
Abstract
Objective
To examine patient knowledge about sudden unexpected death in epilepsy (SUDEP) compared to other risks in epilepsy. To explore patients’ experiences surrounding SUDEP disclosure and opinions on how information should be delivered.
Design
A cross-sectional questionnaire.
Setting
Royal Free Hospital, London outpatient epilepsy clinics.
Participants
New and follow-up patients attending epilepsy clinics at a London teaching hospital over six months. Patients identified as being at risk of suffering negative emotional or psychological consequences of SUDEP discussions were excluded.
Main outcome measures
Patient knowledge about epilepsy risks; patient opinion regarding source, timing and delivery of SUDEP information; impact on health seeking behaviour.
Results
Ninety-eight per cent of patients were aware of medication adherence, 84% of factors influencing seizure frequency, 78% of driving regulations, 50% of SUDEP and 38% of status epilepticus; 72% of patients felt that SUDEP information should be given to all patients. Preferences for timing of SUDEP discussions varied between those wanting information at diagnosis (40%) and those preferring to receive it after three clinic appointments (18%) to avoid information overload at the first consultation. Emotional responses (48% positive, 38% negative) predominated over measurable behavioural change following SUDEP discussions.
Conclusions
Less than half the patients knew about SUDEP and status epilepticus. Although the majority of patients with epilepsy wish to be informed about SUDEP early on in their diagnosis, information must be delivered in a way that promotes patient knowledge and empowerment.
Introduction
Sudden unexpected death in epilepsy (SUDEP) is the unexpected, witnessed or unwitnessed, death in patients with epilepsy, with or without evidence for a seizure, and excluding documented status epilepticus, drowning or trauma, with no toxicological or anatomic cause for death found on post-mortem.1,2 The incidence of SUDEP varies – it is estimated to be 0.09 to 1.2/1000 person-years in the general epilepsy population, and 9.3/1000 person-years in epilepsy surgery candidates.3,4 An increased SUDEP risk is associated with high-seizure frequency, the presence of generalised tonic-clonic seizures, 5 epilepsy duration, 6 and AED polytherapy.5,6 Strict adherence to antiepileptic drugs (AEDs) and optimal seizure control are the only widely recognised preventative measures. 7
Whether clinicians should discuss SUDEP with all patients and their family is a controversial yet important question. Those in favour of a blanket disclosure policy assert that patients have a right to fully understand the risks of their condition to inform decision-making and treatment. 8 Kroner et al. 9 found in a study of 1300 patients that over three-quarters wished to be informed about SUDEP, irrespective of their risk. 9 This is countered by a concern that patients may suffer negative psychological consequences as a result of receiving unsolicited information about a phenomenon they feel they have little control over. 10 The 2012 National Institute of Health and Care Excellence (NICE) guidelines state that health professionals should give patients tailored information about SUDEP, discuss the patient’s individual SUDEP risk and measures to reduce this risk. 11 However, there is a lack of clarity on how, when and by whom this information should be given.
Surveys in the United Kingdom, America and Canada demonstrate that a minority of clinicians discuss SUDEP with all patients with epilepsy (PWE). 10 Only 31% of UK Neurologists discussed SUDEP risk with all or the majority of their patients, with the commonest reason for disclosure being in response to patient request. 12 The main expressed reason for non-disclosure was a fear of causing patient distress.
The disparity between national guidance and current clinical practice has not been studied. Few studies have explored patient opinion in depth as a means to defining best practice regarding SUDEP disclosure. The primary objective of this study was to, therefore, describe patient opinions regarding when and how information on SUDEP and epilepsy safety should be delivered. Secondary objectives were to establish whether health seeking behaviour is influenced by knowledge about SUDEP, and in what way.
Methods
This study was approved by the NHS Research Ethics Service at the Royal Free Hospital. Three consultant epilepsy specialists and an epilepsy specialist nurse recruited patients into the study. Prior to consent, patients were provided with an information sheet that is routinely available in clinic. This covered general epilepsy-related information such as driving and medication adherence as well as specific risks such as status epilepticus and SUDEP. Consenting patients agreed to either complete the questionnaire electronically or to return it by post. A telephone reminder was performed at one and three months.
Questions were asked to identify patients’ existing level of understanding about their condition and its management. We also gathered information on how patients were informed about SUDEP, when, where and how SUDEP discussions should be made, and the impact the information has on patients’ self-management. Anonymised results from the questionnaires were stored in an encrypted database and analysed by three independent clinicians.
Participants and setting
Consenting adult (>18 years) patients with epilepsy attending the specialist epilepsy outpatient clinics at the Royal Free Hospital without intellectual disability were eligible for study. Fifty patients with variable seizure types and severity were included in the study over a six-month period. Both new and follow-up patients were included in the study to reflect a typical outpatient population. Patients whom consultants suspected as being at risk of psychological harm from participation were excluded from the study.
Results
Fifteen per cent (2/13) of neurologists at the Royal Free Hospital in London surveyed discussed SUDEP with all PWE. SUDEP was most likely to be discussed with patients with intractable epilepsy (7/13) and poor medication adherence (9/13). Common reasons for non-disclosure were time constraints in clinic (4/13) and patients perceived to be at a low risk of SUDEP (6/13).
Fifty patients of 74 (68%) consented to the study (mean age 37.4 years; standard deviation (SD) 14.32; range 20–74, 24 women, 26 men).
From the 50 patients studied, there were 12 patients with bilateral convulsive seizures, 8 with focal dyscognitive seizures, 1 focal with motor components, 3 focal with subjective sensory components, 21 focal dyscognitive evolving to bilateral convulsive seizures, 2 absence, 1 myoclonic, 1 with mixed bilateral convulsive and absence seizures and 1 with mixed bilateral convulsive, myoclonus and absence seizures.
Patients’ pre-existing epilepsy knowledge
Patients’ knowledge regarding epilepsy.

Examples of patients’ responses to the question ‘Describe what you know about SUDEP’.

Patients’ understanding of what SUDEP means
Patients were asked the open question “please describe what you already know about SUDEP?” (Table 2). Of the 25 respondents with prior knowledge of SUDEP, patients commented that the condition was rare (n = 9), that the cause was unknown (n = 8), that risk factors influenced the likelihood of it occurring (n = 6) and that it occurred during a seizure (n = 6). Two patients were under the impression that it only occurred during sleep.
Sources of SUDEP information
Of the 25 patients aware of SUDEP prior to the study, six (24%) had received information from multiple sources. Nine patients had received information from their hospital doctor or epilepsy nurse specialist (36%), others from patient information sheets (n = 2, 8%), the internet (n = 3, 12%) or newspapers (n = 1, 4%). Four patients did not respond (16%). No patients were informed about SUDEP by their GP.
Do patients feel information about SUDEP should be given to all patients?
Thirty-six of the 50 participants felt information about SUDEP should be given to all patients (72%). Of the 14 participants that disagreed with this statement, reasons for not informing patients were young age (n = 4), old age (n = 1), unstable psychological state (n = 3), patients with less severe epilepsy and thus a lower risk of SUDEP (n = 3) and no comment (n = 3).
When do patients feel they should receive SUDEP information?
Patients’ responses to ‘When do you think this information should be given?’

Patients’ responses to “What do you feel is the best way to provide patients with information about SUDEP?”

What do patients believe is the best way to receive information about SUDEP?
The majority of patients agreed that the doctor or specialist nurse should provide information about SUDEP in clinic (n = 34, 68%), suggesting that the sensitive nature of the information is best explained in person, possibly supplemented by an information sheet (Table 4).
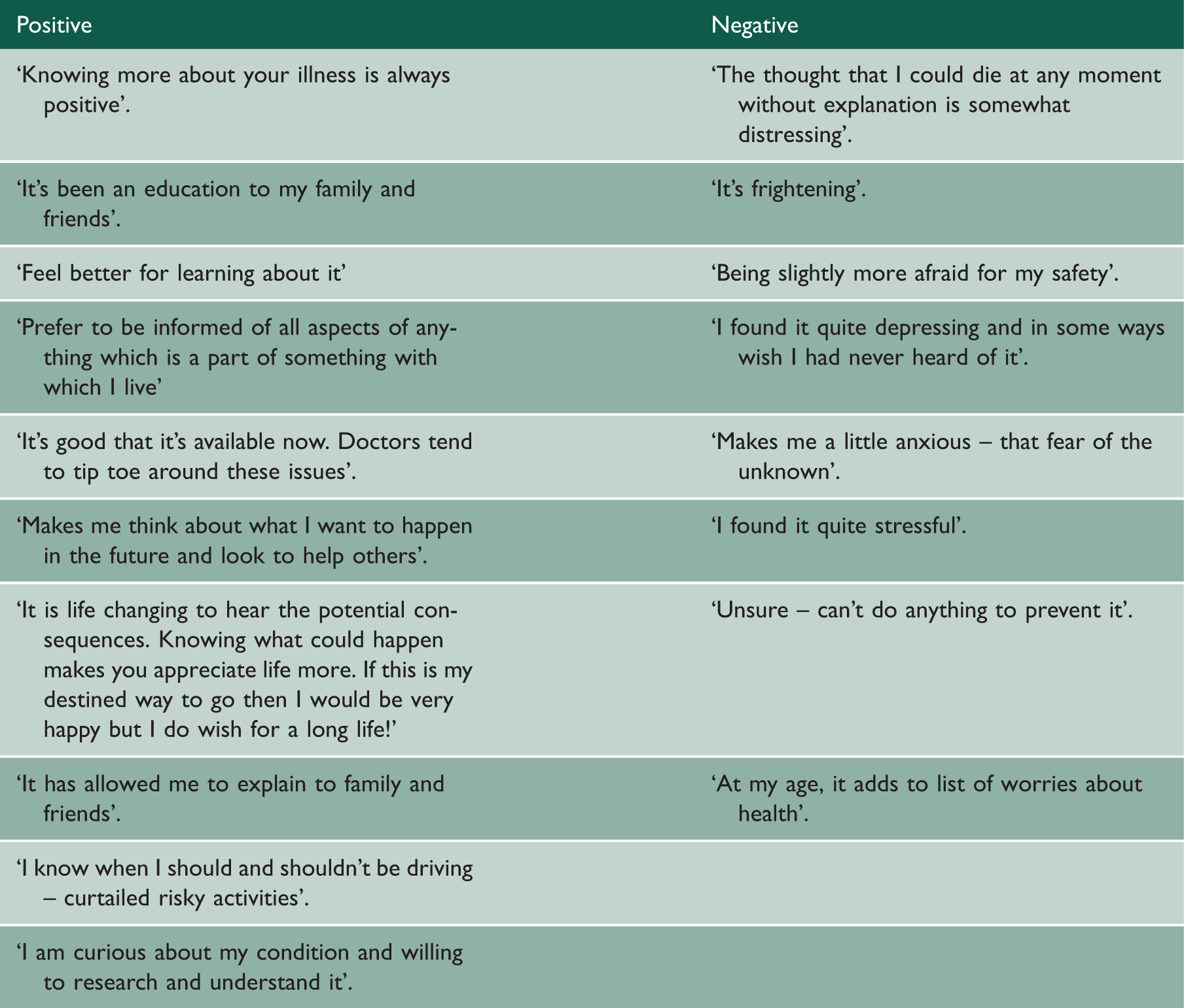
Does the provision of SUDEP information result in positive or negative consequences for patients?
Positive and negative consequences of SUDEP information.
Discussion
When exploring patient knowledge about epilepsy management in general, medication adherence, DVLA driving regulations and seizure triggers were familiar to most patients. A significant proportion of patients lack knowledge about the most serious complications of epilepsy, namely SUDEP and status epilepticus. This may reflect reluctance on the part of the health professional to discuss difficult and emotive topics, particularly given the time constraints in clinic. It is surprising that relatively fewer patients were aware of the risk of status epilepticus despite its median incidence being 40 per 100,000 life years 5 compared with that of SUDEP at 9 per 100,000 life years. 5 The relatively lower proportion of patients recalling information on status epilepticus may represent recall bias, in that SUDEP may trigger a stronger emotional response; however, it emphasises the importance of putting individual risks into perspective.
In line with other studies, 9 three-quarters of our PWE felt that SUDEP should be discussed with all patients. Patients aware of SUDEP appear to be well informed although a few believed that nothing could be done to prevent SUDEP and seemed unaware of the relative risks.
The most commonly expressed preference for receiving SUDEP information appeared to be at the point of diagnosis from the patients’ hospital doctor or specialist nurse. Patients commented that although SUDEP information might alarm patients, it was important for patients to be aware of potential dangers. Such sensitive information should be delivered face to face, allowing patients to ask questions and to receive an assessment of their individualised SUDEP risk. A proportion of patients felt that information delivered at an early stage could be frightening and overwhelming although studies have suggested that this initial anxiety about SUDEP may dissipate by three months. 14 The marked variation in preferred timing of such information may reflect individual coping styles. 13 With this in mind, clinicians may have to use their discretion to gauge patient readiness for such discussions.
With regard to the consequences of receiving SUDEP information, 48% reported benefits and 38% experienced negative consequences. Not all study patients were aware of SUDEP prior to the study. Learning about SUDEP via the participant information sheet rather than a face to face discussion may have contributed to those experiencing negative consequences. This is a potential source of bias. Emotional responses, both positive and negative, predominated over behavioural change such as medication adherence, risk taking activities and seizure management. This overriding emotional response following SUDEP disclosure was also observed in studies of young persons with epilepsy.14,15
Other studies have found that patients experience negative consequences on being informed about SUDEP (43% worrying a little, 23% a lot), albeit short-lived. 8 Our own study showed that almost half of patients suffered negative consequences from SUDEP discussions and 2–7% patients and caregivers consistently state that they wish they had never been informed about SUDEP.9,14,15
Future implications – empowering patients
This study highlights the disconnect between national guidance on SUDEP disclosure and current clinical practice.
Some patients react to information on SUDEP with a degree of fatalism, believing it to be a terminal event over which they have little control. Over half the patients in one study believed their actions would not influence whether or not SUDEP would occur.9,16 This finding raises some concerns. Despite studies purporting that the majority of PWE wish to be informed about SUDEP, it would appear that this knowledge is not being translated into steps to mitigate individual SUDEP risk. This is likely to reflect poor information provision. The manner in which risks of epilepsy, including SUDEP, are relayed to patients may be fundamental to whether patients alter their health-seeking behaviour.
Instead, SUDEP information should be ‘packaged’ with information such as the importance of drug adherence and avoidance of seizure triggers. This would improve patient knowledge and place an emphasis on improved self-management skills. 16 One useful resource is a SUDEP and safety checklist mobile application (Epsmon) that both healthcare providers and PWE can use which improves awareness of safety, prompts SUDEP discussions and calculates individualised risk which may trigger early intervention. 17 As demonstrated in other fields of medicine, emphasising positive steps that can modify risks has the potential to both empower and educate patients.
Generalisability to other populations
This study was conducted in a specialist clinic, so the population may include more severe epilepsy cases than those managed in primary care, reducing its generalisability to patients with milder epilepsy. Future studies should recruit from both community and primary care settings.
Conclusion
Most patients want to know about SUDEP at an early stage of their epilepsy. Despite this, discussions about SUDEP have not demonstrated a positive behavioural change in patients’ self-management. It is therefore suggested that healthcare providers package SUDEP information with other risks in epilepsy with an emphasis on the positive steps patients can take to prevent such a tragic event from occurring.
Footnotes
Declarations
Acknowledgements
We gratefully acknowledge the help of the Royal Free Charity and our patients for their valuable contributions and insight.
Provenance
Not commissioned; peer-reviewed by Andrew Barritt