
Abstract
Objectives
Evaluation of immune profiles in human breast cancer using high-sensitivity detection and analysis methods.
Design
Cohort comparative analysis studies of breast tissue.
Setting
Human hospital and laboratory healthcare facilities.
Participants
Women over 18 years.
Main outcome measures
Evaluation of the comparative immunophenotype of human breast carcinoma and normal breast tissues.
Results
Leukocyte density and specific subgroups of lymphocytes and macrophages were generally higher in breast cancers compared to normal breast tissues. CD3, CD4, CD45RO, CD45RA(2H4), CD45 and HLA Class II (on TIL) were significantly expressed on breast tumour tissues compared with normal tissues (p < .01). Some 30% of T-cells were γδ-TCR positive, but the majority were αβ-TCR in type. CD19 (B-cell), CD14 (FMC32 and 33) and HLA Class I levels (epithelial and TIL) showed no significant differences. IL-2α receptor expression was low or absent on most TIL.
Conclusions
High-sensitivity and image analysis techniques permitted accurate characterisation of the TIL infiltrate for immune profiling. Breast carcinoma showed predominance of CD4 T-cells of mainly memory phenotype. Normal breast tissues showed low leukocyte infiltration. Further correlation of these findings with clinical outcome, including survival, is proceeding with encouraging results.
Keywords
Introduction
Leukocytes are consistently associated with human breast carcinomas. T-cells represent the predominant cell type within infiltrating leukocyte/lymphocyte (TIL) populations.1–4 An increased density of TILs in breast cancer appears broadly associated with improved survival following surgical resection of the tumour,5–9 has been additionally associated with improved response to adjuvant and neo-adjuvant chemo-radiotherapy,10–13 and has also recently associated with PD-1/PDL-1 expression. 14
The specific lymphocytic phenotype has been less clearly defined. Both CD8+ cytotoxic T-cells and CD4+ helper T-cells are widely considered to protect against oncogenesis,15–17 while recent data indicate that CD4+CD25+ regulatory T-cells may actually suppress the antitumoral immunological response. 18 Other authors have found that increased expression of CD3+ has been associated with improved treatment response.19,20 The precise qualitative details of the nature of the infiltrate have been complex to understand, and some disparity remains within the literature regarding the major subpopulations within the lymphoid infiltrate in normal breast and breast carcinoma tissues, particularly regarding the predominance of CD4+ or CD8+ cells.15,16,21
The underlying causes of the variability regarding the characterisation of TILs may partly reside in the sensitivity of the detection methods used. Most studies have used lower sensitivity, non-heavy metal enhanced methods to identify the component cell types of the infiltrate. Consequently, cells with surface molecules in low copy number may not be demonstrated by standard diaminobenzidine immunoperoxidase staining. However, at least a seven-fold greater detection sensitivity for low copy number surface molecules can be achieved using heavy metal enhanced DAB methods to reveal greater numbers of positive cells than unenhanced DAB staining.22,23
Another perhaps even more crucial reason for the considerable variation in the findings of past studies resides in techniques used for quantitation of cellular immunophenotypes. Traditionally, manually graded microscopic quantitation methods have been used almost universally to measure and compare results. Slides of tissue sections are assigned a representative grade of density on a discontinuous ordinal scale such as 0, +/−, +, ++, +++ and ++++. Considerable intra- and interobserver errors exist within standard light microscopic direct manual quantitation methods.24–26 Video image analysis systems have provided a more standardised and objective method of cell quantitation, although manual quantitation still remains the standard methodology used. Comparison of mononuclear infiltrates from different tumours is however an onerous and imprecise task using direct visual methods. 27 Therefore, the novel technique of computer-assisted video image analysis, previously reported by Coventry et al., 28 offers an approach towards quantitation of cellular infiltrate within breast cancer with better standardisation and reproducibility.
If the immunophenotype could be accurately determined in breast cancers, then the association with longer term survival could potentially be more reliably evaluated.
The aim of the present study was to use monoclonal antibody immunostaining with higher sensitivity nickel-enhanced DAB immunochemistry and compare both standard manual visual quantitation and video image analysis quantitation methods to define the immune profile (major TIL subpopulations) of normal breast and breast carcinoma tissues, including the relative balance of CD4+ or CD8+cells.
Methods
The immunostaining and analysis methodology for this study was described previously in Coventry et al. 28
Preparation and immunostaining of breast tissues
Comparison was made between 25 primary breast carcinoma and 10 histologically normal tissue samples taken directly following surgical resection, immediately cryopreserved and then sectioned according to protocol. The samples were taken from surgical specimens by the attending pathologist during surgical pathology dissection at Flinders Medical Centre and Flinders University, Adelaide. Investigators were not involved in the surgery or pathology reporting. Studies were approved by the Institutional Human Research Ethics Committee and data were deidentified for analysis and reporting. Samples were evaluated by investigators without knowledge of the pathology details to avoid bias. Normal breast samples were taken from breast reduction specimens and confirmed non-malignant breast tissues.
Monoclonal antibodies
Monoclonal antibodies used.
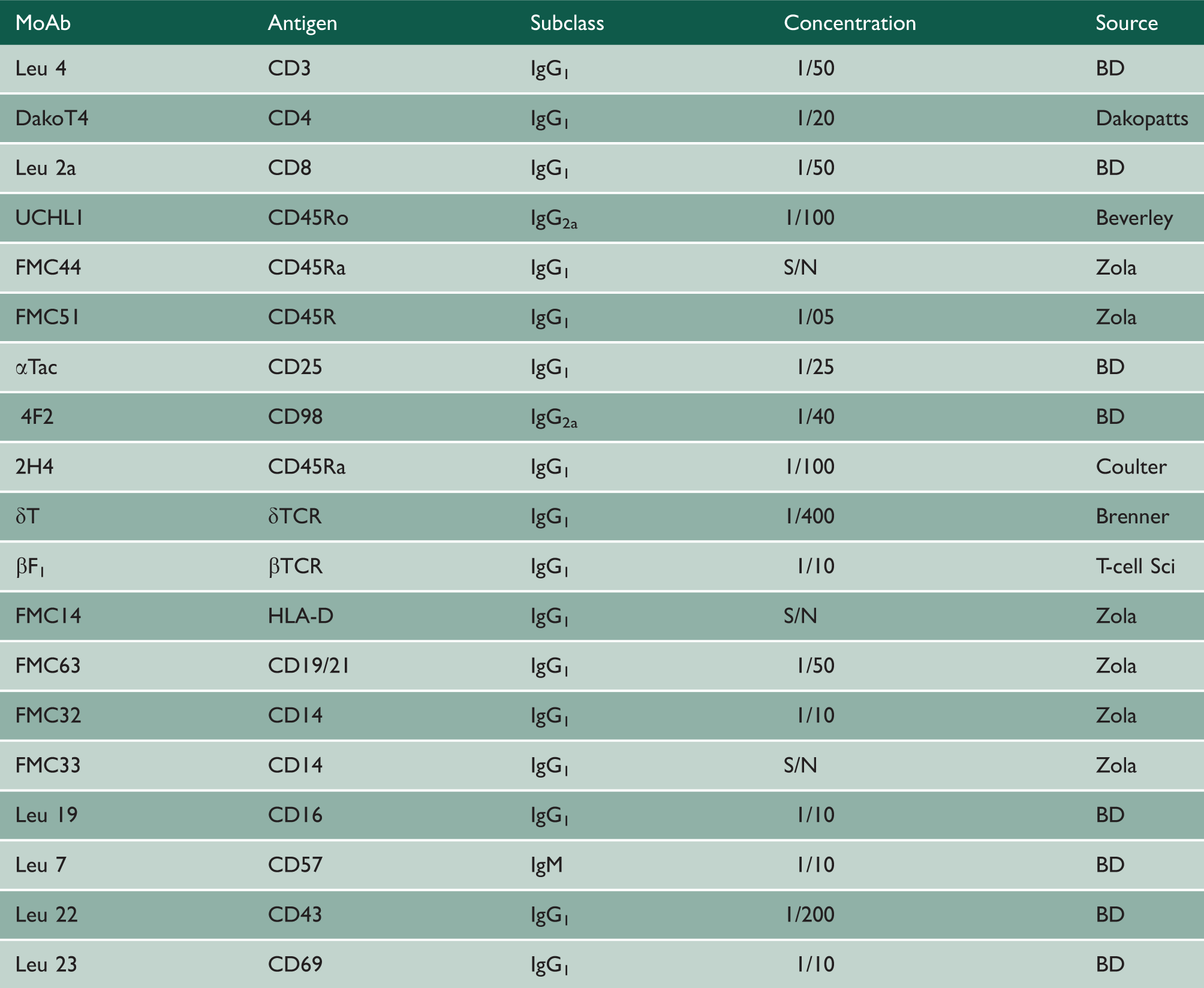
Immunostaining
Horse antimouse biotinylated second antibody was incubated for 30 minutes, with endogenous peroxidase blocking using a 1% solution of H2O2 in 70% ethanol. Avidin–biotin immunoperoxidase complex was incubated for 45 minutes using Vectastain kit reagents (Vector Laboratories, Burlingame, CA). Importantly, 3,3′-diaminobenzidine (Sigma, St Louis, MO) enhanced with 0.08% nickel chloride was used for higher sensitivity. Three five-minute phosphate-buffered saline washes between steps ensured adequate removal of non-bound antibodies and reagents.
Direct microscopic visual quantitation
The stained tissue sections were scored on a grading system of 0, +/−, +, ++, +++ or ++++ by three independent observers (BJC, JB, JMS) to evaluate average density of cells per unit area of section at ×250 magnification. The results of the 25 breast carcinoma and 10 normal breast tissue samples were analysed for the degree of cellular infiltrate for each antibody. A grade was assigned for each tissue, both normal and tumour, and then recorded.
Computer-assisted video image analysis quantitation
Twenty of the stained tissue sections were examined for quantitation using video image analysis, as previously described. 28 Briefly, a microscope head-mounted video camera captured serial images across an immunostained tissue section. Thresholds were chosen to detect reaction product, and total pixel density measurements were made after background correction. 28 Data sets for each consecutive video field were made, and graphs were plotted for each tissue section scanned using Statgraphics time-series analysis (version 4.0; Statpoint Technologies, Warrenton, VA).
Statistics
Statistical analyses were performed using SAS version 9.2 (SAS Institute Inc., Cary, NC) and SPSS Statistics version 20 (IBM, Armonk, NY).
Results
Descriptive statistics
Patient and primary breast tumour details.

ID: infiltrating ductal; IL: infiltrating lobular; M: medullary; Mod. = moderately differentiated; NA = not available/reported; UD: undifferentiated; + = tumour involved lymph node(s); − = non-tumour involved lymph node(s); (x/y) = no. of positive nodes (x) out of the total examined (y).
Direct visual quantitation
The frequency percentage of visual grades assigned for the 25 breast carcinoma and 10 normal breast tissue samples tissues were represented on histograms (Figure 1) displaying each grade of cellular infiltrate for each specific monoclonal antibody.
Normal breast tissues
Low numbers of lymphocytes were present in within normal breast tissue. T-cells predominated with a T4:T8 ratio of 1 and an equal proportion of naive CD45RA to memory CD45RO cells. Most of the T-cells were αβ-TCR in type with approximately 10% or less being γδ-TCR positive. Very small numbers of B-cells, CD16 positive cells and macrophages were located interstitially between the breast ducts. Most of the mononuclear cells in normal breast tissues were IL2α receptor negative, but HLA-D and HLA-DQ positive. The duct epithelium expressed moderate levels of HLA-D in about half the cases examined. HLA-Class I (β2-microglobulin) was expressed at moderate levels on normal breast duct epithelium examined.
Histograms comparing manual visual grades of infiltrate found in normal breast and primary breast carcinoma tissues with respect to immunostaining for various antigens.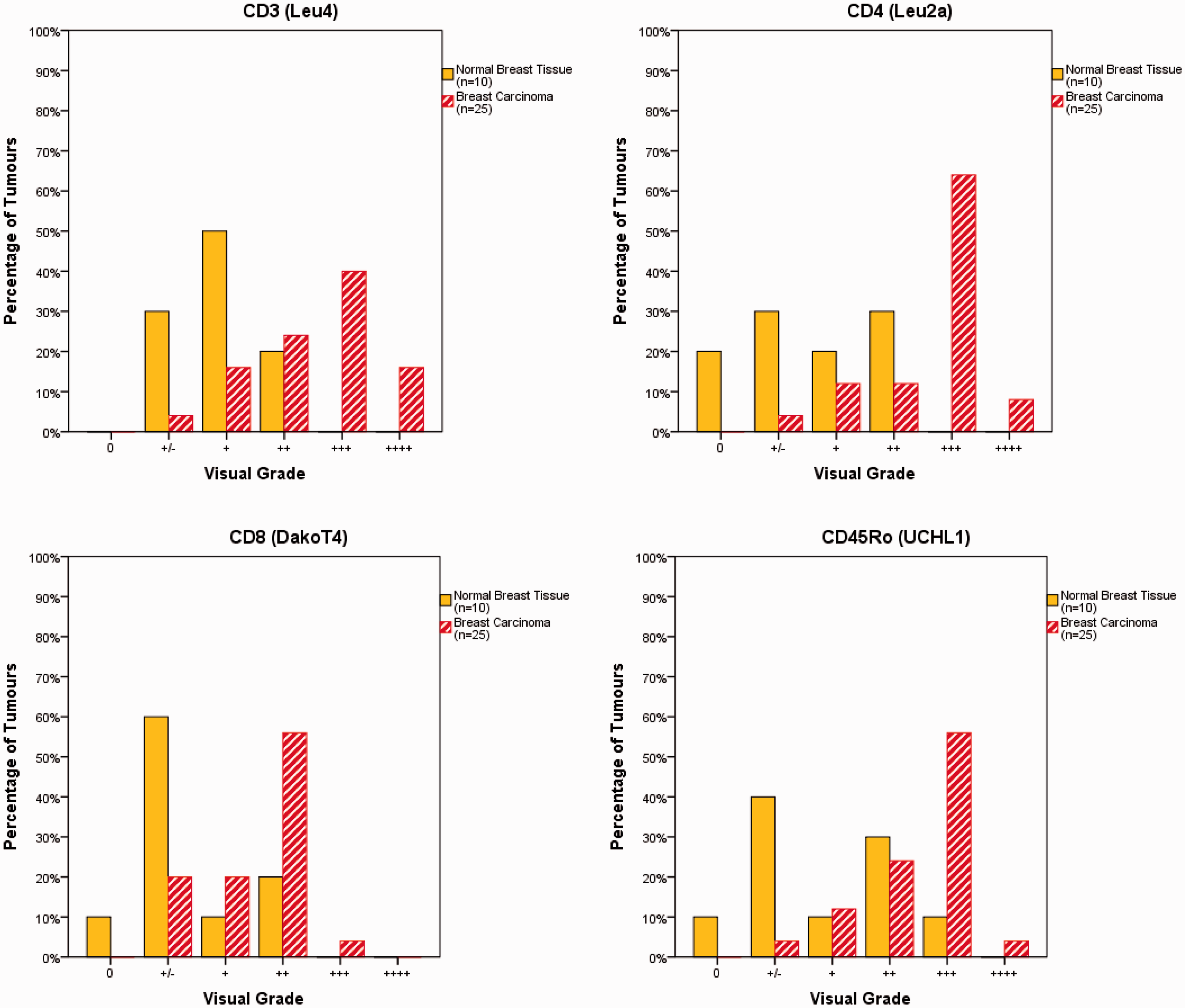
A novel finding was that some γδ-T cells were present in an intraepithelial location in the ducts of normal breast tissue (Figure 2(a)). Double immunostaining with IgA monoclonal antibodies showed these γδ-T cells to be associated with, but separate from, IgA producing cells (Figure 2(b))
Breast carcinoma tissues
The mononuclear infiltrate in breast carcinoma contained mainly T-cells, which were present in much larger numbers than in the normal tissues. There was a predominance of CD4 cells (T4:T8 ratio of >1; significant) and a predominance of memory CD45RO cells over naive CD45RA cells (not statistically significant). No statistically significant difference was found between the grading of CD3 positive cells and CD4 cells in the tumour infiltrates (p = .978), but CD4 and CD8 cell gradings were highly statistically significantly different (p < 0.001). The proportion of T-cells that were γδ-TCR positive was 30%, with the majority of cells constituting αβ-TCR in type. IL-2α receptor expression was low or absent on TIL in all but three tumours, and HLA-D was expressed heavily on TIL in all but one tumour. HLA-DQ was expressed on almost all TIL at moderate to high levels. HLA-D was expressed on tumour cells at low levels in approximately 25% of tumours tested, whereas HLA Class I was expressed on tumour cells at moderate to high levels in 70% of tumours.
(a) High-sensitivity staining showing a γδ-T cell in an intraepithelial location between ductal cells of normal breast tissue. (b) Intraepithelial γδ-T cell shown associated with IgA-producing cells using double staining with IgA monoclonal antibodies.
Low numbers of B-cells and CD16 positive cells were present. Macrophages were present in tumours in a greater proportion than in normal breast tissues. Notably, CD45 labelled more cells than were apparently accounted for by all cells labelled by T, B, CD16 and macrophage antibodies.
When breast tumour tissues were compared with normal tissues, the excess numbers of CD3, CD4, CD45RO, CD45RA(2H4), CD45 and HLA Class II (on TIL) were statistically significant (p < .01, Kolmogorov–Smirnov). CD19 (B-cell), CD14 (FMC32 & 33) and HLA Class I levels (epithelial and TIL) showed no statistically significant differences.
Video image analysis
The results from VIA assessment of the same immunoperoxidase-stained tissue sections used for the direct visual quantitation data above are depicted in Figure 3. Results for the average area under each of the CD3 curves and direct visual grades for each case have previously been published.
28
Data in Table 3 depict the VIA pixel measurements in ascending order of magnitude for the 20 individual breast cancer specimens stained with CD3, with the corresponding ordinal grade measured by manual visual method for each particular tumour shown alongside.
Video image analysis graphical profiles for serial sections from five separate tumours immunoperoxidase stained using various primary antibodies for comparison with direct visual quantitation data in Figure 1. Vertical axis is density of staining; Horizontal axis is distance across the tissue section.
28
Axes are the same for all graphs shown. Comparison of VIA pixel value with assigned manual visual grade.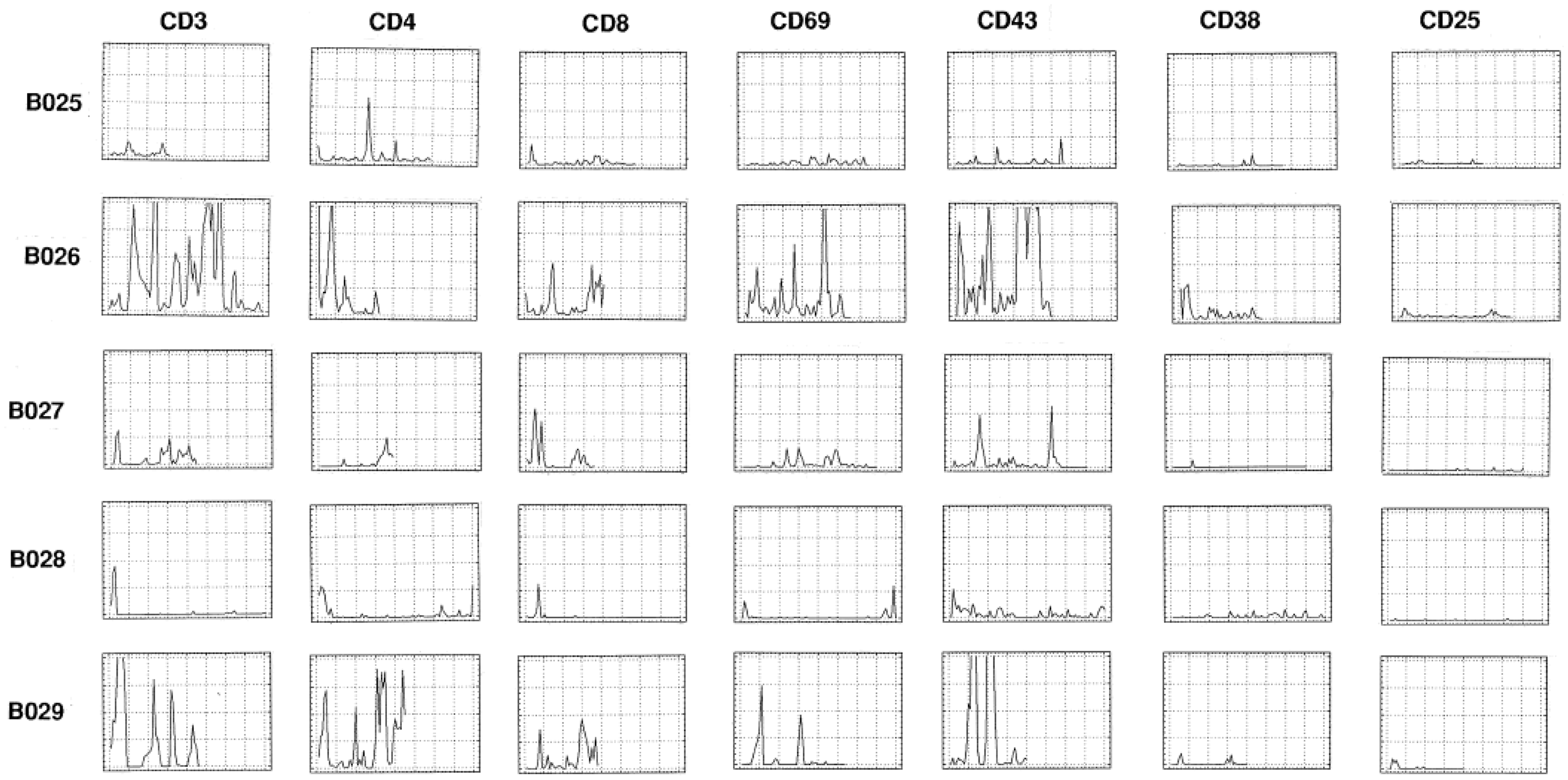

Associations between VIA pixel values and age/tumour size
VIA pixel density correlated with patient age and tumour size.

Pearson correlation coefficients; n = 20.
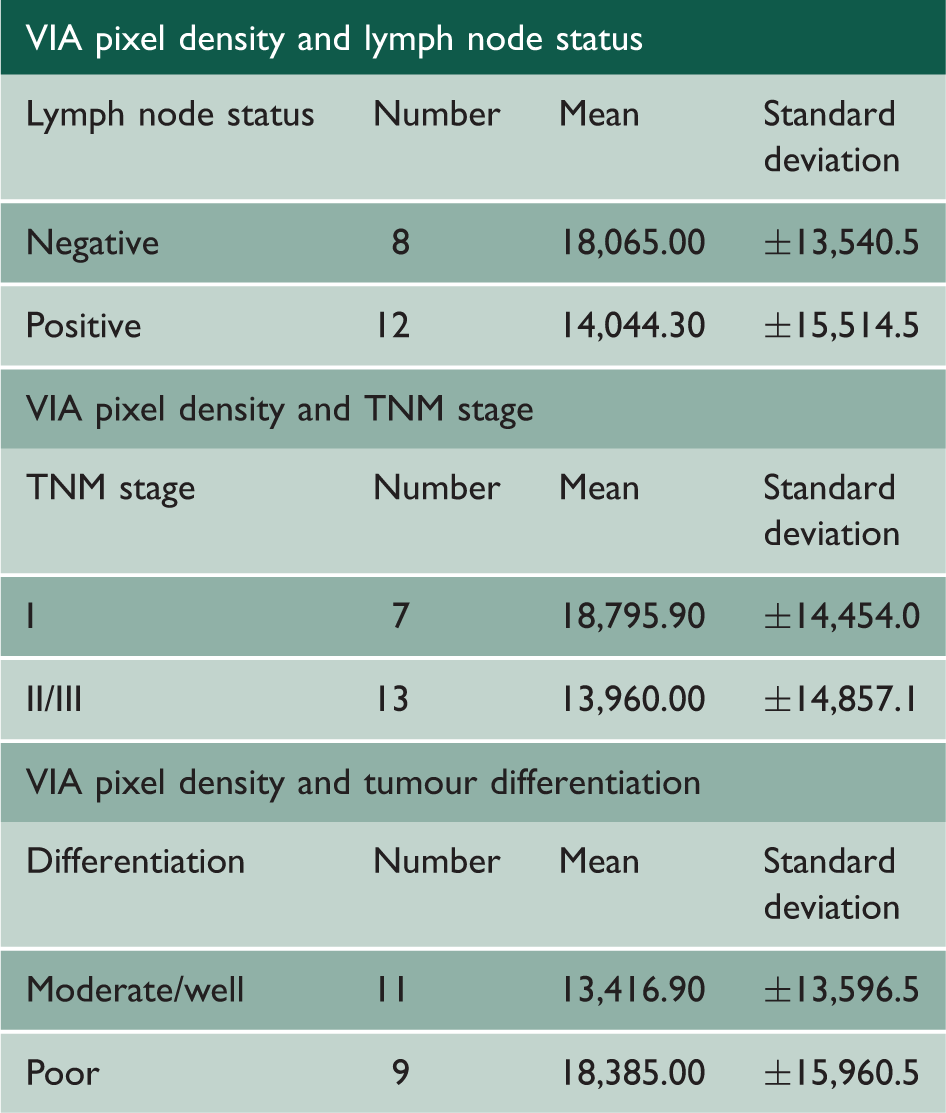
Associations between VIA pixel values and lymph node status, TNM stage and differentiation as assessed using independent samples t-Tests
VIA pixel density correlated with lymph node status, TNM stage and tumour differentiation.
Discussion
Detailed immune profiles of breast carcinomas and normal breast tissues were reported in this study, which is of increased relevance given the current interest in immunotherapeutic approaches to breast cancer management.29,30 The most sensitive techniques were used to obtain a detailed analysis of major subpopulations within the lymphoid infiltrate in breast carcinoma and normal breast tissues. By combining high-sensitivity, heavy metal enhanced di-aminobenzidine immunoperoxidase staining methods with computer-assisted video image analysis for cell quantitation, the most accurate evaluation was possible, and this was compared with standard manual visual quantitation.
This revealed several major qualitative and quantitative differences in the cellular infiltrates of both normal and malignant breast tissues. T-lymphocytes were present in very low numbers around breast ducts in normal tissues but were present in large numbers within and around breast carcinomas. Some 90% of tumours were shown to have infiltrates of ++ or greater compared to 20% for normal breast tissues. Most of the T-cells were CD45RO indicating previous antigen priming 31 and the proportion of CD4 cells was greater in tumours. The proportion of γδ-TCR positive cells was also greater in tumour tissues, perhaps suggesting less specific T-cell mechanisms might also be operational in the tumour microenvironment. An observation which might also support this notion were the increased macrophage numbers associated with tumour tissue compared to normal tissues, with over 75% of tumour samples having a ++ or greater infiltrate compared to 12% for normal tissues. B-lymphocytes were slightly increased in tumour tissues over normal tissues, but the B-cell infiltrate was sparse even in tumours. Similarly, sparse infiltration of CD57 positive cells (neutrophils) was noted in both tumours and normal tissues.
Collectively, these results show that tumour tissues possess a clearly different leukocyte infiltrate to normal breast tissues. Quantitative differences were present in T-cell and macrophage numbers; in addition, qualitative differences were found. CD4 to CD8 subgroup proportions, δ-TCR positive cells and CD45RO positive cells were all elevated in tumours. These findings suggest that T-cells, and to a lesser extent macrophages, either proliferate or are attracted to the tumour microenvironment to aggregate in considerable numbers in most of the breast tumours examined. Most of these cells display the 180,000 kDa form of the leukocyte common antigen implying previous antigen priming and cellular activation. 32 Expression of the CD25 molecule as a marker of early activation was very low in normal breast tissue and also low in the infiltrating cell population associated with breast tumours, supporting other studies.33,34 CD4 cells appeared to predominate over CD8 cells in the breast tumours tested.
T-cells consisting of mainly αβ-TCR CD4 cells comprise the major component of the tumour infiltrate of breast tumours, and possess the CD45RO phenotype, are HLA class II positive in 95% of tumours examined and show almost uniform absence or very low expression of the p55 and p70 chains of the IL-2R. Taken together, these findings suggest that the lymphocytes have been exposed to antigen, but are not activated, being down-regulated. Considering the data from VIA quantitation of immunostained cells from the same tumour sections as used for direct visual assessment, several features are apparent. Clustering of CD3 cells within the tumour is notable from the profiles, and considerable variations are observed between the direct visual grade and the area under the VIA curve. The limitations imposed by the quantal nature of the direct visual grading method become apparent from this comparison.
Novel VIA techniques appeared to be a useful tool that allows for quantitatively correlating staining density as a continuous variable with various patient characteristics. Such analysis has often been difficult previously. Staining density was shown to correlate positively with tumour size, but no association was found with lymph node status, TNM stage or degree of differentiation. This is likely due to the small sample size, although one of the potential benefits of VIA is that larger studies can be conducted more easily, compared with time-intensive and slower manual visual grading.
The VIA methods in this study also provided graphical profiles for each of the different antibodies. This allowed more detailed representation of the pattern of distribution of the subpopulations of lymphoid infiltrate within the tumour. Features such as clustering of cell types can also be observed and quantitated using VIA. 28 Moreover, it also allowed for the association comparison of areas within the tumour where cellular subgroups could be identified as either overlapping or distinct. Analysis of cytokine expression and cytokine receptor expression within the tumour microenvironment using these methods is under current investigation.
Our previous work demonstrated that both dendritic cell number and activation were low in human breast cancers and showed an association between density of CD1a cells and five-year survival, although non-significant at the p = .05 level.35,36
The importance of the current findings and techniques used in this study are that better understanding of the distribution of the tumour infiltrating leukocyte population within human breast carcinomas is now possible. Further work is revealing the implications of TIL characteristics for clinical outcome, including longer term survival, which is currently being actively evaluated in greater detail.
Conclusion
The results obtained in this study indicate that although primed T-cells predominate, other immunological cell types are present. These other cell types and the relationship to the structural morphology and interaction with CD3 cells require further investigation. Indeed, significant interaction or cooperation between cell types in the tumour inflammatory infiltrate likely does occur. More detailed analysis of the distribution of immunological cells within the TIL infiltrate using high-sensitivity immunostaining and VIA techniques offers a logical approach recommended for further investigations in this area. The potential importance and significance of these findings lie in the association between breast cancer TIL immune profile and clinical outcome, including survival.