
Abstract
Objective
To analyze the seasonal variations in calcidiol and parathyroid hormone serum levels along a natural year in a paediatric population living in a region of the north of Spain considering a normal nutrition status.
Design
A cross-sectional study.
Setting
Navarra Hospital Complex, Pamplona, Spain.
Participants
A total of 413 Caucasian individuals (aged 3.1 to 15.4 years): 227 school children (96 males and 131 females) and 186 adolescents (94 males and 92 females), with normal nutritional status.
Main outcome measures
Clinical examination (sex, age, weight, height and body mass index) and blood testing (calcium, phosphate, alkaline phosphatase, calcidiol and parathyroid hormone) during the year 2014.
Results
Calcidiol levels were lower during spring (25.96 ± 6.64 ng/mL) and reached its maximum level in summer (35.33 ± 7.51 ng/mL); parathyroid hormone levels were lower in summer (27.13 ± 7.89 pg/mL) and reached maximum level in autumn (34.73 ± 15.38 pg/mL). Hypovitaminosis D prevalence was 14.3% in summer and 75.3% in spring. Parathyroid hormone levels were compatible with secondary hyperparathyroidism in eight individuals (1.9%). There is a correlation (p < 0.01) between calcidiol and parathyroid hormone (r = −0.336). Logistic regression showed significant increased risk of hypovitaminosis in females (OR:1.63) and adolescents (OR:1.77), and when blood samples taken in autumn (OR:12.22), winter (OR:8.54) and spring (OR:19.72).
Conclusions
There is a high prevalence of hypovitaminosis D in the paediatric population with a healthy nutrition situation in Navarre, mainly during the months of autumn and winter, and, especially, in spring time. Given the difficulties in maintaining a sufficient amount of body vitamin D content along the year, it should be considered to give vitamin supplements and/or increase the intake of its natural dietary sources or vitamin D fortified foods.
Introduction
Vitamin D (cholecalciferol) is a prohormone that is basically synthesized in the skin under the influence of solar radiation. It requires a double hepatic (25-OH-D: calcidiol) and renal (1, 25-(OH)2-D:calcitriol) hydroxylation in order to get its functional activation. The exposure to ultraviolet radiation (type B) leads to endogenous synthesis of vitamin D from epidermal 7-dehydrocholesterol, this being the main source of vitamin D, while less than 10% comes from natural dietary sources.1–3 In the northern hemisphere, beyond 37th parallel (north) and, especially during the colder months of the year, the axial tilt (obliquity) of our planet and the consequent changes in density of incident rays cause ultraviolet radiation (type B) to be diminished by about 80–100%. Thus, the solar radiation is unable to induce an effective vitamin D synthesis and this could explain the seasonal variations in vitamin D content in our bodies.4–7 Therefore, the causes of vitamin D deficiency are usually related either to physical agents that block the exposure to solar radiation (cutaneous pigmentation, sun filters, etc.), or to geographical variables, such as sunlight exposure, atmospheric pollution and altitude, as well as latitude and season of the year.2,3
Serum levels of calcidiol constitute the best indicator of vitamin D reserve in our body, even though there is some controversy about the limits that define its normality.1,8–10 Vitamin D deficiency implies a lower absorption of dietary calcium, so increasing parathyroid hormone secretion in order to maintain normal levels of serum calcium, and, ultimately, induces osteoclastic activity and, consequently, a higher risk of losing bone mineral density. 1 In addition to its contribution to bone metabolism, vitamin D fulfils a broad spectrum of biological functions related to cell proliferation, differentiation and metabolism, which justifies the interest in monitoring its body content.4,11 Nevertheless, the combined intervention of vitamin D and parathyroid hormone, at least regarding the homeostasis of calcium and phosphorus metabolism, may lead to considering that the changes in vitamin D concentrations through the year could be followed by seasonal changes in parathyroid hormone levels.
The aim of this work is to analyze the seasonal variations in calcidiol and parathyroid hormone serum levels during a natural year in a paediatric population living in a region of the north of Spain with a normal nutrition status.
Material and methods
Patients
This is a cross-sectional study of 413 individuals (190 males and 223 females) aged 3.1 to 15.4 years who underwent a clinical examination and blood testing in the Pediatric Endocrinology Unit in the period January–December 2014. The patients were divided into two different groups according to age: school group (age 3.1 to 10.0 years) made up of 227 individuals (96 males and 131 females), and adolescent group (age 10.01 to 15.4 years) made up of 186 individuals (94 males and 92 females).
The individuals were healthy Caucasian children born from Caucasian parents of Spanish origin living in the Spanish community of Navarra. All patients that had received vitamin D supplements in the previous 12 months or suffered from chronic pathologies that might affect growth, body composition, food ingestion or physical activity were excluded. In the same way, the condition sine qua non to be included in this study was having a normal nutrition status at the moment of the beginning of the study, meaning, body mass index should fluctuate between −2.0 (3rd percentile) and +1.0 (85th percentile) standard deviations.
Clinical examination
Weight and height measurements were made in underclothes and barefoot. Weight was measured using an Año-Sayol scale (reading interval 0 to 120 kg and a precision of 100 g), and height was measured using a Holtain wall stadiometer (reading interval 60 to 210 cm, precision 0.1 cm). Body mass index was calculated with the following formula: weight (kilograms)/height 2 (meters). The standard deviation score for body mass index was calculated using the program Aplicación Nutricional from the Spanish Society of Pediatric Gastroenterology, Hepatology and Nutrition (Sociedad Española de Gastroenterología, Hepatología y Nutrición Pediátrica, available at http://www.gastroinf.es/nutritional/). The graphics from Ferrández et al. (Centro Andrea Prader, Zaragoza 2002) were used as reference charts.
Blood testing
Calcium, phosphorous and alkaline phosphatase plasma levels were determined in basal conditions (fasting) by standardized methodologies. Calcidiol was measured by radioimmunoassay and parathyroid hormone by chemilumenescence. Different situations were defined according to calcidiol levels: (a) Vitamin D deficiency when levels are lower than 20 ng/mL (<50 nmol/L), (b) Vitamin D insufficiency when levels fluctuate between 20 and 29 ng/mL (50–75 nmol/L) and (c) Vitamin D sufficiency when levels reach or overtake 30 ng/mL (>75 nmol/L). Secondary hyperparathyroidism was defined when parathyroid hormone serum levels overtake 65 pg/mL.
Statistical analysis
Results are displayed as percentages (%) and means (M) with corresponding standard deviations or confidence intervals (95% CI). The statistical analysis (descriptive statistics, Student’s t, ANOVA, χ2 test, Pearson correlation and logistic regression) was performed using the program Statistical Packages for the Social Sciences version 20.0 (Chicago, IL, USA). Statistical significance was assumed when p was lower than 0.05.
Parents and/or legal guardians were informed and provided verbal consent for the participation in this study in all cases. The study was approved by the Ethics Committee for Human Investigation at our institution.
Results
The average values for calcidiol and parathyroid hormone plasma levels from the totality of the collections were 28 ± 7.6 ng/mL and 30.58 + 15.48 pg/mL, respectively. Calcidiol levels overtake 30 ng/mL (Vitamin D sufficiency) in 174 individuals (42.4%), oscillate between 20 and 29 ng/mL (Vitamin D insufficiency) in 184 (44.9%) and are lower than 20 ng/mL (Vitamin D deficiency) in 52 (12.7%). A further individual was found suffering from severe calcidiol deficiency (<10 ng/mL) the sample having been obtained from an adolescent in the month of November. In the same way, parathyroid hormone levels overtake 65 pg/mL (hyperparathyroidism) in eight cases (1.9%). No values for hypo/hypercalcemia of hypo/hyperphosphatemia were detected.
Clinical and biochemical characteristics in children and adolescents (mean ± SD).
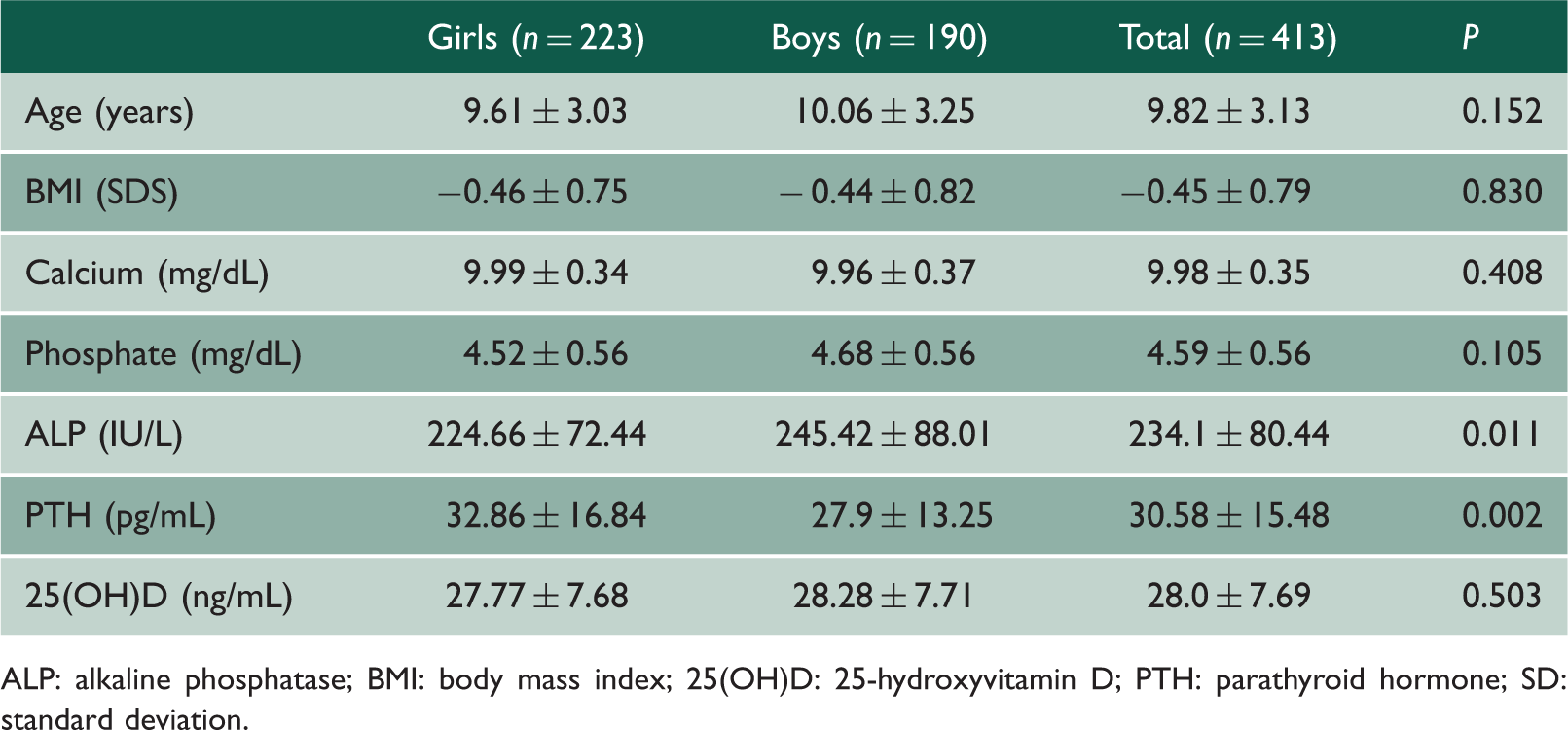
ALP: alkaline phosphatase; BMI: body mass index; 25(OH)D: 25-hydroxyvitamin D; PTH: parathyroid hormone; SD: standard deviation.
Clinical and biochemical characteristics in children and adolescents (mean ± SD).

ALP: alkaline phosphatase; BMI: body mass index; 25(OH)D: 25-hydroxyvitamin D; PTH: parathyroid hormone; SD: standard deviation.
Biochemical characteristics according to seasons (mean ± SD).

ALP: alkaline phosphatase; 25(OH)D: 25-hydroxyvitamin D; PTH: parathyroid hormone; SD: standard deviation.
The prevalence of hypovitaminosis D according to seasons.
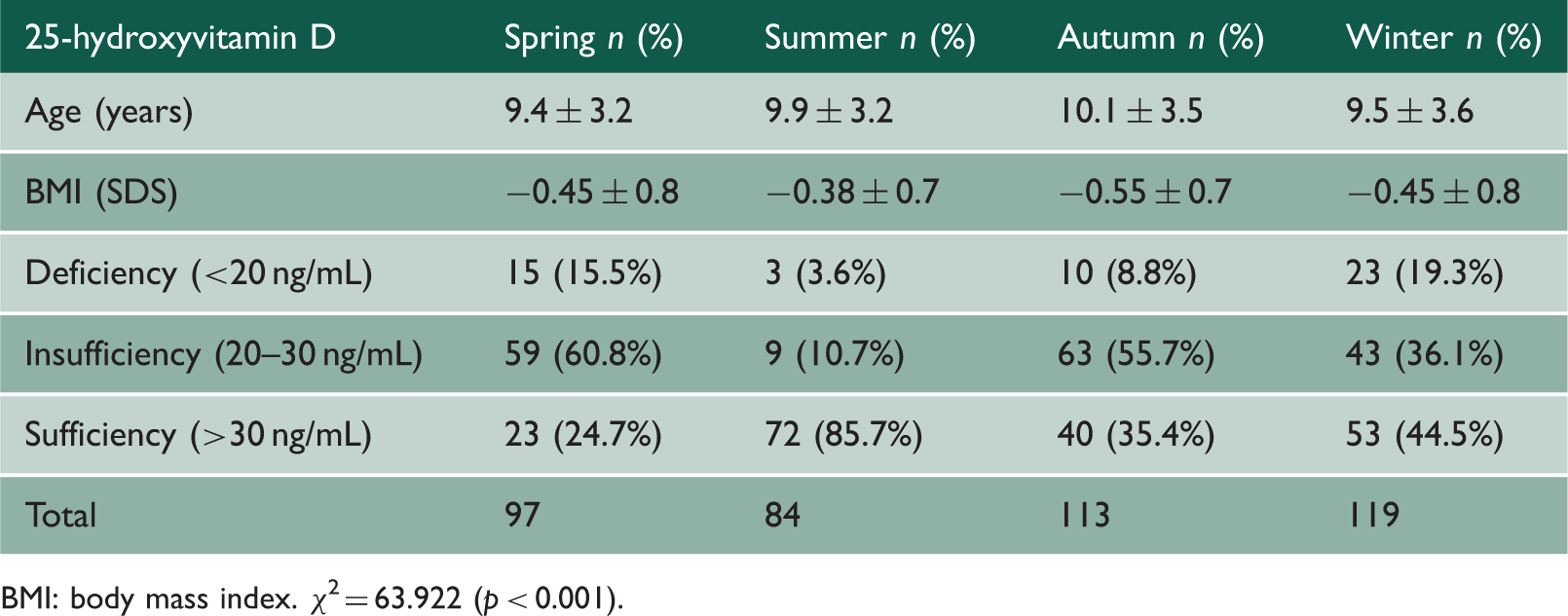
BMI: body mass index. χ2 = 63.922 (p < 0.001).
Figure 1 states the average values for calcidiol levels across the months of the year (ANOVA, p < 0.001), showing the highest levels during the summer months (July: 34.3 ng/mL, CI 95%: 30.4–38.3; August: 37.5 ng/mL, CI 95%: 40.9–34.2 and September: 33.3 ng/mL, CI 95%: 37.0–29.6); meanwhile, these levels were lower during the spring months (April: 24.8 ng/mL, CI 95%: 27.5–22.2; May: 26.1 ng/mL, CI 95%: 28.8–23.5 and June: 26.5 ng/mL, CI 95%: 29.0–24.2).
Calcidiol levels across the months of the year (ANOVA, p < 0.001).
Figure 2 displays the average values of parathyroid hormone levels across the months of the year (ANOVA, p < 0.001), observing the highest levels during the autumn months (October: 34.3 pg/mL, CI 95%: 29.2–39.5; November: 34.0 pg/mL, CI 95%: 30.8–37.2 and December: 33.5, CI 95%: 28.5–38.5) and the end of spring (May: 30.2 pg/mL, CI 95%: 25.4–35.1 and June: 31.4 pg/mL, CI 95%: 26.0–36.9); meanwhile these levels were lower in the summer months (July: 25.5 pg/mL, CI 95%: 21.6–29.7 and August: 26.6 pg/mL, CI 95%: 22.4–30.9).
PTH levels along the months of the year (ANOVA, p < 0.001).
There was a statistically significant correlation (p < 0.01) between calcidiol and parathyroid hormone levels (r = 0.336), also between calcium and parathyroid hormone plasma levels (r = −0.236); in addition, there was also correlation between age and calcidiol levels (r = −0.204) and between age and calcidiol (r = −0.006) and parathyroid hormone (r = 0.049).
Females and the adolescent group showed a higher risk of hypovitaminosis D with respect to males (OR: 1.625, CI 95%: 1.05–2.49) and the school children group (OR: 1.771, CI 95%: 1.13–2.75), respectively. In addition, the risk of suffering from hypovitaminosis D was significantly higher in autumn (OR: 12.22, CI 95%: 5.23–28.5), winter (OR: 8.54, CI 95%: 3.66–19.9) and spring (OR: 19.72, CI 95%: 7.9–49.22) with respect to summer.
Discussion
This work constitutes the first study on the combined variations of calcidiol and parathyroid hormone during a natural year in a Spanish paediatric population with a normal nutrition status. The criteria from the American Academy of Endocrinologists have been applied in order to compare the results to the previous published data; these criteria consider calcidiol as the best indicator of body vitamin D content, given its long half-life (two to three weeks) and, in the same way, establish normality when serum levels reach 30 ng/mL and hypovitaminosis D below this point; in this situation, we refer to vitamin D insufficiency (between 21 and 29 ng/mL) and deficiency (lower than 20 ng/mL).1,9
The results obtained suggest that age and sex are not determining variables of body vitamin D content, even though there was a higher risk for suffering from hypovitaminosis D in women and adolescents, as other authors have published before;5–8,12–16 instead, this content would depend basically on geographical location and/or weather conditions corresponding to the population we want to analyze. Among November and February, in higher latitudes, the solar zenith angle is so oblique that few ultraviolet B photons reach the surface of the earth. 4 Navarre is a Spanish region located between 41°55″22 N (Cortes) and 43°16″42 N (Bera de Bidasoa); as a main weather characteristic, it is remarkable that, in 2014, rainfall was recorded in 47.6% and 31.8% of the days of the corresponding colder (autumn and winter) and warmer months (spring and summer), respectively. This means, in addition to be a high-latitude area, it has a frequency of cloudy/rainy days that is important enough to consider that cyclical variation in calcidiol levels along the year could be explained by a presumably inefficient vitamin synthesis in skin induced by sun radiation, as several authors have noted.5–8,12,14,16,17 In fact, the results confirm that body vitamin D content during the summer months was sufficient in 85.2% of the population analyzed, it slightly decreases in autumn and winter (the percentage of hypovitaminosis D gets to 64.3% and 55.8% in autumn and winter, respectively) and falls to its lowest point in spring, when prevalence of hypovitaminosis was 75.3%.
The analysis of the blood collections performed reveals a prevalence of levels of vitamin D considered as sufficient in 42.4% of the selected population, whereas the remaining 44.9% and 12.7% showed insufficiency of deficiency in vitamin D, respectively. These results, even when considered as high rates of hypovitaminosis for a healthy population, are relatively moderate rates with respect to other published studies;6,7,13,15,18–22 this may be due to the exclusion of overweight/obese patients and the origin/race of such patients (Caucasian), since, as is well known, the difference in skin pigmentation in different ethnic groups implies a higher risk of hypovitaminosis D.
The negative correlation between calcidiol and parathyroid hormone plasma levels has been previously described by different authors;4–8,12,15 however, the combined oscillations existing among both hormones through a natural year have been much less discussed.23,24 This work reveals how asynchronous changes in parathyroid hormone levels with respect to calcidiol take place simultaneously with monthly and/or seasonal variations in calcidiol levels, a fact that presumably would allow maintaining constant calcium levels along the year, as we observe in this study. In fact, the highest body vitamin D content corresponds to summer months – greater sunlight exposure – decreases gradually during autumn and winter months – except for some biological variability – and gets to its highest point in springtime. In contrast to the findings of other authors,5,6,25 only 8 (3.4%) out of 236 individuals in a situation of vitamin D insufficiency of deficiency showed parathyroid hormone levels within range of hyperparathyroidism; since there was neither any diagnosis of hypercalcemia or hypocalcemia nor any bone semiology associated, we could consider that the seasonal variations of calcidiol and parathyroid hormone levels would correspond to a physiological phenomenon of adaptation to the weather and geographical conditions that characterize this region.
Because geographical conditions affect significantly the body vitamin D content and, consequently, parathyroid hormone plasma levels, it would be extremely risky to make comparisons among the different results obtained in the published works from different countries and/or weather conditions, since latitude, and especially the month of the year when the blood sample was collected, have to be always considered. This means, we cannot refer to a vitamin D status in a determined population without mentioning the seasonal variations because, as happened in this case, the risk of suffering from hypovitaminosis D was related to the season of the year in which the sample was collected.
Most body cells and organs (muscle, heart, blood vessels, brain, mammary gland, colon, prostate, gonads, skin, B and T lymphocytes, etc.) have vitamin D receptors and activating enzymes for calcitriol synthesis that, in these locations, is not regulated by parathyroid hormone. This fact suggests the biological importance of sufficient calcidiol serum levels.2,11 In this sense, calcidiol chronic deficiency has been related to a higher cardiovascular risk, as well as a risk to present autoimmune, endocrine, infectious, psychiatric and/or neurological diseases and several types of cancer.1,2,26,27 Therefore, and due to the difficulty in maintaining a sufficient body vitamin D content in the paediatric age group throughout the year, there is a need to supplement with vitamin D (600 UI/day) and/or increase the ingestion of higher amounts from its natural dietary sources (herring, salmon, sardines, tuna, etc.) or vitamin D fortified foods (dairy products, cereals, etc.) during the months of winter and spring, as several authors have suggested.1,5–7
This work has several limitations. As an example, some variables have not been analyzed and they could, to some extent, condition the body vitamin D content, such as the hours of sun exposure, the use of sun screens or calcium and vitamin D dietary intake. However, the monthly and/or seasonal variations in calcidiol and parathyroid hormone are so explicit to leave little doubt about its direct relation to weather and geographical conditions.
Conclusion
As a conclusion, there is a high prevalence of hypovitaminosis D in the paediatric population with a healthy nutrition situation in Navarre, mainly during the months of autumn and winter, and, especially, in spring time. Given the difficulties in maintaining a sufficient amount of body vitamin D content throughout the year, giving vitamin supplements and/or increasing the intake of its natural dietary sources or vitamin D fortified foods should be considered.
Footnotes
Declarations
Acknowledgements
None
Provenance
Not commissioned; peer-reviewed by Eugen-Matthias Strehle