
Abstract
Objectives
Over half of the UK population holds a driver's licence. The DVLA have produced guidelines to ensure drivers with medical conditions drive safely. Doctors should ensure that patients are given appropriate information and advice if they have a medical condition affecting their driving. We sought to evaluate doctors' knowledge of DVLA guidelines.
Design
A 25-point questionnaire was designed from DVLA guidelines (‘The DVLA Questionnaire’). Five questions were included for each of neurology, cardiology, drug and alcohol abuse, visual, and respiratory disorders.
Setting
Ealing Hospital, Northwick Park Hospital, Watford General Hospital, Norfolk and Norwich University Hospital and Leeds Teaching Hospitals Trust.
Participants
140 UK doctors.
Main outcome measures
Questionnaire scores assessing knowledge of DVLA guidelines in five specialty areas.
Results
The median overall questionnaire score was 28%, interquartile range 20–36% and range 0–100% [Watford 28%, Leeds 30%, Norfolk and Norwich 36%, Ealing 30%, Northwick Park 28%]. There were no significant differences between the scores for each centre (p = 0.1332), Mean scores for specialty areas were: neurology 33.1%, standard deviation 22.1; cardiology 35.6%, standard deviation 26.9; drug and alcohol abuse 30.6%, standard deviation 23.8; visual disorders 33.9%, standard deviation 23.5 and respiratory disorders 20.3%, standard deviation 24.8; overall score 30.7%. There was no significant difference between the scores of the specialty areas (p = 0.4060).
Conclusions
Knowledge of DVLA guidelines in our cohort was low. There is a need for increased awareness among hospital doctors through focused education on driving restrictions for common medical conditions. Improving physician knowledge in this area may help optimise patient safety.
Introduction
Driving has long been established as a significant cause of mortality and morbidity. In 2013, 1713 people were killed in road traffic accidents in the United Kingdom (UK) and over 20,000 were seriously injured. 1 The social and financial implications are substantial; every fatality costs an average of £1,703,822 through a combination of lost output, human costs, and medical and ambulance expenses; each serious injury consumes on average £191,462. 2 Given that the number of driving licence holders in the UK is nearing 38 million 3 it is likely that road traffic accidents will continue to burden the National Health Service (NHS) in years to come.
Certain medical conditions and episodes of illness are potentially debilitating for drivers, and therefore the Driving Vehicle Licensing Agency (DVLA) has produced a set of guidelines that clearly explain under what circumstances these medical conditions restrict driving privileges. 4 Examples of their recommendations include not driving for 6 months following a single unprovoked epileptic seizure, 12 months if an individual has multiple attacks of cough syncope, and 4 weeks following a coronary artery bypass graft. 4 It is a requirement under both statutory 5 and European Union 6 law that licence holders and applicants adhere to these recommendations and inform the DVLA of any medical condition which may affect their ability to drive safely. The legal responsibility for notification of the DVLA lies with the patient. However, the General Medical Council (GMC) emphasises the clinician’s responsibility to notify patients when they have a condition or diagnosis affecting their ability to drive and to make them aware of their legal obligation to inform the DVLA about their condition. 7 In addition, when a patient continues to drive despite clear guidance to stop driving or when the patient refuses to accept the diagnosis, it ultimately becomes the doctor’s responsibility to notify the DVLA. 7
In practice, it has been suggested that clinicians neglect this responsibility; a 2003 retrospective study in a UK NHS Hospital showed that only 16% of patients with conditions that legally restrict driving privileges were given any kind of driving-related instruction; with only half of these given accurate direction. 8 O’Neill et al. 9 via postal survey and Kelly et al. 10 via face-to-face data collection demonstrated a low level of clinician knowledge related to driving recommendations in the elderly medically unwell population. King et al. 11 investigated clinician knowledge of medical fitness to drive in primary and secondary care settings, with respondents spanning the seniority range from senior house officer to consultant. The number of clinicians who raised the topic when appropriate, and the subsequent accuracy of their advice on driving restrictions in patients with common diagnoses, for example, myocardial infarction and epilepsy, was inadequate. Frampton provided further evidence of this problem in a study of doctors working in emergency departments (ED), notably in the cases of patients who would be discharged directly from the ED following resolution of symptoms and wrongly assume themselves fit to drive. 12 Frampton also raises the issue of confusion over responsibility between the different health-care workers and different teams involved in patient care.
This study assesses clinicians’ knowledge of the DVLA medical fitness to drive parameters across various medical specialties with the aim of establishing specific targeted improvement. Parameters examined by this study include those relevant to the following specialties: neurological disorders, cardiology disorders, substance misuse disorders, visual disorders, and respiratory disorders.
Methods
Questions included in The DVLA questionnaire, covering DVLA guidelines in five subject areas. Answers are included in brackets.

TIA: Transient ischaemic attack; CABG: coronary artery bypass graft; ACS: acute coronary syndrome; DVLA: Driving Vehicle Licensing Agency.
The questionnaire was distributed to junior doctors and senior house officers at five study centres: Ealing Hospital (London), Northwick Park Hospital (London), Watford General Hospital (London), Norfolk and Norwich University Hospital (Norwich) and Leeds Teaching Hospitals Trust (Leeds). The questionnaires were distributed at planned foundation year teaching or department of medicine teaching sessions without prior notification. A link to an identical online questionnaire via SurveyGizmo 13 was also sent out to junior doctors via email. Participants completed one of either a paper or online questionnaire. Each question had a maximum score of 1 mark, there was no negative marking. In questions that had more than one correct answer, a mark was awarded if the doctor was able to give at least one of the correct responses. For each specialty area, the maximum score was 5 marks, and the maximum score for the whole questionnaire was 25 marks. Participation in the study was purely voluntary and no incentives were offered. The questionnaires were anonymised and marked by two independent reviewers.
Results
The DVLA Questionnaire was distributed to a total of 189 doctors across five study centres. A total of 140 doctors including foundation year doctors and senior house officers completed the questionnaire (Watford General Hospital n = 30, Leeds Teaching Hospitals Trust n = 26, Norfolk and Norwich University Hospital n = 24, Ealing Hospital n = 30 and Northwick Park Hospital n = 30). The response rate was high at 74%. Total questionnaire scores were tightly clustered around a median of 28% (interquartile range 20–36%) (Figure 1). Some participants scored very highly and others scored very poorly – two doctors answered all questions correctly and two doctors failed to answer any questions correctly. We checked for normality using the D’Agostino and Pearson omnibus normality checks; the data obtained was not normally distributed.
Box and whisker plot showing questionnaire scores (%) for all participants from the five study centres and for each individual study centre. The median score, interquartile range and range are displayed.
Figure 1 shows box and whisker plots for the overall questionnaire scores for participants in each individual study centre; Watford General Hospital (median score 28%, interquartile range 24–32%, range 12–44%), Leeds Teaching Hospitals Trust (median score 30%, interquartile range 21–36%, range 8–92%), Norfolk and Norwich University Hospital (median score 36%, interquartile range 27–48%, range 8–100%), Ealing Hospital (median score 30%, interquartile range 17–36%, range 0–48%) and Northwick Park Hospital (median score 28%, interquartile range 17–32%, range 0–60%). Following logarithmic transformation of the data, a one-way analysis of the variance was performed; there were no significant differences between the scores of each centre (p = 0.1332).
Questionnaire scores for each specialty.
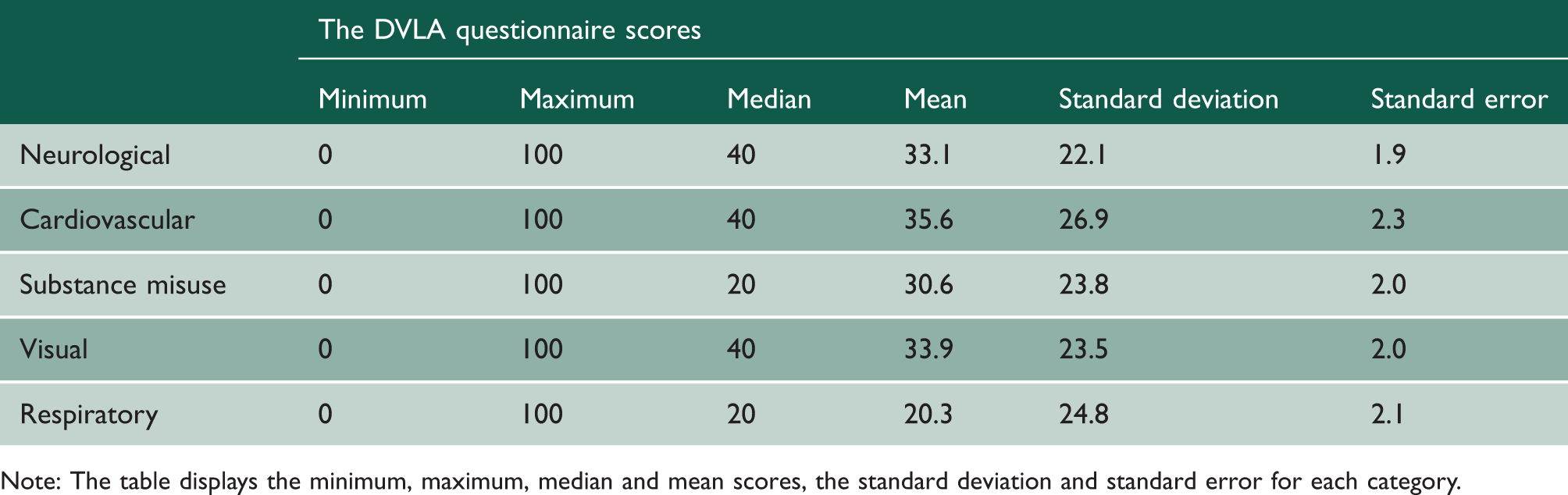
Note: The table displays the minimum, maximum, median and mean scores, the standard deviation and standard error for each category.

Mean questionnaire scores (%) for the sets of questions asked in each of the five specialty areas covered.
Figure 3 shows the percentage of participants answering each specialty question correctly. Question 22 (how long must a patient with multiple attacks of cough syncope cease driving for?) was answered correctly by only 11% of participants. Question 17 (In monocular vision loss, should the DVLA be notified?) was answered correctly the most often with 68% of participants providing the correct answer.
Percentage of participants answering each individual question correctly in the specialty areas of neurological disorders, cardiovascular disorders, substance misuse, visual disorders and respiratory disorders.
Several questions required the participants to state for how long certain conditions disqualify patients from driving. Less than 40% of doctors knew patients are disqualified from driving for six months after an unprovoked epileptic seizure. Only 21% of participants were aware of driving restrictions following a stroke. Only 15% of doctors correctly answered when a patient can recommence driving after an acute coronary syndrome treated with elective angioplasty.
Discussion
This multicentre study demonstrates that doctors’ knowledge of DVLA guidelines relating to commonly occurring medical conditions is consistently poor. This lack of knowledge is not limited to one or two clinical domains, but instead to all of the diverse subsets explored in our questionnaire. In total, 140 doctors across five UK centres responded to the questionnaire and the median overall score was 28%. Even in the set of questions that were most successfully answered (those relating to cardiovascular conditions) only 36% of responses were correct. At the other end of the spectrum, only 1 in 10 respondents was able to provide appropriate guidance to patients suffering from cough syncope. This is the largest and only multicentre study on this topic to date; these results provide robust evidence in demonstrating a paucity of knowledge among doctors regarding medical restrictions to driving. While there are no formal reports examining causation, this study is consistent with previously published findings, which point to a lack of formal training received either in an undergraduate or postgraduate setting.
Driving is a high-risk activity and the costs of an accident are substantial. Doctors should be concerned about medical illness and its impact on fitness to drive for two reasons. Firstly, the presence of an acute or chronic medical condition increases the risk that an individual will be involved in an accident. Based on police reports to the DVLA in 2000, causes of road traffic collisions (RTC) involving collapse at the wheel include epilepsy (38%), blackouts (21%), diabetics taking insulin (19%), heart condition (8%) and stroke (7%). 4 Estimates suggest that approximately 15 in 10,000 accidents are precipitated by loss of consciousness due to an acute medical condition. 14 In addition, drivers with chronic medical conditions are more likely to be involved in accidents and are more likely to be responsible for causing accidents than drivers without chronic medical conditions.15,16 Secondly, the risk of patients being involved in serious accidents decreases significantly if they are warned in hospital that they may be unfit to drive. 17 This is a serious and widespread problem with a simple and effective solution; doctors must inform patients about the impact of their medical conditions on their legal status as drivers and encourage them to inform the DVLA. In cases where patients refuse to contact the authorities, confidentiality must be over-ridden if there is significant risk of harm to the public.
A number of previous studies support our findings. Physicians often have poor knowledge of the medical conditions that could impact their fitness to drive, and submit poor quality medical reports relating to licensing issues.10–12,18 In our study, only 21% of doctors knew how long a patient should stop driving for after a stroke and less than 40% knew how long a person must stop driving for after a first episode of seizure. Only 15% of doctors correctly responded to the question asking when a patient can recommence driving after an acute coronary syndrome treated with elective angioplasty. These are examples of common medical conditions encountered in daily practice and also mentioned in the report of top causes of RTCs involving collapse at the wheel. 4
Our study evaluated physician knowledge across a broad range of specialties. Previous studies in this area have had relatively small sample sizes in a single centre.10–12,18 In this study, a questionnaire was distributed to a large cohort of doctors across five UK centres, increasing the robustness of our data. The majority of questions required doctors to provide numerical answers from their own knowledge; there were no multiple-choice questions and only four polar questions. This substantially reduced the likelihood of a respondent guessing the correct answer.
It is important, however, to note the limitations of our study. Our questionnaire has not been used before and its validity has not been evaluated. Our study evaluated DVLA knowledge from junior doctors and senior house officers and there was lack of representation of doctors from the registrar and the consultant level. However, junior doctors have great responsibility in the planning and coordination of a patient’s discharge, 19 so the large representation of this cohort in our study may be appropriate. Doctors’ knowledge in five University Hospital Trusts in the London and Leeds region were evaluated, thus this may not be fully representative of doctors in the rest of the country. Although 25 questions were asked across five specialties, there are some areas of practice that the questionnaire did not include, for example, endocrine disorders. However, the questionnaire was designed to focus more on the commonly encountered specialties and the level of ignorance in this area suggests a similar trend in more specialised domains.
Another aspect of the study that could be improved is the lack of representation from the General Practitioner demographic. It may be the case that many hospital-based doctors do not consider the provision of driving restriction related advice to be a part of their duty and instead expect their community-based colleagues to factor this into their care. The debate about whether primary or secondary care should accept this responsibility is one worth having, but what cannot be denied is that hospital-based clinicians must be equipped with appropriate knowledge of these guidelines for those cases in which GPs are not involved. For example, patients that attend the accident and emergency department who are subsequently discharged may be lost to follow-up – they must be informed at the time of discharge if the reason for their admission disqualifies them from driving. 12 Patients with progressive chronic conditions can decline significantly over time and must be informed when the DVLA guidelines require that they avoid driving – the responsibility lies with the physicians involved in their care, be they GPs or hospital doctors, to make an appropriate evaluation of fitness to drive and prompt these patients to take action when necessary.7,15 An area of future research would certainly be to focus on the knowledge of these guidelines among GPs throughout the UK, and likewise to analyse whether or not clinicians from primary and secondary care settings considered the administration of this advice to be their duty.
Another potential criticism of our study may be that the questions themselves are too difficult and thus could overstate the problem of clinician knowledge in this domain. However, we believe that the specific nature of the questionnaire, while no doubt challenging, reflects the need for detailed understanding in a subject as sensitive as driving restrictions. Although it may seem pedantic, a doctor believing that restrictions after a certain illness episode should be 2 months as opposed to 3 months may in itself be cause for an accident that could cost lives. While it may be argued that doctors could look up these details as and when they needed to provide them, as our study focused on extremely common illness episodes, we feel it appropriate to expect a certain level of familiarity. We also question whether clinicians would be likely to seek out DVLA guidelines multiple times per day, which would be necessary considering the frequency of such admissions. Future research in this area may look into whether or not clinicians do endeavour to seek out the appropriate guidelines when needed, even if they themselves do not have the knowledge.
Given the consistently inadequate knowledge of DVLA guidelines among physicians, the substantial financial and societal costs associated with RTCs secondary to diagnosed medical conditions, and the evidence demonstrating the effectiveness of warning patients, focused training in this area is necessary. Currently, there is no formally dedicated education on medical fitness to drive for medical students or doctors. DVLA guideline education should be considered in undergraduate training as a component of the curriculum and in postgraduate training. While a mastery of the guidelines in no way guarantees that clinicians will pass on this advice appropriately during their practice, adequate knowledge of the DVLA recommendations is a prerequisite for the delivery of appropriate advice for patients and would increase the likelihood of this taking place. There are other factors that reduce the likelihood of adherence to guidelines by physicians even when they know them; work by Cabana et al suggests that if doctors do not expect their actions to produce the desired outcome they are less likely to adhere to the suggested behaviour. 20 For the specific problem of medical conditions and fitness to drive the evidence exists to show the effectiveness of patient notification 17 and therefore it should be integrated into any provisional teaching. Provision of patient information leaflets for DVLA guidelines for each condition may help to bridge the large gap between physician knowledge and the requirements of safe practice in the interim period while a structured education system works towards providing clinicians with an adequate and much needed understanding of driving restriction guidelines.
In summary, with inadequate physician knowledge of DVLA guidelines, certain medically disqualified patients may be discharged and wrongly assume themselves fit to drive; this increases the risk of road traffic accidents and contributes to this significant and growing problem. There is a need to increase awareness of driving restrictions for common medical conditions among hospital doctors through focused undergraduate and postgraduate education.