
Abstract
Dental trauma as a result of anaesthesia practice is a relevant issue concerning morbidity and litigation. The investigator aimed to consolidate pertinent information on this issue to aid in the redressal of such an occurrence. A review of this relevant literature alongwith the author’s suggestions towards the management of the various kinds of dental trauma sustained as a result of anaesthesia practice is presented.
Introduction
Dental trauma or, as a matter of fact, any intra-oral trauma caused as a result of anaesthetic practice is a relevant issue which apart from playing a contributing role to the overall morbidity of a patient can also lead to litigation issues. It is hence prudent practice to be aware of such issues and incorporate adequate measures in order to avoid causing such incidences, and in the event of such an occurrence have a plan in place to address the issue in the interest of the patient.
Methods
A literature search with the search terms ‘dental trauma anaesthesia’, ‘dental considerations anaesthesia’ and ‘dental anaesthesia’ was made utilising databases such as PubMed, Medline, ScienceDirect and GoogleScholar. From a total of 3113 results, only 7 articles in the English language were included as they dealt specifically with the issue of trauma inflicted to dentition as a result of anaesthesia practice.
Incidence
The incidence of the occurrence of dental trauma in patients undergoing general anaethesia has been reported to be 1 in 2073 (0.05%) and 1 in 2805 (0.04%).1,2
A retrospective study conducted by Rosenberg 3 states the incidence to be 1:1000 endotracheal intubations. Prospective studies however such as those conducted by Chen et al. 4 report a higher rate of occurrence in the range of 12.1%.
Incidence of dental injury. 1

Includes damage to dental restorations, prosthetic crowns, fixed partial dentures and dislodgement of veneers.
The most commonly implicated region is the maxillary anterior sextant, in particular, the maxillary central incisors are the most common victims of trauma. To be even more specific, the maxillary left central incisor has been implicated to be the most common victim of trauma from the laryngoscope blade owing to its position in the oral cavity. 4 However, one study notes that all injuries sustained were on the right side of the patient and implied that not only the laryngoscope but also the endotracheal tube insertion were to blame for dental injuries. 6
The author acknowledges the fact that intra-oral soft tissue injuries such as those to the buccal mucosa and gingiva along with injuries to the lip are far more common than those sustained by the dentition itself, it is rather difficult to quantify such injuries. A probable method to do so might be to classify the gravity of such injuries based on their depth abrasion, contusion and laceration, followed by mentioning the extent in terms of the length of tissue involvement in a laceration or the dimension of an ecchymosis. Lastly, the involvement of a vital structure such as orifice of the stensen’s duct, greater palatine artery (palatal lacerations) could be taken into account. This scheme is, however, merely suggestive.
Identification
It would be preferable, both in terms of managing morbidity and also for avoiding an awkward situation later on, for the anaethetist to be the first to identify the occurrence of a dental injury. This would ensure that the trauma is accounted for and the timely institution of appropriate measures to manage the incident. Also, it suggests the picture of a more prudent clinician later on, when the incident is discussed with the patient, instead of the patient discovering the injury leading to a confrontation and evaluation. In a study of 161,687 anaesthetic cases, 14% of dental damage was identified first by the patient or a member of the recovery staff.
Etiology
The causes of dental trauma related to general anaesthesia can be divided into those related to anaesthetic factors and those dependent on dental factors.
Anaesthetic procedure
A study by Adolphs et al. 7 states that 89% of dental injuries in anesthesia practice occurred during scheduled procedures, of which 32.9% occurred during the intubation procedure and 50% were unrelated to the intubation or extubation procedure but did, however, take place during general anesthesia. A total of 80% of such injuries were termed ‘unavoidable’ by the anesthetist. 7 Another earlier study by Warner et al. 2 stated that one half of all dental injuries in the sample size were related to laryngoscopy or tracheal intubation, and a further 23% occurred during the procedure but after intubation.
Endotracheal intubation accounts for the highest incidence of dental trauma in patients undergoing surgery under general anaesthesia. Consequently, a higher Mallampati score can be correlated with a higher occurrence of dental trauma. Patients presenting with a ‘difficult airway’ are more likely to be victims of dental trauma than those with a straightforward airway. 1
A decreased mouth opening (represented as a decreased inter-incisor gap in Mallampati Scoring) can inadvertently cause the anaesthetist to utilise the maxillary central incisors as a fulcrum in order to position the laryngoscope to obtain a satisfactory view of the glottis. Another factor to aggravate this situation is a proclination of the maxillary central incisors as is observed in Angle’s Class II Division I malocclusion (the so-called ‘buck teeth’). This sort of a malocclusion would inevitably lead to higher chances of contact of dentition with the laryngoscope blade. In fact, patients with a Mallampati score of 3 and prominent ‘buck teeth’ have been reported to experience blade-tooth contact in greater than 90% of intubations. 8
A note must also be made of patients with advanced periodontal disease which predisposes to tooth mobility and is a significant dental finding in patients about to undergo anaesthetic procedures as, simply put, a mobile tooth is more likely to be dislodged.
Emergence from anaesthesia
Massive forces can be generated as a result of clenching on part of the patient, which is a common occurrence upon emergence from general anaesthesia. Sudden forces of such magnitude can result in dental trauma, especially in cases where an oropharyngeal airway is being utilised as a bite block.
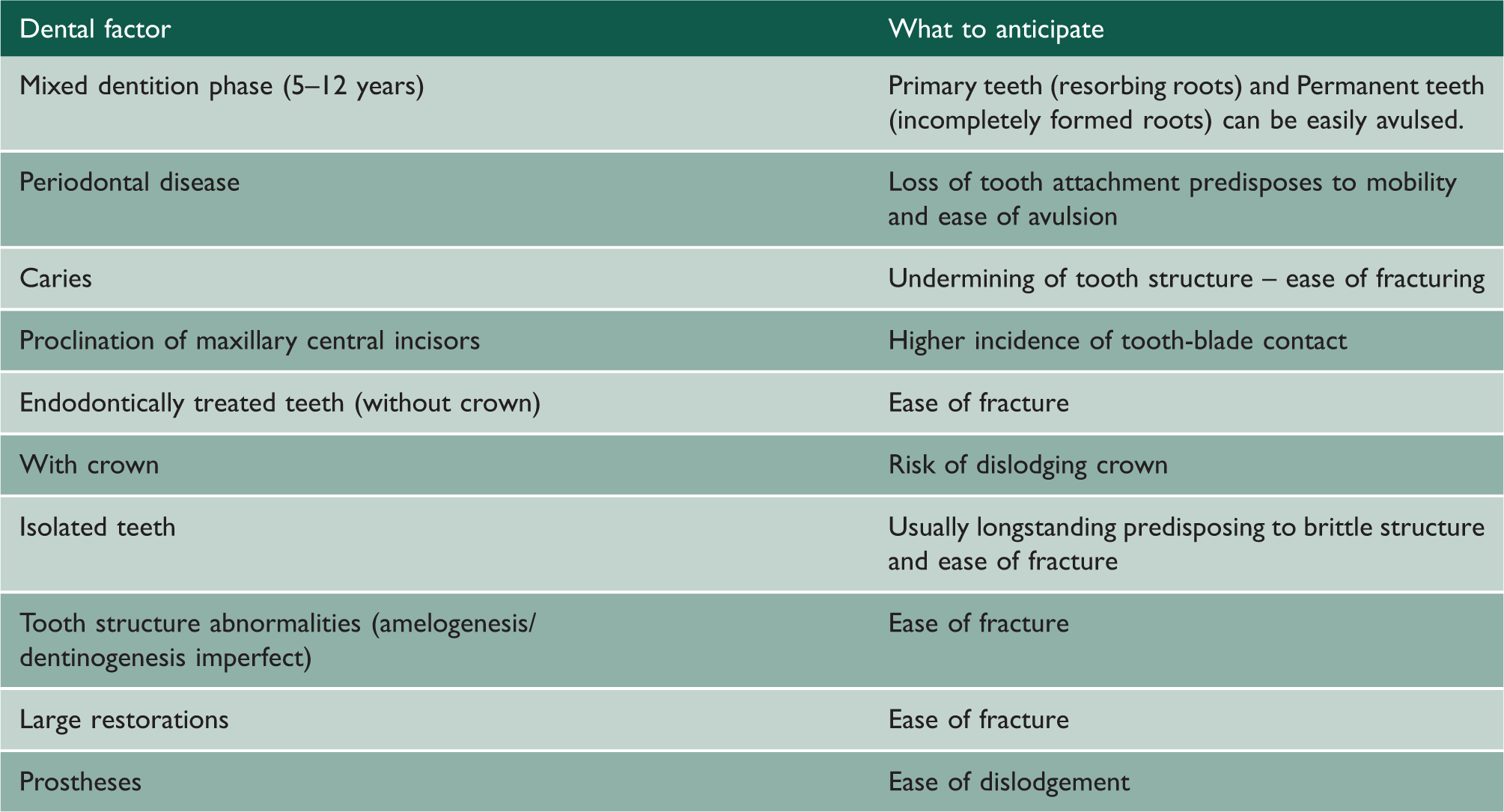
Dental factors
Dental work accounts for about 40% of injuries sustained during anaesthesia. 9
Dental factors for trauma susceptibility.
In light of these factors, every patient scheduled to undergo general anaesthesia must have a dental examination to rule out the above stated factors and ensure that none of them adds to the morbidity or creates an issue intra- or post-operatively.
A regular dental examination at the pre-anaesthetic stage must include a brief history of the patient and the procedure that he/she is about to undergo. The dental surgeon must also be aware of the type of intubation that would be performed and must keep this in mind while performing the examination. Carious lesions should preferably be restored, mobile teeth splinted/extracted prior to anaesthesia. Any loose restorations must be replaced. Some practices recommend the use of a mouthguard to protect the dentition during intubation, but it is not a reliable measure. Further, it has been noted that only when a patient is to undergo endoscopy under general anaesthesia and problems of a difficult airway are foreseen by the surgeon and/or the anaesthetist is a mouthguard deemed necessary. 10
The patient should be informed about the risks of dental trauma, and appropriate warnings must be issued wherever deemed necessary. Lastly, it is the responsibility of the anaesthetist to ensure that no or minimal dental trauma occurs to the patient. Airway instrumentation should be kept to a minimum.
Avoiding dental trauma (Table 3)
Management of dental trauma
Measures to avoid dental trauma.

Management of dental trauma.

Post-anaesthetic recovery, when the patient is awake and fully oriented, the occurrence of the incident must be discussed with the patient leaving out no detail and explaining the factors which led to the incident along with a sincere apology. This must be done in the presence of the patient’s chaperone and preferably a liaison officer of the institution and a senior anaesthetic colleague if possible. All such occurrences must be made note of in the patient’s records, and an immediate plan for dental rehabilitation should be discussed with the dental practitioner and appointments setup, so that the patient, upon discharge, is assured of the fact that the incident of dental trauma that he endured has been managed and that he shall be well taken care of in that regard.
It is also significant to mention that demographic factors such as those of age, gender, height and weight do not predilect a patient to sustain dental injury during anaesthesia; neither does the level of training of an anaesthesia resident have anything to do (statistically) with the occurrence of a dental injury. 8
Medico-legal implications
Despite the best of efforts, dental trauma can occur either inevitably or iatrogenically. Dental injuries can legally constitute both civil and criminal suits, at which point the health care professional must prove without a doubt that he/she utilised all possible precautions and acted in a manner concurrent with best clinical practice to avoid such an injury if one in fact has occurred. Pre-operative anaesthesia charting should include proper documentation of the dental/oral status of the patient in regard to the condition of his/her dentition, restorative/crown-bridgework in place, prosthetic work. These must be done alongside charting of the anaesthesia procedure to be undertaken and the difficulty of the airway. If deemed necessary, the clinician must employ protective measures such as mouthguards or putty material. Such charting allows the clinician to pre-operatively discuss potential claim-related issues with the patient beforehand and also downregulate the same by employing safety measures and prudent practice. Overall, such a practice aids in improving clinician–patient relationships and also curbs claim-related disputes.
Hence, a clinician must chart three basic factors not only to safeguard himself/herself from a claim dispute but also in the best interests of the patient:
Pre-operative dental assessment, Existence/absence of dental lesions and Incorporation of safety measures.
It must always be borne in mind that these aspects are not simply check boxes to protect oneself from a potential claimant, but instead, prudent measures to provide effective care to one’s patient.
Conclusion
The incidence of dental trauma in patients undergoing general anaesthesia is a serious issue with not only morbidity related but also medico-legal issues. The anaesthetist must not ignore the oral health of the patient and should diligently pursue a dental examination for the patient as recognition of potential risk factors can aid in eliminating the occurrence of dental injury. Awareness of iatrogenic risk factors as well as having a protocol in place for management of dental trauma would lead to better and more satisfactory patient outcomes.
Footnotes
Declarations
Acknowledgements
None
Provenance
Not commissioned; peer-reviewed by Sandra Girgis.