
Abstract
Lesson
Traumatic bilateral extradural haematoma resulting from injury to the superior sagittal sinus is rare; in such cases, early surgical evacuation of the haematoma and control of bleeding from the sinus can achieve an excellent patient outcome.
Case report
A 32-year-old right-handed man was struck by a train at high speed. On scene, his Glasgow Coma Scale score was 3, and his pupils were 2 mm in diameter. Following rapid sequence induction and intubation, he was transferred to the regional Major Trauma Centre, where he was resuscitated and promptly underwent whole-body computed tomography. Computed tomography of the head showed an extensive bifrontal extradural haematoma, with underlying complex skull vault fractures including a right temporoparietal depressed skull fracture, and a fracture line extending across the midline (Figure 1); computed tomography venography demonstrated that the superior sagittal sinus remained patent. Otherwise, the remaining imaging was unremarkable.
(a) Preoperative axial computed tomography head demonstrating bifrontal extradural haematoma with underlying complex skull vault fractures including a right temporoparietal depressed skull fracture, and a fracture line extending across the midline, (b) preoperative computed tomography head 3D reconstruction and (c) postoperative computed tomography head demonstrating evacuation of the haematoma.
The patient was immediately transferred for surgical evacuation of the extradural haematoma. A bicoronal skin flap was turned, and bilateral frontal craniotomies were performed, preserving the midline skull vault overlying the superior sagittal sinus. A large bifrontal extradural haematoma was identified and cleared with copious irrigation (Figure 2). Bleeding from the sinus was controlled using a combination of chemical and physical haemostatic measures. Surgicel® (Johnson and Johnson, NJ, USA) was wrapped around Floseal® (Baxter, IL, USA) to form haemostatic ‘roulades’ that were applied to each side of the bleeding sinus. The dura surrounding the sinus was then hitched to the remaining midline skull vault with 3-0 vicryl. The bone flaps and depressed skull fragments were then replaced and secured with titanium miniplates. The skin flap was closed in two layers, and a subcutaneous wound drain placed.
Intraoperative image demonstrating preservation of the midline skull vault and use of dural tenting sutures.
Postoperatively, the patient was transferred to the intensive care unit, and subsequently to the major trauma ward. A computed tomography of the head confirmed evacuation of the extradural haematoma (Figure 1). The patient was discharged home approximately a month after his injury, with no neurological deficits, and only intermittent headaches that had completely resolved at 6-month follow-up.
Discussion
Although traumatic bilateral extradural haematoma was first described as early as 1884, 1 it is a comparatively uncommon entity, accounting for approximately 2%–5% of adults with extradural haematoma.2,3 Kett-White and Martin classified such cases into two distinct groups 4 : patients with bilateral but separate extradural haematoma located in the convexities, resulting from dura being stripped from the skull independently on both sides, either simultaneously or sequentially; and, more rarely, patients with bilateral extradural haematoma straddling the midline, resulting from injury to the sagittal sinus.
Summary of cases with bilateral extradural resulting from sagittal sinus injury.
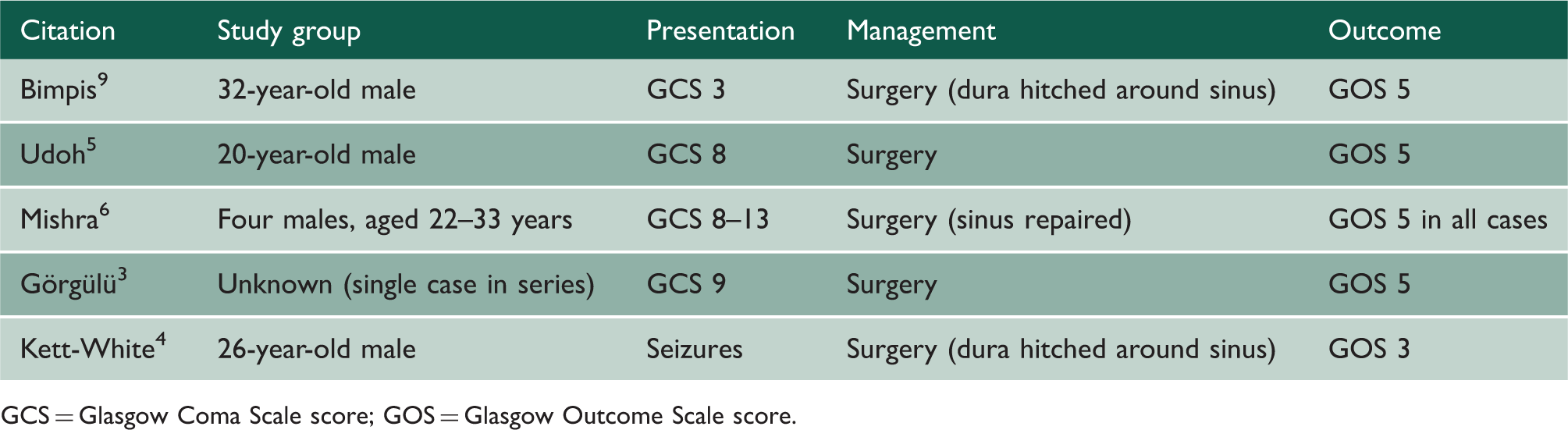
GCS = Glasgow Coma Scale score; GOS = Glasgow Outcome Scale score.
Although all identified cases with bilateral extradural haematoma resulting from sagittal sinus injury underwent urgent surgical evacuation, the operative technique varied. Control of bleeding from the superior sagittal sinus may be technically challenging. In the present case, a combination of chemical and physical haemostatic interventions was used. A potential concern with the use of Floseal® over venous tears is the risk of thromboembolic complications. 8 In our experience, wrapping Floseal® with Surgicel® to form a haemostatic ‘roulade’ prevents migration into the venous sinus. An additional operative nuance is the decision to either preserve the midline skull vault and use dural tenting sutures, or – in selected cases – expose the sagittal sinus and attempt primary repair. 6
There is often little primary brain injury in patients with extradural haematoma. The clinical corollary is that it is almost always possible to immediately replace the bone flap and rapidly wean sedation. Moreover, the overall outcome of patients with extradural haematoma that undergo timely surgical evacuation is excellent; all but one of the cases identified in the literature recovered with little or no disability (Glasgow Outcome Scale score 5). Follow-up is mandated for cases with bilateral extradural haematoma resulting from sagittal sinus injury. Although not routinely performed postoperatively, in patients with symptoms and signs suggestive of sinus occlusion, venography may be indicated.
In conclusion, traumatic bifrontal extradural haematoma resulting from sagittal sinus injury is rare. In such cases, urgent surgical evacuation is critical to reduce secondary brain injury. Although managing bleeding from the sinus may be technically challenging, a multifaceted strategy incorporating basic physical and chemical haemostatic measures is almost always successful; direct repair of the sinus is indicated only in selected cases. Overall, the outcome of patients with traumatic bifrontal extradural haematoma that undergo surgery is excellent.