
Abstract
Lesson
Primary polydipsia occurs in up to 25% of patients with chronic psychiatric disorders (especially schizophrenia), related to the disease, its treatment or both. Urine output fails to match intake >10 L/day and water intoxication may develop. Rhabdomyolysis is a rare complication of hyponatremia, and an acute anterior compartment syndrome of the leg, an emergency, may be very rarely associated.
Case report
A 58-year-old man had a six-year history of hypertension and dyslipidemia controlled with lercanidipine and atorvastatin (10 mg/day, each). He had been diagnosed with paranoid schizophrenia at the age of 25 and was living in a hostel and treated with zuclopenthixol (200 mg intramuscular, every two weeks) and olanzapin (15 mg/day). Five years prior he was admitted with generalized convulsions due to severe hyponatremia and his recovery was complicated by rhabdomyolysis. There was no history of alcohol or drug abuse and no other admissions. His drug treatment had been unchanged for years.
He was now admitted when, following excessive water drinking, he became confused and agitated over a day, with no convulsions. The general/neurologic examination was non-contributory. Tests revealed serum sodium of 110 mEq/L (urinary sodium 10 mEq/L) with normal renal, adrenal and thyroid function (estimated glomerular filtration rate 105 ml/min, MDRD formula) and elevated creatine kinase of 748, then 8000 IU/L (normal <200). Serum aspartate aminotransferase and lactate dehydrogenase were also increased and the patient's urine was noted to be dark brown and tested strongly positive for myoglobin. Serum osmolality was 236 mosm/Kg (normal 275–290 mosm/Kg) with urinary osmolality 72 mosm/Kg. Other laboratory tests including serum potassium, phosphate, calcium and liver enzymes were unremarkable. Head CT showed cerebral edema. Self-induced water intoxication with severe symptomatic hyponatremia and associated rhabdomyolysis were diagnosed. He was treated with hypertonic saline and serum sodium rose to 128 mEq/L (at 24 h), then 136 mEq/L (48 h). Serum creatine kinase rose to 26,760 at 24 h with neither symptoms nor acute kidney injury, decreasing gradually with forced alkaline diuresis. However, on the fourth hospital day, he developed burning pain, warmth and erythema in both lower legs, followed on the next day by severe pain, parasthesiae, non-pitting edema, muscle weakness and prominent bilateral drop foot with absent ankle muscle stretch reflexes. Anterotibial compartment syndrome was suspected. Compartment pressure was measured using standard technique 1 and found to be significantly increased: 38 mmHg (right leg) and 30 mmHg (left) (normal 0–8 mmHg). The patient was monitored, improving spontaneously with time and hydration, but dorsiflexion remained severely compromised. Electromyography before discharge showed distal bilateral peroneal neuropathy. Tibial nerve conduction was normal. Since bilateral drop foot persisted, the patient was discharged to a rehabilitation centre and started using bilateral corrective bracing. Regular electrolyte monitoring was started.
Discussion
Primary polydipsia occurs in up to 25% of patients with chronic psychiatric disorders (especially schizophrenia), related to the disease, its treatment, or both.2 Urine output fails to match intake >10L per day and water intoxication and hyponatremia may develop. Rhabdomyolysis is a rare complication of hyponatremia.3 We report our patient’s second episode of central nervous system symptoms due to severe hyponatremia, caused by primary (so called psychogenic) polydypsia. Although antipsychotics were the most common medical drug involved in rhabdomyolysis, 4 they were unlikely to be implicated here as they had been administered for years and the patient’s previous episode had also been hyponatremia-associated. When rhabdomyolysis occurs, serum creatine kinase levels rise within hours more than five times the upper limit of normal, constituting the diagnostic hallmark of rhabdomyolysis and accompanied by other muscle enzymes (Serum aspartate aminotransferase, lactate dehydrogenase, aldolase) and the appearance of released myoglobin in the urine. Here, within 3 h of presentation and before the severely depleted serum sodium of 110 mEq/L changed, his serum creatine kinase levels steeply rose (748 to 8000 IU/L) and myoglobinuria was detected – indicating that rhabdomyolysis was a manifestation of severe hyponatremia, not its correction.
Fortunately, it was not associated with acute kidney injury, reached its climax 24–48 h after admission (creatine kinase 26,750) and resolved. This is in line with the kinetics of serum creatine kinase which is the most sensitive laboratory marker of muscle injury and begins to rise within 2–12 h following the onset of muscle injury reaching its apogee within 24–72 h. Two days later, the patient developed the typical symptoms and signs of an acute anterotibial compartment syndrome, most notably, bilateral and persistent drop foot due to peroneal nerve damage.
Electrolyte disorders mediating Rhabdomyolysis.*

Full references can be obtained from the authors upon request.
Rarer than hyponatremia itself at a ratio of about 1:10.
The mechanism is not fully understood. Possibly, decreased sodium entry into muscle cells is deleterious to the normal transmembrane sodium/calcium exchange, increasing intracellular calcium accumulation that leads to activation of cytotoxic enzymes. 6 Whatever the mechanism, hyponatremia-associated rhabdomyolysis in our patient was followed by acute anterotibial compartment syndrome.
Causes of the acute anterotibial compartment syndrome.
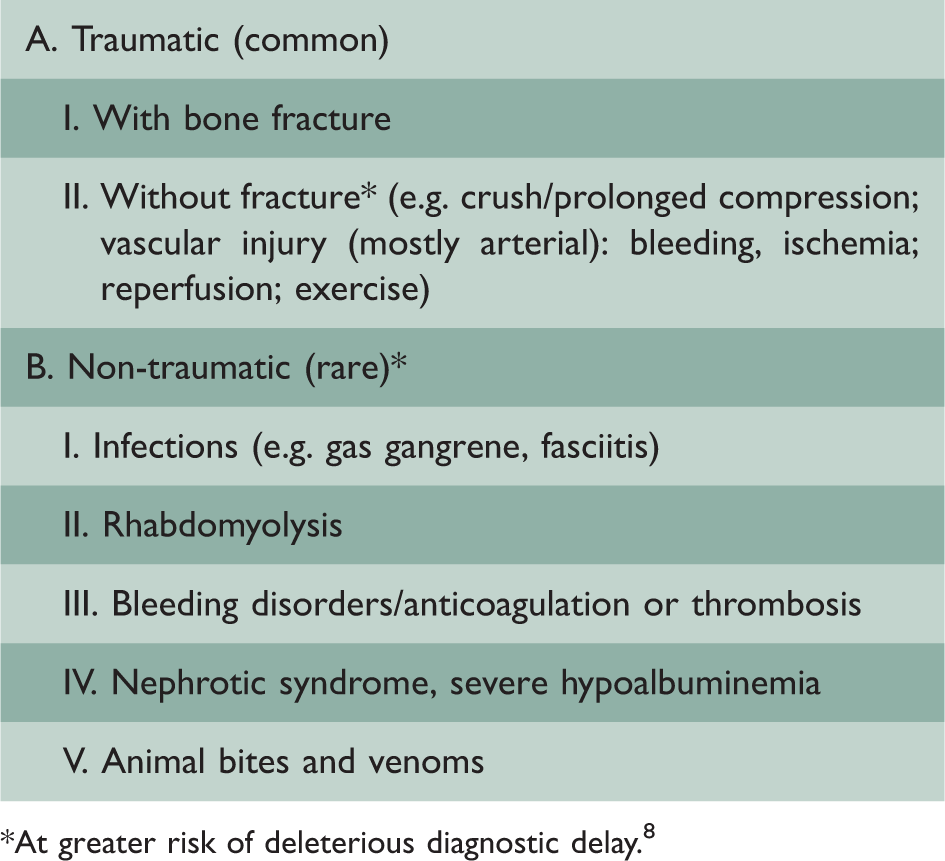
At greater risk of deleterious diagnostic delay. 8
Severe pain is the most sensitive clinical marker of anterotibial compartment syndrome. The hyponatremia-rhabdomyolysis-acute compartment syndrome sequence was reported in just two other patients to the best of our knowledge9,10 (another who also had primary hypothyroidism and adrenal insufficiency) and is poorly recognized. Its rarity, possibly due to an occult anatomical susceptibility, does not detract from the importance of this association. Anterotibial compartment syndrome, confirmed here by the increased intracompartmental pressure readings and in another patient by MRI of the anterior compartment muscles, can be a limb-threatening emergency. Faulty or delayed diagnosis may require immediate surgical intervention (fasciotomy) aimed at decreasing pressure within the compartment and restoring blood flow. 1
Conclusions
Our report highlights potential complications of severe hyponatremia which are not well recognized, as well as the fact that ‘rare times rare’ situations are encountered in clinical medicine. On recovery from hyponatremia, any significant leg pain should trigger the consideration of anterotibial compartment syndrome as well as urgent evaluation and treatment.
Footnotes
Declarations
Acknowledgements
None
Provenance
Not commissioned; peer-reviewed by Kaushik Sanyal.