that the levels of staffing are not sufficient to deal with the number of patients, training of new personnel is not well developed. This could increase the risk of incidents that can cause harm to the patients.
The proportion of respondents who showed positive attitude (scores ≥ 75 on 100-point scale) was less than 50%. Comparing our findings to previous studies,21,25,26 the percentage of positive responses in our study was similar to Lee et al. 26 According to high-reliability organisation theory, achieving high reliability requires a safety culture that is highly uniform in both safety attitudes and experiences. 27 This means, everyone must practise the safety principles and its appropriate behaviours.
This study showed an association between safety culture and health workers’ safety behaviours in terms of collaboration with co-workers (physicians, nurses and pharmacists) which is in line with findings of Lee et al. 26
Policy and management implications
In the light of the present findings, initiating policies to address issues like improving working conditions and the perceived inadequate staff levels, develop acceptable standards for patient safety system, and implement interventions targeted to reduce the impact of these factors on the quality of hospital care are needed. The variation of safety culture perception among participants could be a guide to management, either the hospitals or the units, to improve the safety culture and workforce perception of safety. Many studies supported the evidence about strong relationships between improving organisational safety culture and patient safety and clinical outcomes. Therefore, the Joint Commission on the Accreditation of Healthcare Organizations in USA and the National Patient Safety Association in UK suggested regular safety culture surveys for safety improvement in hospitals. 23 It addressed the need for unit based safety programmes as a means to improve health workers’ perception of safety and improve safety climate. 28 Examples of unit based safety programmes can be: introducing leadership work round, improving working communication, enhancing teamwork practice, providing training for new staff and making level of staffing enough and adequate. 23
Strengths and limitations of study
This study has many strengths, including the high response rate which was not reported before; our response rate was over 90% compared to previous studies where the rate was between 50% and 78%.11,14,26 This could be down to the method of data collection, face to face interview being superior to self-administered questionnaire which enhanced the response rate. Also, we chose to use the SAQ, the most rigorously tested instrument to measure the safety climate, which provides a snapshot of a safety culture. The methodology of the study is excluded from selection bias due to the approach followed in selecting participating hospitals, nurses and physicians. Two limitations are reported: first, this study analysed the safety culture by measuring the attitudes of physicians and nurses. However, attitudes and real behaviour are not similar. It would be worth employing a triangulation methodology, combining the SAQ with other methods to study safety culture, such as field observations, focus group discussions and analysis of an organisation’s incident history. Another limitation is the inability to generalise the results to excluded private and specialised hospitals due to the nature and character of their differences from the general hospitals.
Conclusion
This study provides a benchmark data for safety culture and a useful reference to formulate policies related to patient safety. There is still a space for improvement and to build a safety culture better than the status quo. Further researches are recommended towards assessment of patient safety culture in various healthcare organisations along the hierarchy of the Palestinian healthcare system to make a jumpstart action towards better patient safety.
Footnotes
Declarations
Acknowledgement
The authors are grateful and thankful to Ministry of health and hospitals for facilitating the work. Also appreciation goes to nurses and physicians who participated in the study. Many thanks to Mrs Julie Webb-Pullman and Dr Robert Spencer for their assistance in editing this manuscript. Many thanks to Tehran University of Medical Sciences (TUMS_IC) for its support.
Provenance
Not commissioned; peer-reviewed by Sondus Hassounah.