
Abstract
Objectives
To report a qualitative study of themes doctors raised spontaneously, in a large-scale prospective cohort study covering many aspects of their medical careers, when referring to their own chronic illness or disability.
Design
Questionnaire survey.
Setting
UK.
Participants
Questionnaires were sent one, five and 10 years after graduation to 44,539 doctors who qualified between 1993 and 2012 in the UK: 38,613 questionnaires were returned and 11,859 respondents provided comments made by doctors about their training or work.
Main outcome measures
The comments of 123 doctors about their own chronic illness or disability.
Results
Main themes raised included poor support for doctors with chronic illness or disability, delays in and changes to careers (either planned ahead or imposed), the impact of pressure at work, difficulties returning to work after illness, limitations on career choices and inadequate careers advice for doctors with chronic illness or disabilities.
Conclusions
More needs to be done to ensure that doctors with chronic illness or disability receive appropriate support. Occupational health guidance should be monitored closely, with more support for ill doctors including adjustments to the job, help if needed with morale and mental health, and advice on career options. Further studies should establish the prevalence of long-term health conditions among doctors.
Introduction
Physical and mental illness among medical doctors has been documented in several studies. Stress, depression and burnout are common.1–4 ‘Sickness presenteeism’, where doctors go to work when they should take time off, is detrimental to the doctor’s own recovery, a risk to their patients’ health 5 and makes the management of sickness absence difficult. 6 However, doctors often feel pressure to continue working while ill, 7 and this can lead to acute problems becoming chronic.
The UK Medical Careers Research Group conducts prospective cohort studies of UK-trained doctors from a number of year-of-qualification cohorts. The survey questionnaires contain questions on the doctors’ career choice, work and training, and factors that have influenced them; we also invite the doctors to write comments on any aspect of their training and work if they wish. In this paper, we report on doctors’ comments about working as a doctor with, or being affected by, chronic illness or disability. In another recent paper 7 we reported on doctors’ comments about acute illness. Our aim, in the present paper, is to report on the themes that doctors raised with us when discussing chronic illness or disability. As this was a qualitative study, it was not our intention to quantify the overall scale of problems associated with chronic illness; rather, it was to report on issues raised by the doctors even if numbers affected by them were small. We hope that senior doctors, human resources staff and health service administrators will consider, in respect of these case studies, what, in their view, the right organisational responses to the reported situations should be and whether the right responses would occur in their organisations.
Methods
The Medical Careers Research Group surveyed the UK medical graduates of 1993, 1996, 1999, 2000, 2002, 2005, 2008, 2009 and 2012. The aim in our surveys is to survey each cohort (by email, web and post, offering the doctors the choice of how they would like to reply) one, five and 10 years after qualification. This study uses data from the most recent year-one surveys (cohorts 2002, 2005, 2008, 2009 and 2012), year-five surveys (cohorts 1999, 2000, 2002, 2005) and year-10 surveys (cohorts 1993, 1996, 1999, 2000 and 2002). Non-respondents received several reminders. Full details of the methodology are described elsewhere. 8
Our surveys were multipurpose and mainly contained closed questions about career choices, about career progression, and about experiences and attitudes. At the end of each survey questionnaire, in a section headed ‘Additional Comments’, we asked respondents to ‘Please give us any comments you wish to make, on any aspect of your training or work’. The request was accompanied by a large blank box for responders to write comments in their own words; the equivalent online version of the surveys featured a large scrolling text box to collect extended comments. The researchers assured doctors that their individual comments would remain confidential, and any identifying information was redacted. All handwritten comments were transcribed into our database exactly as written and were combined with the electronic comments entered directly by web responders.
A strategy based on keyword search, supplemented by inspection of individual comments, was used to identify comments which were relevant to working as a doctor while chronically ill or disabled. The criteria and process used are described in Appendix 1.
The identified comments were read by two researchers and a coding scheme was developed iteratively which reflected the main themes raised. The researchers identified six main themes. Each researcher independently coded the comments, allocating up to five themes per doctor’s comment (if more than one theme was raised). Any inter-coder differences were resolved through discussion.
Illustrative quotes for each theme are presented. We have endeavoured to provide quotes which are representative of the themes raised, and we report the frequency with which each theme was raised.
The analysis was undertaken in Microsoft Excel and SPSS. Quantitative data were analysed by univariate cross-tabulation and χ2 statistics.
Results
Response
Questionnaires were sent to 44,539 doctors. The cohorts ranged in size from 3671 graduates in 1993 to 6795 graduates in 2008. Excluding doctors who declined to participate, were known to have died, or were untraceable (939 doctors), the response rate was 53.1% in year one (14,560/27,414), 59.4% (12,624/21,254) in year five and 61.6% (11,429/18,556) in year 10.
Of the doctors who provided comments on any topic (11,859), 123 made reference to what we classified as chronic illness (96) or disability (27).
Frequency of themes
Frequency distribution of coded comments made by the doctors one, five and 10 years after graduation (N = 123 † ).
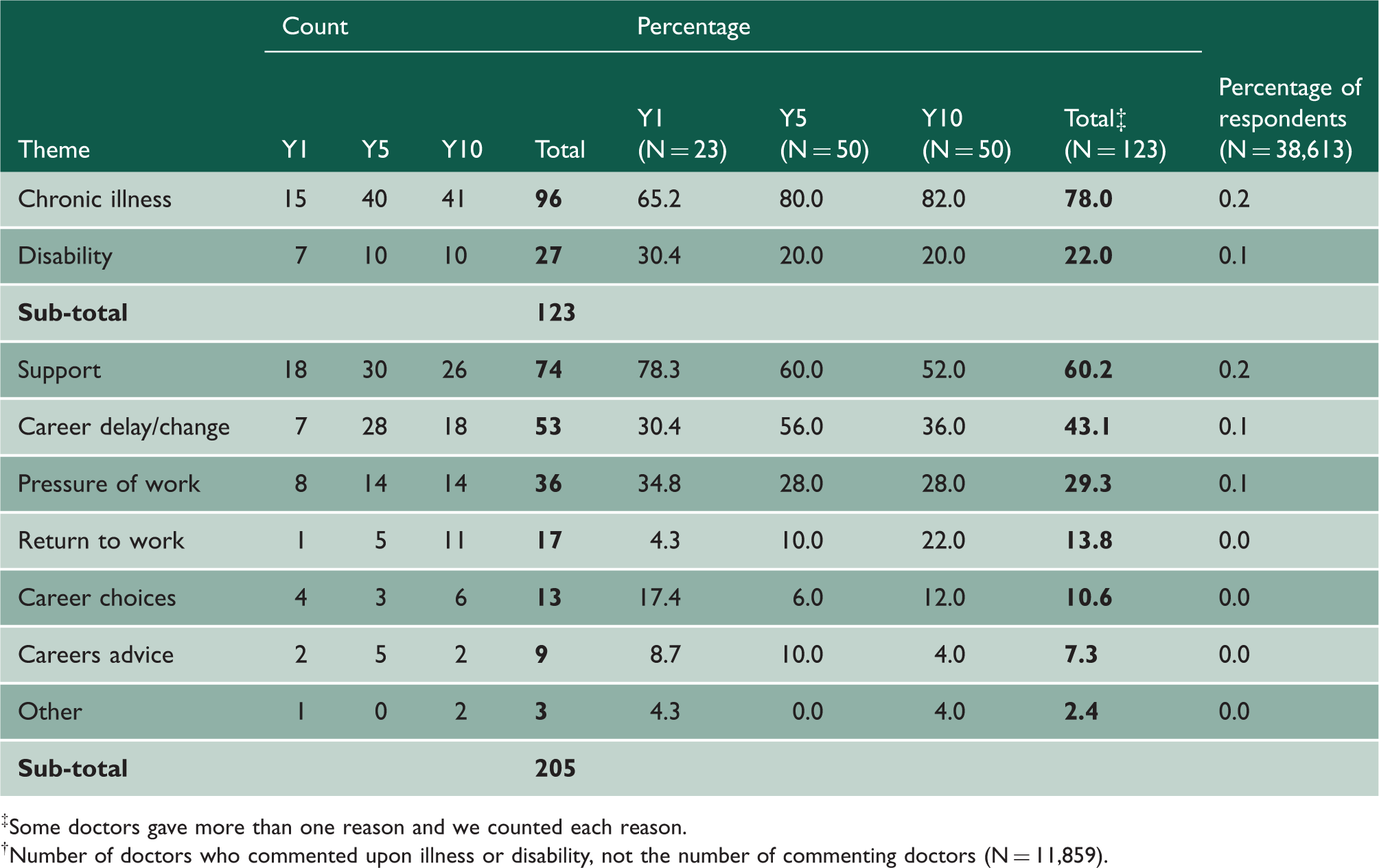
Some doctors gave more than one reason and we counted each reason.
Number of doctors who commented upon illness or disability, not the number of commenting doctors (N = 11,859).
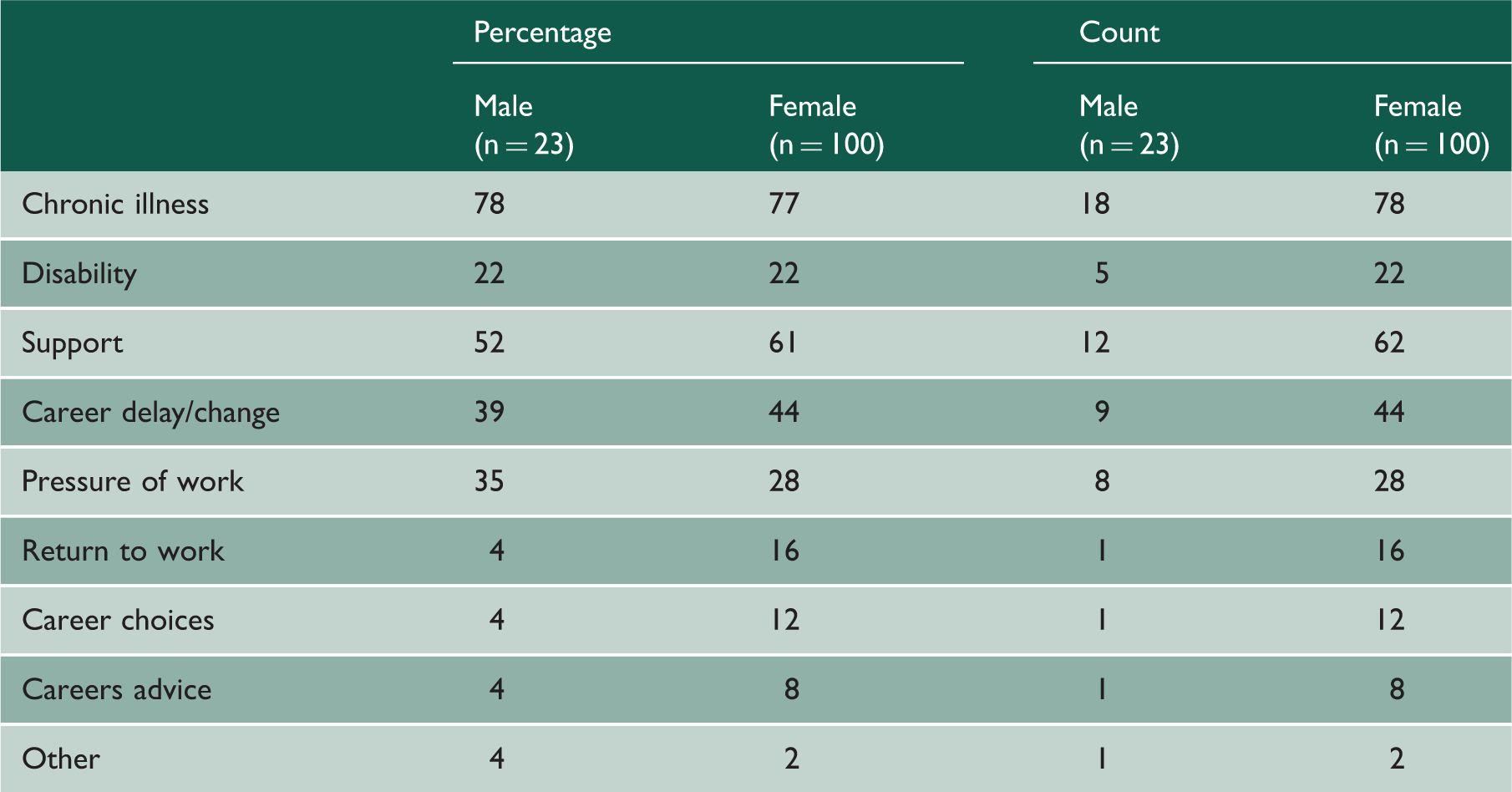
Frequency distribution of coded comments made by the doctors, by sex.
Selected quotations about working as a doctor while chronically ill or disabled.

Quote number cross-refers to ‘Results’ section.
Year denotes the number of years after graduation.
Support from others
One doctor who used a wheelchair wrote about many problems with the internal layout of hospitals (Box 1, quote 1). A senior doctor with multiple sclerosis wrote about discrimination that she had experienced across many areas of her professional life (Box 1, quote 2).
On support, it was more common for doctors to write that they had received very little support than to write that they felt well supported, whether when dealing with chronic illness, bereavement, depression, anxiety or stress (Box 1, quotes 3–6).
Doctors suffering from a chronic illness wrote that it was hard to ensure that suitable adjustments were made to their job (Box 1, quotes 5–9).
Doctors complained that guidance from the Occupational Health service within their workplace was either not forthcoming or not acted upon (Box 1, quotes 6–7). For example, one doctor with a chronic knee problem said that recommendations were not followed through (Box 1, quote 7). Another doctor could not get referred to Occupational Health for months until a worsening health condition necessitated attention (Box 1, quote 8).
Some doctors, already with health problems, struggled to cope with pressure. One doctor said that during her first year she worked a minimum 10 h a day as well as doing on-calls, despite being physically disabled (Box 1, quote 9).
Some doctors felt that they were bullied, which exacerbated their health problems (Box 1, quote 10). Another relatively senior doctor said that she had suffered depression caused by her treatment during a Senior House Officer job, which had only been alleviated by the intervention of her postgraduate dean (Box 1, quote 11).
By contrast, several doctors reported receiving a great deal of support when they were ill (Box 1, quotes 12 and 13).
Career delay/change
Several doctors wrote about changing their careers to accommodate their illness. A female general practitioner was considering palliative medicine (Box 1, quote 14). One doctor, with insulin-dependent diabetes, found that shift work made control of his blood sugars extremely difficult. He moved from hospital medicine to general practice so that he could maintain his health (Box 1, quote 15).
Other doctors wrote that they were forced to change their career because the system was too inflexible to cope with their health needs (Box 1, quote 16).
Doctors also commented that their illness had led to delays in training (Box 1, quote 17). Another doctor who was ill for a long period had serious problems achieving professional qualifications (Box 1, quote 18).
Pressure of work
Some doctors commented that pressure of work and inflexible rotas were making them feel stressed, and in some cases, mentally and physically ill (Box 1, quote 19). A few doctors reported taking time off work, reducing hours or changing careers due to stress or mental health problems (Box 1, quote 20). One doctor also commented that, for junior doctors, work in emergency medicine was particularly difficult (Box 1, quote 21).
Return to work
Some doctors who wanted to return to work after illness reported a lack of support (Box 1, quote 22) or that they faced barriers and discrimination (Box 1, quote 23).
However, a similar number of doctors had positive stories to tell about their return to work (Box 1, quotes 24 and 25).
Career choices
Doctors commented on how their illness or disability had limited their career choices. For some, the issues were specific and practical (Box 1, quote 26) while for others, they were more general (Box 1, quote 27).
Other doctors were concerned about the effect of certain career choices upon their health in the future (Box 1, quote 28).
Careers advice
Doctors at all stages of their career, from medical school through to senior level, bemoaned the lack of good career advice available to those with chronic illness or disability (Box 1, quote 29). One doctor with a disability wrote that no one had advised her about working in medicine with a disability (Box 1, quote 30).
One doctor had not been formally diagnosed with a depressive illness but had sought career advice in her last year at medical school to identify non-medical career options because she wasn’t sure she would be able to cope with a ward-based medical job (Box 1, quote 31).
Some doctors felt that career advice was limited to standard choices (Box 1, quote 32): ‘… there seems to be an ingrained “fear” or distrust of any career path outside of the norm’. A senior doctor commented similarly about the lack of alternative careers (Box 1, quote 33) and was advised to opt for general practice, but finally found a job she enjoyed after searching in the British Medical Journal special appointments pages.
Discussion
Main findings
Doctors with chronic illness or disability were most concerned about lack of support in the workplace. This included poor facilities for the disabled, experiencing insensitive working practices or colleagues, lack of offering or implementing Occupational Health guidance, bullying and discrimination. Doctors also discussed decisions to alter their career plans to fit in with their illness, but, for some, these changes felt imposed, not sought. Pressure at work was discussed as both a cause of chronic illness and as an extra stressor for doctors who were already ill. However, some chronically ill or disabled doctors commented that they had experienced very supportive and imaginative working practices from their employers, and some had found work colleagues to be adaptive and positive.
Strengths and weaknesses of the study
Our surveys were nationwide and we drew on the comments of many thousands of doctors over a number of survey years and at a range of career stages during their training and the early part of their careers. We did not specifically ask about experiences of working while chronically ill or disabled. Hence the comments we used for this study were those which arose spontaneously from the doctors, when asked to comment on any issue of importance to them about their career. Only a small number of doctors wrote about the topic, and we have no way of knowing if others have been similarly affected and have had similar experiences. The results should not be over-interpreted in that, of necessity, the findings are somewhat historical; some might pertain to situations that have now improved. If so, we hope that senior clinicians and human resources staff can assure themselves of this in respect of their own institutions.
Comparison with existing literature
A UK study of doctors who had been away from work for more than six months with physical or mental health problems reported that regulatory processes in the UK were detrimental to their mental health and did not aid their return to work. 9 Swedish research has found that doctors who took long-term sick leave were expected to take charge of their own treatment and rehabilitation. 10 Some doctors told us that, in their view, they experienced bullying behaviour and discrimination. In other studies, group interviews with trainee doctors found similar concerns regarding bullying, namely belittling, threats and unreasonable expectations. 11 A recent national survey found that disabled doctors were twice as likely as others to report bullying (15% versus 8%). 12 Research on a recent cohort of first-year doctors included the statement that ‘the NHS is a good equal opportunities employer for doctors with disabilities’: 13% disagreed, 57% agreed and the remainder had no view. 13
Implications
Doctors with chronic illness and disabilities present challenges for employers. Acceptance is needed, by doctors whose capacity for work is restricted, that there may be limits on what is possible for employers to achieve. However, our study indicates that, in the view of some affected doctors, work practices can fall short of what could reasonably be expected. There seems to be inconsistency in the level of support offered to sick or disabled doctors by employers. Sometimes poor support seemed to be due to a lack of communication and liaison between the employer’s occupational health function and its senior hospital management, or a reluctance to tailor support to the individual doctor. In other cases, the comments implied a high level of indifference on the part of management, or, occasionally, work colleagues, to the health issues of doctors.
Managers also need to be more proactive and effective at arranging the return to work of doctors who have taken long-term sick leave. There is clearly a need for good careers advice to help doctors assess which career paths to take and to mitigate the impact of delays to careers. Health organisations should have a culture of enablement whereby doctors with chronic disease or disability are supported, according to their needs, to continue their medical careers to the limit of their ability.
It was not the purpose of this study to quantify the level of chronic illness or disability among doctors. However, we note that only 1% of the commenting doctors wrote about working with a chronic illness or disability, while the Long term Conditions Compendium of Information: Third Edition published by the Department of Health in 2012 14 showed that approximately 15–25% of the general population of the approximate age of these doctors, between 25 and 35 years of age, suffered from a long-term condition. We suggest therefore that there may be a much larger volume of chronic illness and disability among doctors than that reported by us, and that formal further study of the prevalence of chronic illness and disability in doctors would be justified.
Footnotes
Declarations
Acknowledgements
We thank Janet Justice and Alison Stockford for data entry. We are very grateful to all the doctors who participated in the surveys.
Provenance
Not commissioned; peer-reviewed by Raymond Chadwick.