
Abstract
A seven-year-old boy died from autopsy-proven brain haemorrhage due to hypertensive vasculopathy. This emphasizes the importance of early diagnosis and therapy of hypertension in children. Brain haemorrhage is a potentially fatal complication of paediatric hypertension.
Introduction
This case report demonstrates that hypertension may be a rare and unrecognised cause of death in children. In adults, hypertension is responsible for 62% of cerebrovascular disease manifestations and 49% of ischaemic heart disease and is the number one risk factor for death throughout the world. 1 The prevalence of hypertension in childhood is estimated to be lower than 5%; however, distinctive differences in the prevalence of childhood hypertension have been reported in certain patient subgroups. 2 Paediatric hypertension is gaining attention because of its association with subclinical organ damage and tracking into adult hypertension. 3 In general, it is not known to lead to death in childhood and adolescence. 2
Case report
A male newborn presented with cyanosis and extensive metabolic acidosis, resulting in renal and hepatic failure two days after an uneventful birth. A complex congenital heart defect was surgically treated with reconstruction of the aortic arch and closure of an aortopulmonary window and atrial septal defect.
After initial recovery, the newborn showed signs of cerebral palsy with spastic tetraparesis and seizures and was also diagnosed with hypertension, most likely due to chronic renal insufficiency. Nephrocalcinosis and diffuse echogenicity of renal parenchyma with reduced medulla-cortex differentiation were visible on ultrasound. Treatment with atenolol, enalapril and furosemide was installed.
At the age of five months, cerebral magnetic resonance imaging confirmed microcephalia and multiple small old haemorrhages.
Results of blood chemistry testing at various age points.

A 24-h blood pressure monitoring was scheduled at the age of six years and seven months, but no data were found in the hospital documentation system. The family physician confirmed that the earlier antihypertensive medication has been regularly administered, while further clinical examination and antihypertensive treatment adjustment apparently have not been carried out.
At the age of seven years and four months, the boy was found in bed in an unconscious and cyanotic state. The parents and subsequently the attending emergency physician performed cardiopulmonary resuscitation, but after 60 min the boy was declared dead. As the cause of death was unclear, the public prosecutor ordered a forensic autopsy.
Autopsy
The boy had a body length of 103 cm and a mass of 10.9 kg. Atherosclerotic fatty streaks and plaque formations were noticed in the aorta, the coronary and carotid arteries.
The heart showed left ventricular hypertrophy (heart weight 120 g) and smooth yellowish plaque formations in the aortic and mitral valves. Histology confirmed mild hypertrophy.
The renal surface was irregular with multiple tiny nodular formations. Histology showed focal scarring of the renal cortex, hyaline degeneration of the glomerula, mild nephrosclerosis and minor nephrocalcinosis.
The right frontal lobe of the brain was enlarged, resulting in a midline shift from the right to the left side. Brain sections revealed an extensive haemorrhage in the right frontal white matter and the right medial basal ganglia that invaded the ventricle from laterally, leading to widening of anterior horns of both lateral ventricles and haematocephalus internus (Figure 1). The upper brainstem showed macroscopical signs of compression from dorsolaterally.
Coronal sections of the cerebrum with a large right-sided haemorrhage.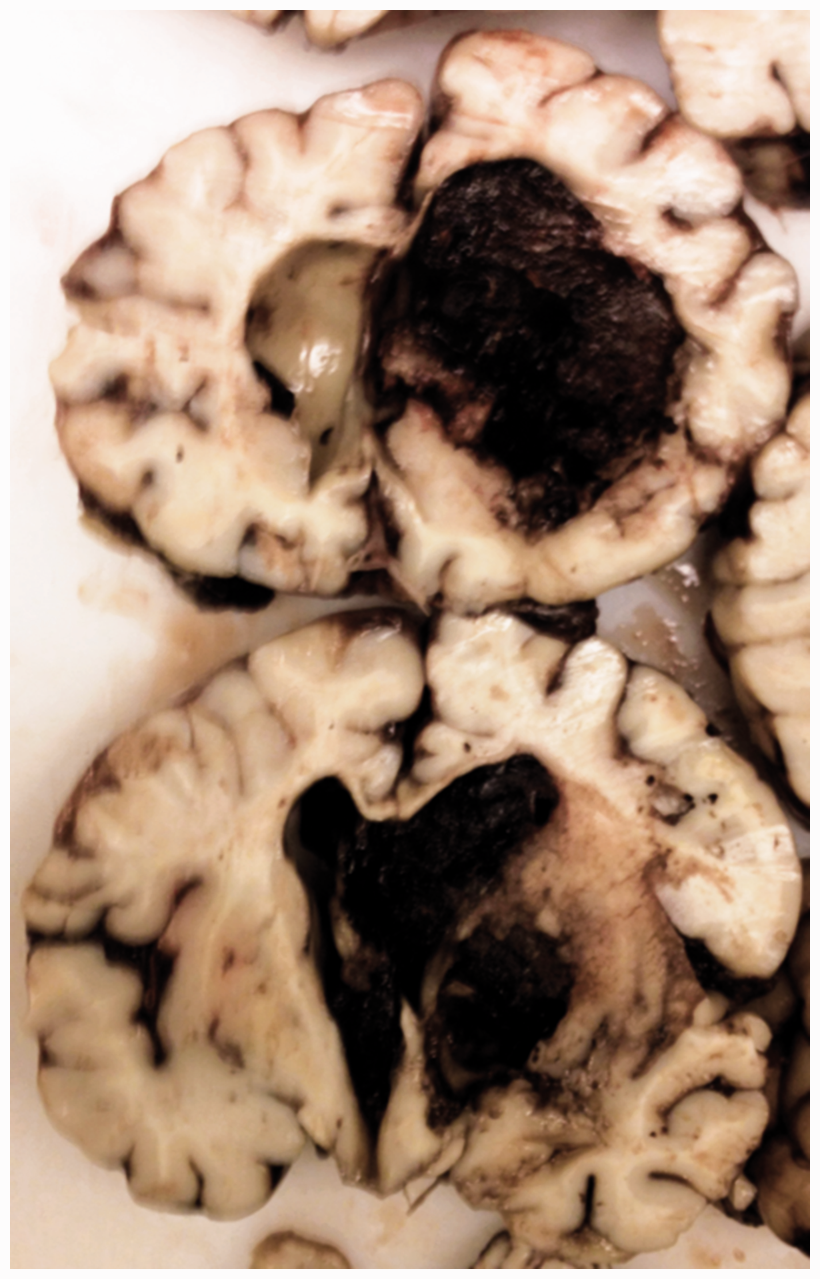
Histologic examination of the brain identified typical hypertensive lesions in small and middle sized arteries, including acute fibrinoid necrosis (Figure 2 (a) to (c)), lipohyalinosis, fragmentation and proliferation of the internal elastic lamina (Figure 2(e)) and of smooth muscle cells (Figure 2(c) and (f)), fibrotic thickening (Figure 2(d)), intimal foam cell cushions (Figure 2(g) to (i)), luminal obstruction (Figure 2(f)) and mild perivascular infiltrate (Figure 2(d)).
Histological changes of cerebral small and middle-sized vessels. (a) to (c) Fibrinoid necrosis with destruction of smooth muscle cells. (d) Fibrous thickening of vessel wall and mild perivascular infiltrate. (e) Irregularities and proliferation of internal elastic membrane. (f) Proliferation of smooth muscle cells and lumen obliteration. (g) to (i) Prominent intimal cushion of foam cells. (a) and (g) haematoxylin-eosin, (b), (d), (e), (h) van Gieson-Elastica, (c), (f), (i) immunohistochemistry for smooth muscle actin.
In concordance with clinical symptoms of cerebral palsy, extensive gliotic scarring and small calcifications were identified in the thalamus.
Discussion
This boy died unexpectedly. Autopsy revealed a fatal brain haemorrhage due to hypertensive cerebral angiopathy. This is a very unusual case that emphasises the pivotal importance of early diagnosis and therapy of hypertension also in children. There are special recommendations for antihypertensive drug therapy and long-term follow-up.4–6
There is a possibility of a genetic basis for the boy’s early problems after birth. Unfortunately, no genetic testing has been performed. The cardiac malformations were similar to, but not identical with, Berry syndrome, a rare combination of heart defects; its genetic aetiology was proposed in a case report. 7 It is likely that symptoms observed later, including the cerebral paresis with seizures, growth retardation, chronic renal insufficiency and hypertension, were complications of the initial critical situation two days after birth that prompted cardiac surgery.
Concerning fatal hypertensive brain haemorrhage in childhood, only a single case report has been published, describing a child suffering from renal arterial stenosis-associated hypertension, who finally died of a brain stem haemorrhage. This was considered a likely consequence of hypertension, although the brain was not investigated in detail. 8 Nevertheless, in the current literature, the opinion prevails that hypertension is not known to lead to death and cardiovascular disability in childhood and adolescence. 2 According to the previous report 8 as well as the present case, this point of view may be reconsidered: brain haemorrhage may be a potentially fatal complication of paediatric hypertension. With the advent of the epidemic of childhood obesity in many parts of the world and the increasing burden of paediatric hypertension,9,10 more future cases could be expected.
Footnotes
Declarations
Funding
None declared
Ethical approval
Written informed consent for publication was obtained from the deceased boy’s mother.
Guarantor
All authors are guarantors.
Contributorship
HB performed the autopsy, drafted the initial manuscript, and approved the final manuscript as submitted.
HJM performed the autopsy and contributed to the forensic casework investigation, reviewed the manuscript, and approved the final manuscript as submitted.
FCM contributed to the forensic casework investigation, reviewed the manuscript, and approved the final manuscript as submitted.
AB provided her paediatric expertise, reviewed the manuscript, and approved the final manuscript as submitted.
HBu performed the neuropathology examination, critically reviewed and revised the manuscript, and approved the final manuscript as submitted.
Acknowledgements
The Author Processing Charge for Open Access of this article was covered by the Open Access Publication Fund of the University of Salzburg, Austria.