
Abstract
Summary
Objectives
To assess whether the effects of community-based educational interventions to improve blood pressure, weight and health behaviours benefit participants with lower educational levels more than those with higher educational levels.
Design
Secondary data analysis.
Setting
Two 12-month community-based educational interventions, one led by trained peers and one delivered by health professionals.
Participants
A total of 403 hypertensive individuals, grouped by education (high school or less; 1–3 years college; 4 + years college).
Main outcome measures
Blood pressure, weight, physical activity and fruit and vegetable intake.
Results
We found that changes in blood pressure, weight and physical activity were similar across education levels; college graduates consumed more daily servings of fruits and vegetables at baseline (3.7 versus 3.6 for those with 12–15 years and 3.1 for those with < 12 years, p = 0.0112), and increased intake more after the intervention (+0.4 versus −0.1 and −0.1, p = 0.0142). The two methods of delivery – peer-led versus professional – had similar effects on all measures.
Conclusions
We conclude that educational interventions, whether delivered by peers or professionals, may improve chronic disease self-management among participants but do not confer greater benefits on participants with lower educational levels.
Introduction
Hypertension is a common, highly treatable chronic illness, affecting 30.5% of adult men and 28.5% of adult women in the United States (US). 1 It is a major risk factor for heart disease and stroke; 69% of Americans who have a first heart attack and 77% of Americans treated for a first stroke have blood pressure above 140/90 mmHg. 2 Despite the effectiveness of drug therapy in controlling hypertension, fewer than half (46.5%) of US adults with hypertension achieve target blood pressure. 1
There is strong evidence that persons with lower socioeconomic status are more likely to have hypertension and less likely to achieve optimal blood pressure when treated.3–10 Paulsen et al. 5 investigated the association between socioeconomic status and blood pressure control in Denmark, a healthcare system with free access to care/treatment. They determined that patients who are under 65 years of age with an educational level of 10–12 years are more likely to have their blood pressure under control than patients with an educational level of <10 years. Poorer blood pressure control in low socioeconomic status populations might be due to the association between socioeconomic status and factors known to be related to blood pressure control, such as hypertension knowledge, medication adherence, diet, weight, self-efficacy and social support.6–10
Numerous studies suggest that educational interventions can improve hypertension knowledge, health behaviours, and blood pressure control.11–13 Researchers have shown a particular interest in interventions delivered by peer educators, which show promise as sustainable, cost-effective adjuncts to standard clinical care, especially for chronic conditions. For example, randomised trials of commercial, largely peer-directed weight loss programmes such as Weight Watchers have demonstrated efficacy. 14 Similarly, the Chronic Disease Self-Management Program (CDSMP) developed by Lorig and her colleagues at Stanford University has improved functional status, self-efficacy, and/or healthcare use in a number of randomised trials. 15 The usage of peer support to reduce hypertension has not been studied extensively, but preliminary evaluations of the National Heart, Lung and Blood Institute-sponsored program ‘Salud Para Su Corazon (Health for Your Heart)’ provide some reason for optimism. 16
Given the evidence for the effectiveness of educational interventions in improving health behaviours, we hypothesised that such interventions might particularly benefit individuals with less education, since part of the disparity in hypertension prevalence and control is explained by differences in lifestyle-related risk factors.6,8 Moreover, we hypothesised that blood pressure education delivered by trusted peers might be more effective than education delivered by health professionals, since peers are likely to convey health information in a less academic, more comprehensible manner. 17
To test these hypotheses, we performed a secondary analysis of data from a randomised trial comparing two types of educational interventions promoting hypertension self-management among hypertensive Veterans: one delivered by trained peers and one delivered by health professionals. We first determined whether changes in blood pressure and lifestyle were related to participants' education. We then examined whether the relative effectiveness of peer-led versus professionally delivered education varied by level of education.
Methods
Study overview
We conducted a secondary analysis of data from POWER II, a cluster randomised controlled trial. In that study, hypertension control improved in both groups and the impact of the two interventions was similar overall. 18 For the present analysis, we compared the change in blood pressure control, weight and health behaviours during the intervention period among participants with different levels of education. We then examined whether there was an interaction between the intervention's delivery mechanism (peer-led versus professionally led) and participants' educational level. The Zablocki Veterans Affairs Medical Center's Human Studies Subcommittee (IRB) approved the randomised controlled trial and our secondary data analysis (9392-08H); participants in the randomised controlled trial provided written informed consent.
Description of POWER II
POWER II participants were recruited from individual units of various Veterans' service organisations (e.g. American Legion, Veterans of Foreign Wars) in Southeast Wisconsin. These local units (typically called posts) meet monthly to conduct organisational business; 58 posts agreed to participate. All participating posts were provided with an automated blood pressure monitor, weight scale and pedometers. For the peer-led intervention, volunteer post members were trained to deliver 10-min educational sessions about blood pressure self-management at each monthly meeting for a total of 12 sessions. For the professionally delivered intervention, participants were invited to attend three 90-min self-management seminars that were held once per quarter and variously led by a physician, a pharmacist, a combat medic and an occupational therapist. Volunteer post members encouraged attendance at these seminars. Topics covered by the peer leaders in monthly sessions and those covered by the health professionals in the seminars were similar, including exercise, diet and the importance of blood pressure monitoring.
Randomisation occurred at the post level. Prior to alerting the posts of their random assignment, 404 hypertensive post members were recruited to participate in a study of the effect of the intervention on blood pressure control. Among these, 219 were at posts assigned to the peer-led intervention and 185 at posts assigned to the professionally led intervention.
Measures
Trained research assistants collected the following data from POWER II's 404 study participants: (1) resting blood pressure, (2) weight and (3) survey data, which included demographic questions (such as age, race, education, income), medical history and previously validated measures of health behaviour, including fruit and vegetable intake, 19 sodium intake, 20 and physical activity levels, 21 as well as self-efficacy, 22 patient activation 23 and engagement in healthcare. 24 Details of the POWER II data collection methods have been described.18,25 One participant did not provide his educational level, leaving 403 participants eligible for this analysis.
Analysis
Baseline characteristics by level of education.

BMI: body mass index; BP: blood pressure; F&V: fruits and vegetables; METS: metabolic equivalents.
aCluster adjusted ANOVA test (general linear model using GEE) for linear education effect.
bCluster adjusted logistic regression testing a linear education effect.
cCluster adjusted logistic regression with cumulative logit link testing a linear education effect.
Change in outcomes at 12-month follow-up by educational level.
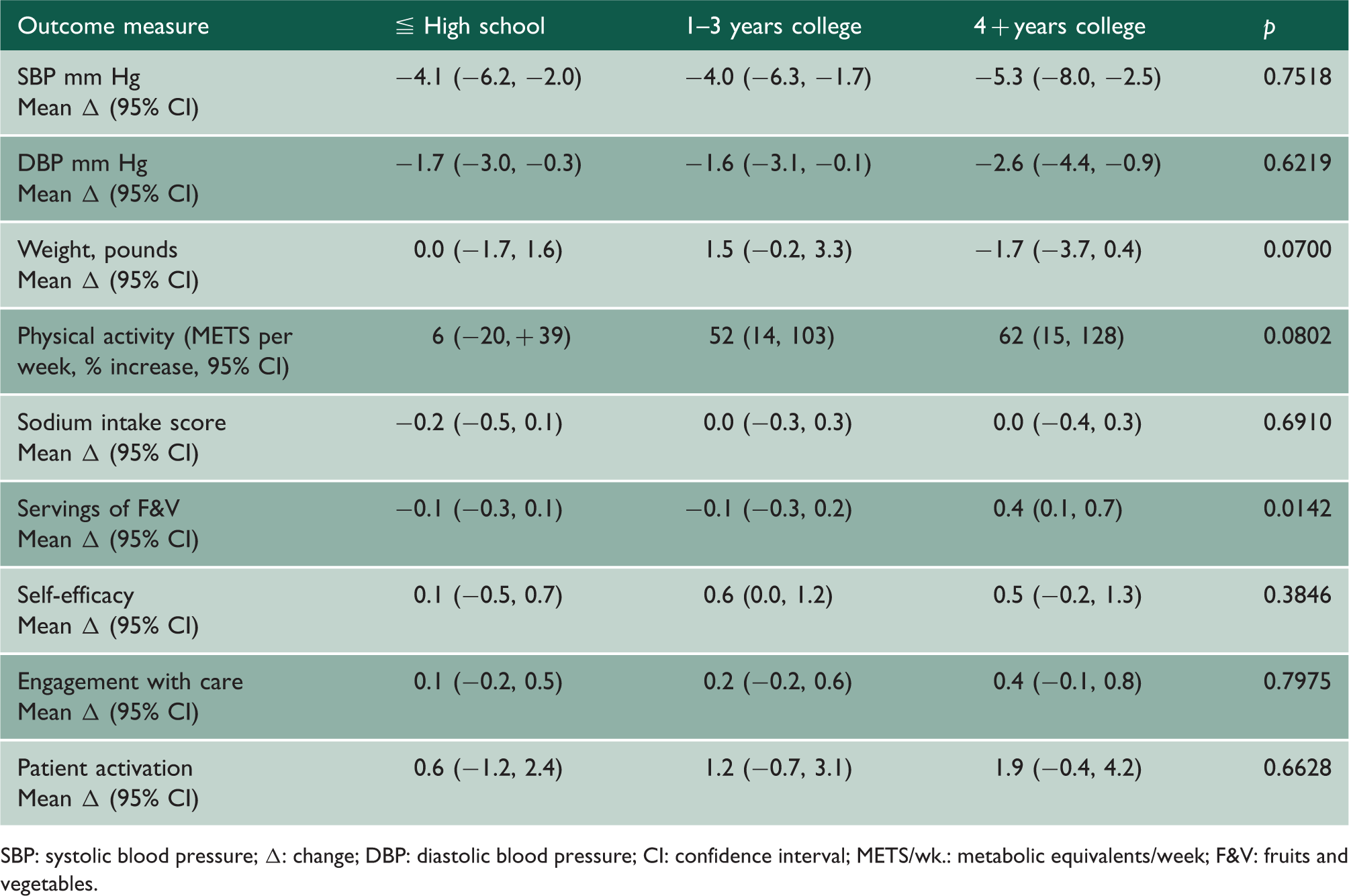
SBP: systolic blood pressure; Δ: change; DBP: diastolic blood pressure; CI: confidence interval; METS/wk.: metabolic equivalents/week; F&V: fruits and vegetables.
Change in blood pressure, weight and diet by education and intervention. a

Δ: change in measure; CI: confidence interval; SBP: systolic blood pressure; F&V: fruits and vegetables.
aThere is no significant interaction between education and intervention for any endpoint.
bThere is no significant Education-by-Intervention interaction effects for change in SBP and F&V servings (p = 0.27, 0.60).
cThere is a significant Education-by-Intervention interaction effect for change in weight (p = 0.016). Within the 4 + years college group, peer-led lost more weight than professional (p = 0.0025). Within the peer-led group, those with 4 + years college lost more weight than those with 1–3 years of college (p = 0.0015). These may be considered significant at the 0.05 level with a Bonferroni adjustment for nine comparisons.
Results
Reflecting the demographics of the participating organisations, the 403 study participants were primarily older (mean age 68.2 years), white (96%) and male (87%). Table 1 presents the baseline characteristics of participants by educational level. While baseline systolic blood pressure and weight were similar across education groups, educational level was positively associated with our measures of literacy,26,27 patient activation, self-efficacy and preference for participation in healthcare, as well as daily servings of fruits and vegetables. Conversely, educational level was inversely associated with the likelihood of smoking. Other measures were similar across groups.
At 12 months, we had data from 378 of the 403 participants; 13 died, 4 moved, 5 withdrew, and 3 were lost to follow up. Mean systolic blood pressure decreased by 4.4 mm Hg overall, while overall weight, daily servings of fruits and vegetables and physical activity were unchanged. We present changes in outcomes measures from baseline to 12 months by educational level in Table 2. The changes in systolic blood pressure, weight and metabolic equivalents/week of physical activity were similar in all education groups. However, fruits and vegetables intake improved more among participants with the highest level of education (+0.4 servings/daily) than in the low (−0.1 servings/daily) and medium education groups (−0.1 servings/daily), (p = 0.0142).
There was no pattern to the interactions between the effect of level of education and that of intervention approach on changes in the outcome measures. We present changes in systolic blood pressure, weight and daily servings of fruits and vegetables in Table 3. Although the impact of peer-led compared with professionally delivered education on weight was greatest in the most highly educated group, this pattern was not seen for other behaviour changes. Moreover, persons with the lowest levels of education had a more favourable change in weight than those with intermediate levels of education. This lack of trend is surprising, and we have no explanation other than a possible type I error.
Discussion
Principal findings
The results of our analysis do not support the hypothesis that educational interventions may be particularly useful in populations with lower levels of education; they also give no indication that persons with less education do not benefit. Across a number of outcomes, less and better educated individuals had similar changes in systolic blood pressure or health behaviours. This finding was true for both the peer-delivered and professionally delivered educational interventions. Similarly, we found no evidence that persons with less education derived more benefit from peer-delivered education than they did from professionally led educational sessions.
We note that this study had a number of strengths. We examined a range of outcomes that were either objective (blood pressure, weight) or based on validated instruments. Our educational intervention was also efficacious, generating a significant improvement in hypertension knowledge 28 during the intervention, as well as improved blood pressure control.
Several limitations of our study warrant consideration. First, our study population was relatively homogeneous – all participants were Veterans from southeastern Wisconsin; most were older white men. However, this homogeneity made it less likely that educational status would be confounded by other characteristics associated with response.
Second, we had relatively few participants with very limited education; only 26 participants did not have at least a high school education. Thus, we cannot determine how individuals with only primary education respond to an educational intervention. Furthermore, despite our effort to recruit peer educators who shared similar background and experience with the participants, our peer educators tended to be better educated than the average participants (data not shown). Nevertheless, they were members of the same relatively small (10–40 members) group of Veterans that met on a monthly basis, suggesting they were truly peers. However, due to their different educational backgrounds, they might not have delivered the material in a way that would facilitate learning among participants with less formal schooling.
Third, although our intervention duration occurred over an entire year, we were addressing long-standing behaviour patterns, and the number of educational contacts was limited. It may be that a longer or more intense intervention would do more to alleviate disparities related to educational background.
Finally, we note that our study was relatively small, so that a small difference in the impact of our intervention on blood pressure control could have been missed. However, the confidence intervals around our estimates of change in blood pressure in each educational group suggest any effect would be small.
Relation to other studies
Our study is the first to examine this question among persons with hypertension, but it is consistent with other research, which has also suggested that the impact of educational interventions is similar across educational backgrounds, and may actually be greater among persons with more education. Bosma et al. 29 found that among patients with type II diabetes mellitus or chronic obstructive lung disease and mild to moderate depressive symptoms, a self-management intervention only improved depressive symptoms among persons with more education.
Educational interventions may be unable to mitigate socioeconomic disparities in health because they fail to address important environmental factors which are associated with lower socioeconomic status. For example, individuals with less education are more likely to live in neighbourhoods with fewer stores selling fresh produce, which could result in lower fruits and vegetables intake. 30 Moreover, as seen in our study, they are likely to have lower levels of health literacy, numeracy, and self-efficacy and be less actively involved in their own healthcare. These factors may limit the impact of educational interventions directed at chronic disease self-management.
Our finding that individuals with less education did not benefit more from peer-led education contrasts with the results of Rhee et al. 17 who found that adolescents from lower socioeconomic backgrounds benefited significantly more from peer-led asthma education than the adult-led asthma education. It is difficult to compare our study with this study, which used a different form of intervention for a different disease in a different population. Moreover, the advantage of peer education in the asthma study was confined to asthma quality of life; objective measures of pulmonary function did not improve in either group. It may be that quality of life is more apt to respond to peer education. In the present study, we focused on health behaviours and blood pressure control.
Implications and future work
Despite these caveats, we believe our findings are important. In a large population of hypertensive patients, we found nothing to suggest that educational interventions alone will reduce disparities in chronic disease self-management. Indeed, similar to Bosma et al., 29 the trends we observed suggest that persons with greater baseline education are more likely to benefit from such programs, exacerbating socioeconomic health disparities.
Future studies should examine whether more intensive self-management programs, such as the 15 contact-hour peer-led Chronic Disease Self-Management Program developed by Lorig et al. 15 would diminish disparities in self-management skills. In the interim, efforts should continue to address environmental factors that make it harder for disadvantaged groups to self-manage chronic conditions.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Footnotes
Declarations
Funding
This work was supported by a grant from the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, Health Services Research and Development (Project IAB 06-086-2, Working with Veterans Service Organizations to Improve Blood Pressure).
Guarantor
JW.
Ethical approval
Trial Registration: ClinicalTrials.gov NCT00571038/
Contributorship
KZ generated the hypothesis, conducted the literature review, wrote the first draft, and provided feedback on subsequent revisions; DE performed the statistical analyses and created the tables; KE recruited, consented, and collected data from participants in the randomised controlled trial, and ensured adherence to study protocols. She edited and proofread all drafts of the paper for content and clarity; JW designed the randomised controlled trial, oversaw its conduct, and analysed and interpreted the data. He assisted KZ with the design, conduct, and write-up of the secondary data analysis. He reviewed and edited all drafts of the paper.
Acknowledgements
We would like to acknowledge the support we received from the staff in our local Research Office.
Provenance
Not commissioned; peer-reviewed by Anthony Laverty.