
Abstract
Cardiac and pulmonary artery emboli are lethal complications following vertebroplasty. Clinicians should recognise these fatal complications immediately and surgical extraction is mandatory and provides the best outcome.
Introduction
Vertebroplasty has been proven to be a safe procedure since its introduction in 1987. 1 The rate of general complications from the procedure varies between 1 and 10%. Moreover, bone cement leakage is the main complication and has been reported to be as high as 24%. 2 Cement leakage can result in lethal complications such as pulmonary and cardiac embolization. This case highlights an uncommon but a serious early complication following vertebroplasty.
Case presentation
A 28-year-old male was re-admitted to the emergency department with shortness of breath 24 h following a percutaneous uncomplicated vertebroplasty for severe osteoporosis of the lumbar spine (L2–L5). His medical history was only significant for ulcerative colitis. Initially, he had a persistent tachycardia; but otherwise haemodynamically stable. Plain chest X-ray (Figure 1(a)) showed a radiopaque mass in the right side of the heart. Transthoracic echocardiogram confirmed an unusual echogenic mass in the right atrium with a significant pericardial effusion. The patient was stable enough for a CT chest angiogram (Figure 1(b) and (c)). Suddenly, the patient deteriorated, and became hypotensive and more tachycardic (150 beats/min) with a raised JVP. A repeat transthoracic echocardiogram showed an increase in the pericardial collection with compression of the right ventricle that warranted emergency ultrasound guided pericardiocentesis that drained bloody fluid. The patient remained haemodynamically compromised with continuous drainage of dark blood. He was immediately transferred to the operating suite and emergency cardiac surgery was performed. The patient underwent a median sternotomy, standard aorto-bicaval cannulation and cardiopulmonary bypass was instituted. An 11 × 3 cm mass (Figure 2(a)) was extracted through the tricuspid valve. The ventricular rupture was directly repaired with 4-0 Prolene. The mass eroded the tricuspid valve papillary muscle which was also repaired. Another 3 × 4 cm mass (Figure 2(b)) was extracted from the right lower pulmonary artery. The patient had an uncomplicated recovery and was discharged one week later and remains well four years later.
(a) Chest x-ray showing radiopaque material protruding from the right atrium into the right ventricle (arrow); (b) Chest CT scan (axial) shows high-density cement material within the right atrium and tricuspid valve (arrow) (c) Chest CT scan (coronal view) showing radiopaque shadow in lower lobe pulmonary artery segments (arrow). (a) Extracted (11 × 3 cm) cement mass from right atrium; (b) Three extracted (3 × 4 cm) cement lumps from lower lobe pulmonary artery branches.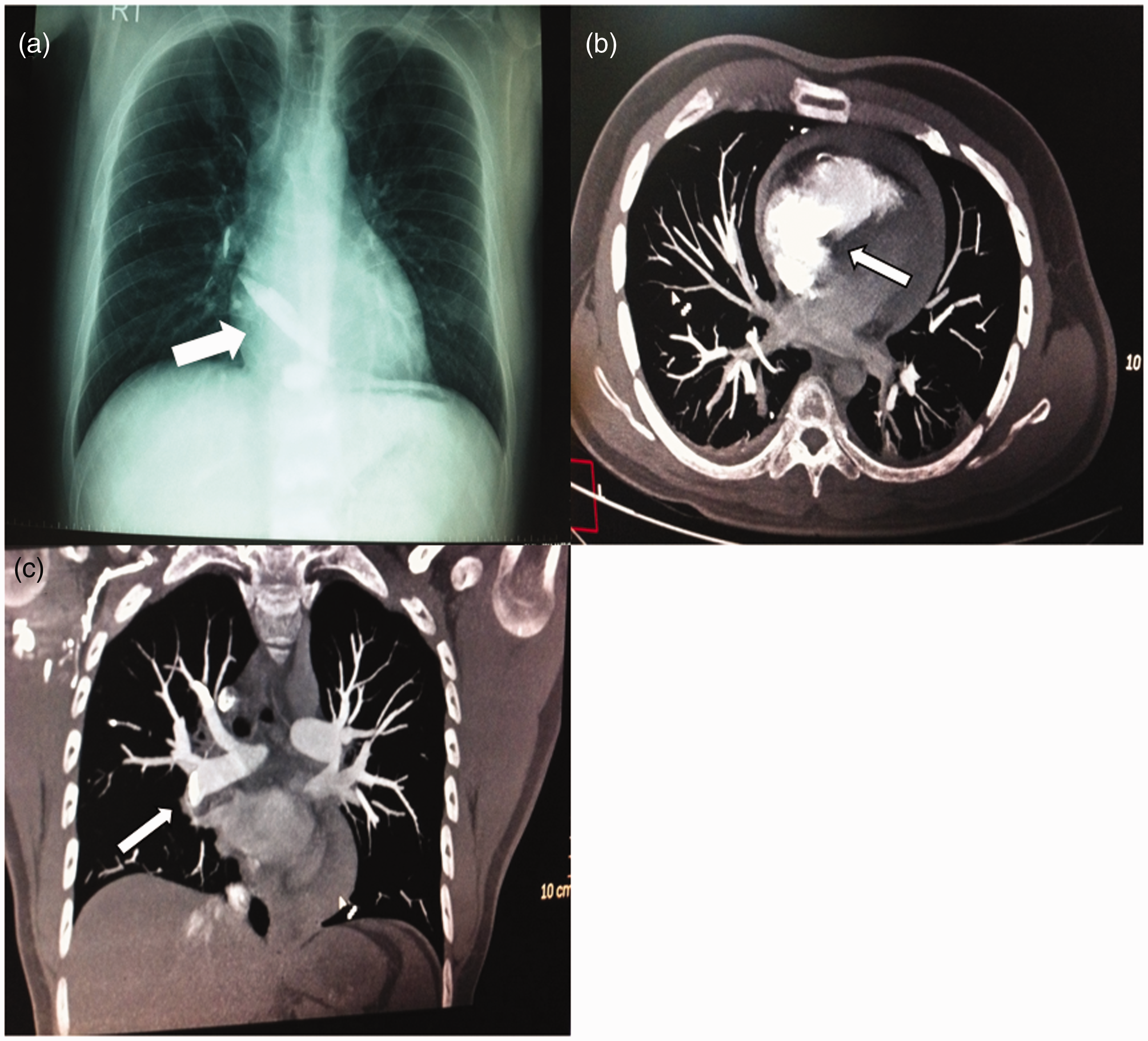

Discussion
Vertebroplasty provides better quality of life and restores vertebral body height. Nevertheless, there are complications, such as local infection, radicular pain and haemorrhage. The most lethal complications are cardiac and pulmonary artery embolization. 2 These phenomena can be explained by cement embolus migrating from the vertebral venous plexus to the inferior vena cava, right heart chambers, and pulmonary arterial system. Pulmonary cement emboli after vertebroplasty are not uncommon (1%–23%). 2 Most cases are asymptomatic, with only 1% presenting with dyspnoea which usually settles with conservative management (oxygen therapy ± anticoagulants and observation). 3 However, for symptomatic cases or patients with central emboli, anticoagulation cannot dissolve the cement or release the right ventricular load, and surgical extraction is mandatory. We emphasize on the immediate arrangements for the institution of cardiopulmonary bypass and surgical extraction of the cement emboli when a significant pericardial collection is noted specially after continuous blood oozing after pericardiocentesis.
This is the first case reporting cardiac cement embolus larger than 10 cm and presenting less than 24 h following the vertebroplasty procedure. Previous reports of similar cement-related cardiac perforation and pulmonary emboli involved smaller fragments (range, 1–10 cm).2,4–7 Only one article reports a patient with acute respiratory distress during the vertebroplasty procedure requiring emergency surgery for a PA embolus. 8
We recommend using large calibre needles, with a side-opening cannula, to reduce the injection pressure. 9 Real-time CT guidance during vertebroplasty has proven to be superior to conventional fluoroscopy guidance. 10 Finally, we suggest that all symptomatic patients with a history of vertebroplasty should have a CT chest and echocardiography performed and managed accordingly.
Footnotes
Declarations
Acknowledgements
None
Provenance
Not commissioned; peer-reviewed by Sandeep Basavarajaiah