
Abstract
Objective
To analyse the prevalence of malnutrition among paediatric patients at the time of hospital admission throughout a calendar year in a tertiary-level hospital and to identify those patients and/or groups of pathologies with a higher risk of malnutrition.
Design
Observational (retrospective evaluation of nutrition status).
Setting
Navarra Hospital Complex, Pamplona, Spain.
Participants
A total of 852 patients hospitalised in 2013 in a Spanish tertiary-level paediatric hospital (462 males and 390 females).
Main outcome measures
Sex, age, body mass index at the moment of admission and days of hospitalisation and diagnosis codified according to the International Classification of Diseases were registered.
Results
The prevalence of malnutrition patients registered at the moment of admission was 8.2%. Diseases of the nervous system (22.9%), together with diseases of the respiratory system (22.9%), infectious diseases (18.6%), congenital malformations (11.4%) and diseases of the genitourinary system (8.6%) account for 84.4% of the cases with malnutrition.
Conclusions
The overall prevalence rate for malnutrition in paediatric patients at the moment of admission in our hospital was 8.2%, being a figure similar to those published in occidental countries. It should be mandatory to accomplish an initial screening and follow-up during hospitalisation of younger patients and those suffering from diseases of the nervous and/or respiratory system and, especially, from congenital diseases.
Keywords
Introduction
The nutritional deterioration in hospitalised adult patients has been a subject of extensive analysis, being associated with higher morbidity and mortality and, therefore, an increase in healthcare expenditure.1–4 This eventuality has been widely debated at the highest administrative and political level, so making necessary the development of clinical guides and resolutions (from the Council of Europe) on feeding and nutritional care in hospitals.5–8
The epidemiological studies on hospital malnutrition that have been carried out in occidental countries show a prevalence of malnutrition at the time of admission ranging from 6.1 to 13.3%,9–15 making these patients more susceptible to presenting nutritional deterioration during the hospital stay.15–17 However, this eventuality often goes undetected owing to the lack of specific strategies for nutritional screening. 18
Several nutrition screening tools have been designed to identify patients at risk of malnutrition, which have been validated and adapted to paediatric age. They basically consist of scoring systems that allow the identification of patients at risk of malnutrition (and, therefore, in need of a deeper clinical and nutritional evaluation), from clinical and anthropometric data. We should mention the Pediatric Nutritional Risk Score, as well as the Screening Tool for Risk on Nutritional Status and Growth and the Screening Tool for the Assessment of Malnutrition in Pediatric, even though there is no clear consensus on the most appropriate nutrition screening tool to be applied in paediatric age.19–23
Nevertheless, there are several diseases that are an explanation per se for this nutritional situation, which suggests that the nutritional status at the moment of admission could be conditioned by the suffering of an specific pathology,11–24 and, consequently, it could be useful to get to know the group of diseases that involves a higher risk of hospital malnutrition in order to take preventive measures.
The purpose of this work is to analyse the prevalence of malnutrition of the paediatric patients at the time of hospital admission throughout a calendar year in a tertiary-level hospital and to identify those patients and/or groups of pathologies with a higher risk of malnutrition.
Material and methods
The Spanish Community of Navarre (Comunidad Foral de Navarra) had a population of 644,477 inhabitants in 1 January 2013 (according to the Instituto de Estadística de Navarra), with a child population (under 15 years of age) of 100,424 (15.6%). The structural and/or functional organization of the Health Care system (Sistema Navarro de Salud) allows every patient whose clinical status requires assistance to be referred from secondary level hospitals (located in the cities of Tudela and Estella) to the reference hospital in our community (Complejo Hospitalario de Navarra).
A retrospective evaluation of nutrition status at the moment of admission (from every patient who required admission in the paediatric department of our hospital within the period 1 January–31 December 2013) has been carried out. Neonates (aged less than one month), oncology, paediatric intensive care unit and surgery patients were excluded.
Sex, age, weight and height at the moment of admission were recorded. In the same way, hospital stay (days of hospitalisation) and diagnosis (codified according to the last edition of the International Statistical Classification of Diseases and Related Health Problems 10th revision, ICD-10) were also registered. 25
Inpatients were divided into age groups: infants (1 to 12 months), preschool children (1 to 6 years), school children (6 to 10 years) and adolescents (10 to 15 years).
Weight and height evaluations were assessed wearing underwear and barefoot. Weight was measured using an Año-Sayol scale, which has a 0 to 120 kg range and a precision of 100 g, and height was measured with a Holtain wall stadiometer, ranging 60 to 210 cm and a precision of 0.1 cm.
The criterion to define the nutritional status of the patients was the body mass index, according to the formula: weight (kg)/height2 (m). The Z-score values for the body mass index were calculated using the program Aplicación Nutricional, from the Spanish Society of paediatric gastroenterology, hepatology and nutrition (Sociedad Española de Gastroenterología, Hepatología y Nutrición Pediátrica); the reference growth charts were those from Ferrández et al. (Centro Andrea Prader, Zaragoza 2002). 26
The Z-score value for body mass index allowed establishing the following groups:
Malnutrition: when Z-score was lower than −2.0 (third percentile). Normality: Z-score between −2.0 (third percentile) and + 1.0 (85th percentile). Overweight: Z-score higher than 1.0 (85th percentile). Obesity: Z-score higher than 2.0 (97th percentile).
Results are displayed as percentages (%), means (M) with corresponding standard deviations (SD) and/or 95% confidence intervals. The statistical analysis (descriptive statistics, Student’s t test, ANOVA test and comparison of percentages) was done using the Statistical Packages for the Social Sciences (SPSS) version 20.0 program (Chicago, Illinois, USA). Statistical significance was assumed when p was lower than 0.05.
Results
The number of inpatients in the year 2013 was 852: 462 males (54.2%) and 390 females (45.8%). The measurement of anthropometric variables (weight and height) and the calculation of body mass index were carried out in 814 patients (95.8% of the admissions). The distribution of patients according to age group was 262 infants (30.8%), 382 preschool children (44.8%), 94 school children (24.4%) and 114 adolescents (13.4%). The seasonal distribution was 282 patients (33.1%) in winter, 106 (24.2%) in spring, 184 (21.5%) in summer and, finally, 180 (21.1%) in autumn.
The average stay was 3.87 days (CI 95%: 3.61–4.09), with no statistically significant differences among age groups. Hospital stay ranged 2 to 5 days in 82.4% of cases (n = 702), 6 to 10 days in 12.2% of cases (n = 104), 11 to 30 days in 4.8% (n = 41) and, finally, longer than 30 days in only five patients (0.6%). There were no statistically significant differences in hospital stay in relation to the nutritional status of the patients at the moment of admission and/or the group of diseases of the ICD-10.
Groups of diseases (ICD-10) according to age groups.
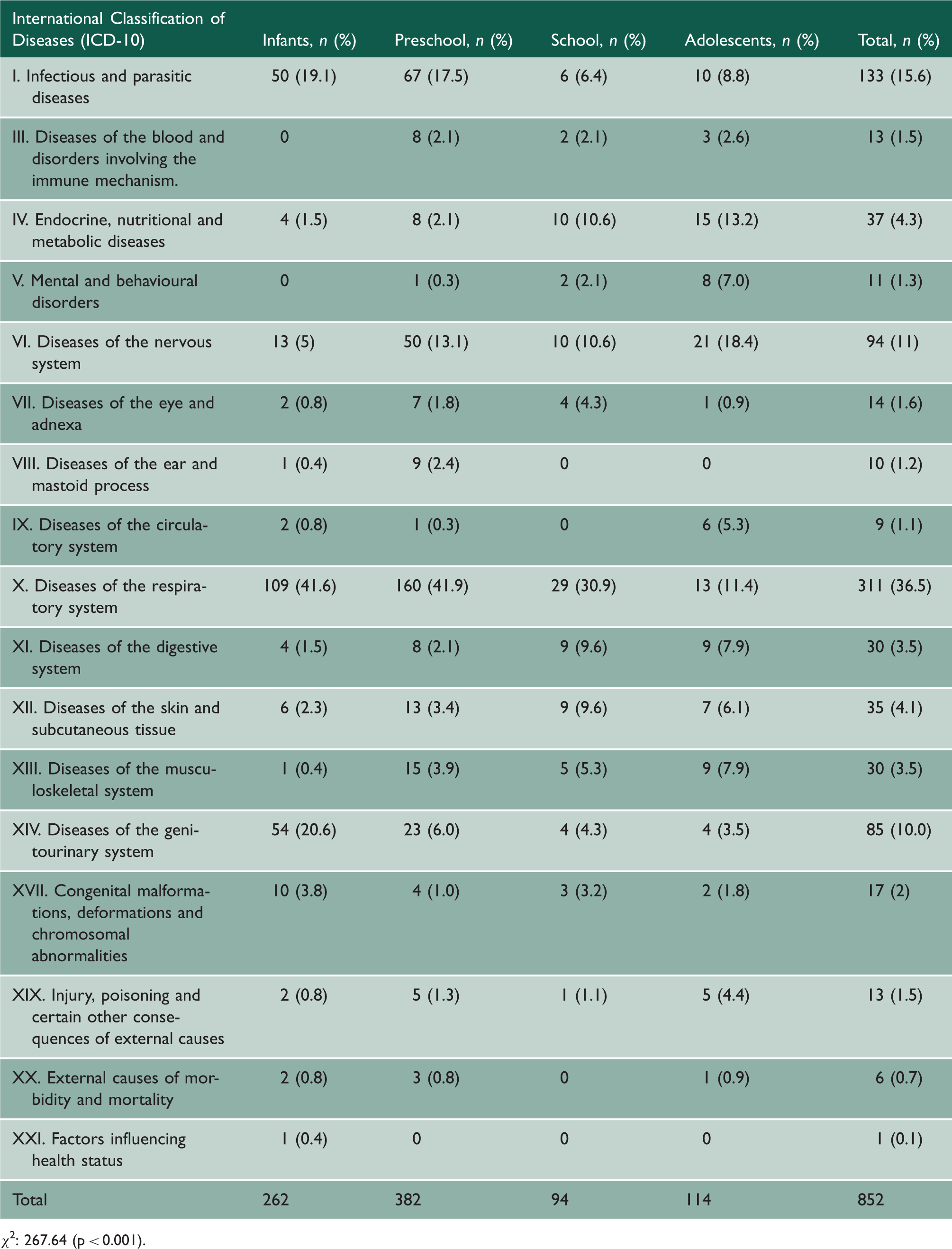
χ2: 267.64 (p < 0.001).
Nutritional status of the patients at the moment of admission according to age groups.

Chi2: 27.893 (p < 0.006).
Nutritional status of the patients according to group of diseases (ICD-10).

Chi2:108.866 (p < 0.001).
Diagnosis after hospital admission in patients with malnutrition (n = 70) according to age groups.

Discussion
The objective of this study was to determine the nutritional status of the patients right at the moment of admission in a tertiary care paediatric hospital during a natural year (January to December) and its relation with the medical diagnosis; the anthropometric measurements were the screening tools to be applied in order to identify those patients with malnutrition and, therefore, at a higher risk of nutritional deterioration during hospital stay. Moreover, in order to solve potential arbitrariness in the gathering of patients according to the different diseases, they were classified following the most recent edition of the International Classification of Diseases from the WHO. The exclusion of neonates, as well as patients from paediatric oncology, paediatric intensive care and paediatric surgery was due to the need, in most cases, of nutritional support in relation to the diagnosis and/or treatment. In our case, the interest relies on the analysis of the nutritional situation in those patients who were not to be monitored regarding nutrition during the hospital stay.
There are few references in our country on nutritional status in paediatric patients who require hospital admission, and the published data are somehow incomplete.13,27 As an example, the DHOSPE (Desnutrición Hospitalaria en el Paciente Pediátrico en España) study, even when it is an ambitious multicentric study, only registers patients in summer months (June to September) and, as occurred in our study, the diseases of the respiratory system, which are the most frequent causes for admission, have a higher prevalence in autumn and winter months. In addition, the diseases of the respiratory system account for a significant percentage of patients with malnutrition.
The European Charter on the rights of children in hospital (from the Association for Children in Hospital – EACH), promulgated by the European Parliament and whose content was assumed and promoted by the UNICEF and the WHO, begins with the statement that “children shall be admitted to hospital only if the care they require cannot be equally well provided at home on a day basis”. The policy for paediatric hospital admission in our environment, pursuant to this resolution, is quite restrictive, intending that only those patients whose pathology requires exclusive hospital care be admitted. This clarification was obliged in order to understand the fact that 82.4% of inpatients throughout the year 2013 went through a hospital stay no longer than five days and that 5.4% overtook a 10-day hospitalisation, extended stays being exceptional. In addition, these restrictive measures – always intended to be applied with common sense – would also explain the absence of statistical relationship between nutritional status at the moment of admission and the days of hospitalisation, regardless of age and group of disease.
The overall prevalence rate for malnutrition in paediatric patients at the moment of admission in our hospital was 8.2%, this figure being similar to those published in occidental countries8–15 and, of course, much lower than those countries with worse socioeconomic conditions.17,28,29 Nevertheless, it is important to highlight two variables that seem to play an important role in detecting patients at risk of malnutrition at admission: age and reason for admission. The results obtained in this study indicate that, on one side, 85.7% of the cases with malnutrition recorded were infants and/or preschool children; and, on the other side, that the diseases of the nervous and/or respiratory system account for almost half of the cases of malnutrition. Additionally, the congenital malformations, deformations and chromosomal abnormalities, even though with a low prevalence, involve a high risk of malnutrition. It is well worth remembering that one out of six admissions secondary to diseases of the digestive system also present with malnutrition at admission.
Conclusion
As a conclusion, it should be mandatory to accomplish an initial screening and follow up during hospitalisation – probably by applying validated nutrition screening tools18–22 – of younger patients and those suffering from diseases of the nervous and/or respiratory system and, especially, from congenital diseases, given the risk of presenting with malnutrition at the moment of admission and the potential deterioration during the hospital stay. Nevertheless, this strategy should be applied to every patient. This means, we should establish, on a routine basis, simple strategies to detect those patients at nutritional risk at the moment of admission, either by age or by the disease they suffer from, and also establish immediately all necessary measures of nutritional support in order to assist in the prevention and, when applicable, resolution, of an adverse nutritional situation.