
Abstract
Summary
Vaccination programmes are implemented either as new vaccines become available or evidence about them accumulates, or in response to specific situations. In the United Kingdom, development and implementation of the national immunisation programme is centrally coordinated and funded by the Department of Health on behalf of England, Wales, Scotland and Northern Ireland. A number of significant changes were made to the UK immunisation schedule for 2013/2014. Three new vaccines were introduced: intranasal influenza and oral rotavirus for children and subcutaneous shingles for older adults. To ensure protection against meningococcal C infection into adulthood, there has been a change to the schedule for meningitis C vaccination. The temporary pertussis vaccination programme for pregnant women, set up in response to an increase in the number of cases of pertussis particularly among young babies, has been extended until further notice. Furthermore, in response to large outbreaks of measles in south Wales and other parts of the UK, a national measles, mumps and rubella catch-up campaign specifically targeted at unvaccinated children aged 10–16 years was launched to ensure that all children and young people have received two doses of measles, mumps and rubella vaccine. This review describes the rationale behind these policy changes.
Keywords
Introduction
Vaccination policy refers to a plan of action adopted or pursued by a government in relation to vaccination. National immunisation schedules and programmes are implemented or amended based on vaccination policy decisions. In the United Kingdom, development and implementation of the national immunisation programme is centrally coordinated and funded by the Department of Health (DH) on behalf of England, Wales, Scotland and Northern Ireland. DH is advised by the Joint Committee on Vaccination and Immunization (JCVI), an independent expert advisory committee. JCVI makes recommendations to DH concerning vaccination policy and schedules, after considering disease epidemiology, vaccine efficacy, vaccine safety and cost-effectiveness of implementing a programme. Once a new vaccine policy has been accepted by the UK government, DH develops a strategic plan with activities, timelines, agencies and tasks to manage the implementation of the new policy. Depending on the policy, different actions will be required, ranging from simple amendment of existing activities to a major campaign for introduction of a new vaccine. Changes and additions to the immunisation programme are incorporated alongside other vaccines wherever possible to minimise the number of appointments needed and disruptions to patients and services. To facilitate the process, DH manages a network of ‘Immunization Coordinators’ who have local responsibility for implementation of new policies and effective delivery of the immunisation programme.
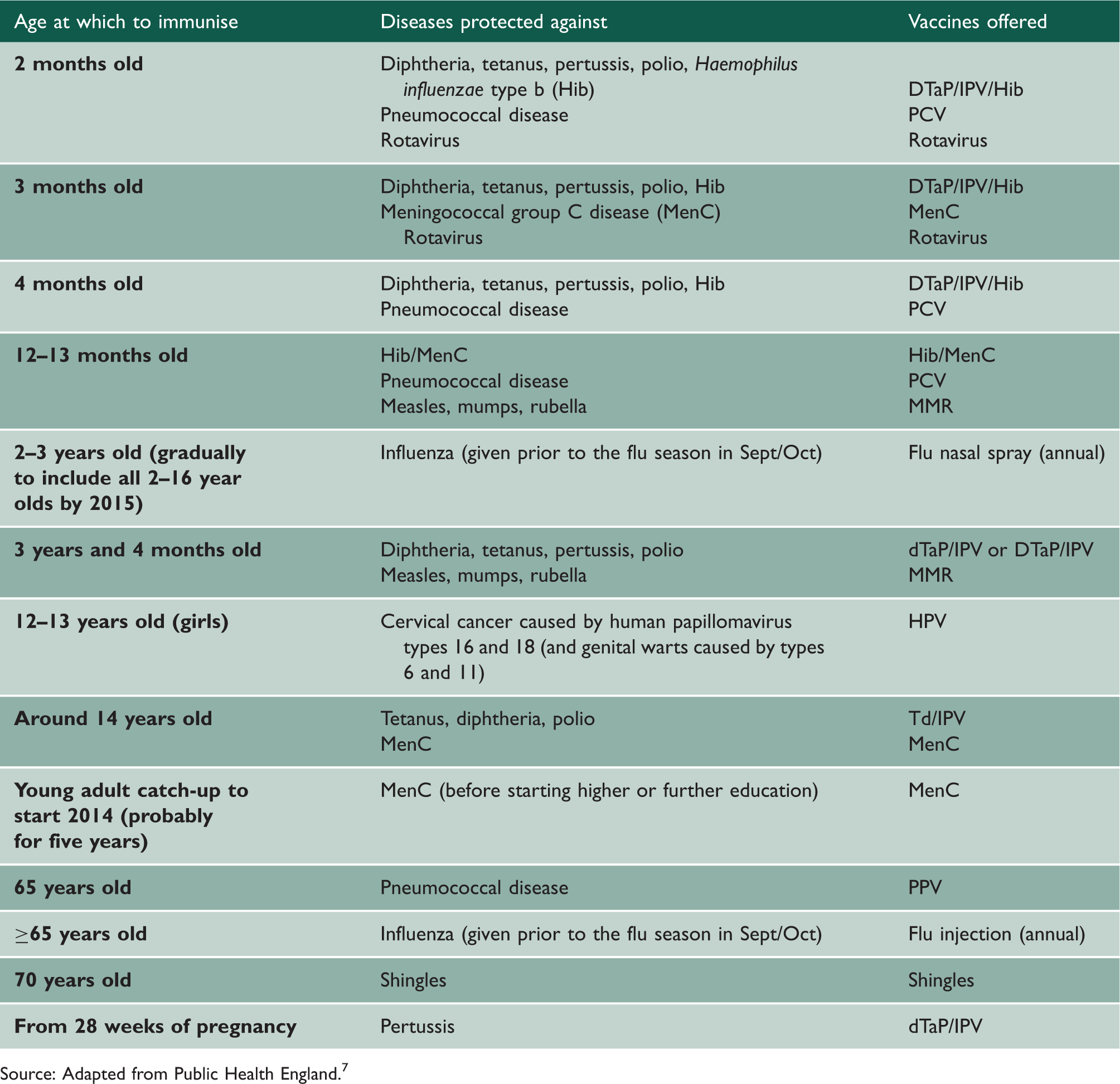
Figure 1 shows a timeline for the introduction of vaccines in the UK, and Table 1 outlines the complete routine UK immunisation schedule. For the 2013/2014 financial year (defined as running from April 2013 to March 2014) significant changes were made to the UK immunisation schedule. Here we describe the changes and outline the rationale behind these developments in vaccine policy.
Timeline for introduction of vaccines in the UK. The UK routine immunisation schedule 2013/2014. Source: Adapted from Public Health England.
7

Methods
Relevant literature was identified through a search of the online databases (MEDLINE, EMBASE and the GOV.UK online publications library) using a number of keywords (e.g. immunisation, vaccination, rotavirus, influenza, shingles, meningococcal C, pertussis, measles, mumps, rubella) either alone or in combination. A range of publications was retrieved, including research reports, editorials, letters and books, and a subset of 30 relevant articles and textbooks was used for our reference list. Information and evidence have been compiled from these to provide the reader with a concise and up-to-date review of developments in the UK vaccine policy.
New vaccines in the schedule
Rotavirus vaccine
Rotavirus is the most common cause of severe gastroenteritis among children under five years of age. 8 In the UK, rotavirus infection is estimated to result in 750,000 episodes of diarrhoea and 80,000 general practice (GP) consultations each year, 1 with 14,300 hospital admissions in children under five years. 2
Rotarix was added to the UK immunisation schedule from July 2013. The protective efficacy (>85%) of Rotarix against severe rotavirus gastroenteritis has been demonstrated in a number of large randomised controlled trials. 3 Post-licensure studies from the United States and Europe have demonstrated its effectiveness in real-world settings, with significant reductions in hospital admissions for rotavirus disease. 4 Safety is a primary concern of parents accepting a new vaccine that is administered to infants to prevent disease causing high morbidity yet very low mortality. An early rotavirus vaccine (RotaShield) used in the US was associated with a significant risk of intussusception among children who received it. 5 Large pre-licensure studies showed no association with intussusception, 3 but there is evidence from post-marketing surveillance that the two current rotavirus vaccines (Rotarix and RotaTeq) are associated with a slightly increased risk of intussusception. 6 However, the data suggest that the benefit from reduced cases of rotavirus gastroenteritis far outweighs the risks. 6 Nevertheless, these findings highlight the need for continued safety monitoring by countries introducing a rotavirus vaccine.
In November 2012, following the procurement of Rotarix at a cost-effective price, DH announced its decision to introduce the rotavirus vaccine into the national immunisation schedule from 2013. 7 Rotarix, a live-attenuated, orally administered two-dose vaccine, is recommended to be given at two and three months of age, via GP surgeries, alongside other primary immunisations scheduled to be given at that time (Table 1). Because of the possible link to intussusception, it is recommended that the first dose is received before 15 weeks of age and that the course should be completed by 24 weeks of age. 7 Information flyers and leaflets for parents have been produced to support the introduction of the rotavirus vaccine, and a Q&A factsheet has been developed for health professionals. These are available on the UK government’s immunisation webpage (www.gov.uk/government/collections/immunisation).
Preliminary findings from the first post-vaccination year in the UK suggest 88% vaccine uptake for a complete two-dose course, and a 67% reduction in laboratory-confirmed rotavirus infections compared with the pre-vaccination 10-year average for 2000–2013. 9
Influenza vaccine for children
Estimates of excess winter deaths potentially attributable to influenza in the last decade in England and Wales range from not determined (2005/2006 and 2006/2007) to 10,351 (2008/2009). 10 The risk of serious illness from influenza is highest amongst children under six months of age, older people, those with certain underlying health conditions and pregnant women. 7
Until recently, annual inactivated influenza vaccine given by intramuscular injection has been offered to individuals ≥65 years of age, and all those aged six months or older in clinical risk groups (chronic renal, heart, respiratory, liver or neurological disease; diabetes; immunosuppression; asplenia or dysfunction of the spleen; pregnancy). 7 In 2012, JCVI recommended that the routine annual flu immunisation programme be extended to all children aged 2–16 years from September 2013. It is expected to appreciably lower the public health impact of flu by directly averting a large number of cases of disease in children, and through lowering flu transmission in the community, indirectly preventing flu in individuals at high risk of serious illness from influenza, including unvaccinated younger children, people in clinical risk groups and older adults. This will substantially reduce flu-related illness, GP consultations, hospital admissions and deaths. 11 Mathematical models predict that the long-term incidence of influenza A and influenza B in the UK could decrease by 65–97% and 85–96%, respectively, in the overall population by vaccinating individuals aged 2–16 years. 12 Implementing an annual influenza immunisation programme for all children will inevitably have an impact on workforce capacity. As a result, full coverage of this age group will be phased in over several seasons. For 2013/2014 the programme was rolled out to all two and three year olds through GP, and local geographical pilots are being conducted among older children to identify the most effective delivery method for full roll out in 2015/2016. Long-term success of extending the programme to all children aged 2–16 years is likely to depend on adopting a multi-professional approach involving schools and teachers as well as healthcare professionals.
Fluenz, a live-attenuated, intranasal influenza vaccine has been recommended for use in this programme. This vaccine has been found to give greater protection against culture-confirmed and symptomatic influenza in children than the current inactivated influenza vaccine. 13 It has a good safety profile in children aged two years and older and has an established history of use in the US. 14 A single dose of Fluenz gives adequate protection in children. 15 Therefore, JCVI recommends that most children should be offered a single dose. 7 However, children in clinical risk groups aged two to less than nine years who have not received influenza vaccine before should be offered two doses, given at least four weeks apart. In a change to the previous recommendations, children aged 2–17 years in clinical risk groups will be offered the intranasal vaccine rather than the inactivated injectable influenza vaccine. Children aged six months to less than two years in clinical risk groups will continue to be offered the inactivated influenza vaccine. 7
Extending the flu immunisation programme to all children will have the added advantage of raising awareness of the benefits of flu immunisation amongst parents. DH anticipate that as flu immunisation for children becomes accepted as routine, this will have a positive impact on uptake rates for others who are eligible for flu immunisation, particularly those in clinical risk groups for whom the risk of serious complications is highest, and for whom coverage is presently only around 50%. 7 Parents of young children do not always perceive influenza to be a serious disease. 16 Therefore, a challenge for policymakers and health professionals will be to increase public awareness of the potential severity of influenza.
Shingles vaccine
Shingles (herpes zoster) is a debilitating condition caused by the reactivation of a latent varicella zoster virus (chickenpox) infection. It occurs most frequently and is more severe in older people. 17 It is estimated that over 50,000 people ≥70 years old are affected in the UK each year. Around one in 1000 people ≥70 years old who develop shingles die of the infection. 17
Zostavax, a vaccine to prevent shingles, was added to the UK immunisation schedule from September 2013. Zostavax, a live-attenuated vaccine, is given as a single dose by subcutaneous injection preferably in the deltoid region of the upper arm. It can be given at the same time (in a different body part) as seasonal influenza vaccine and at the same time as 23-valent pneumococcal polysaccharide vaccine in eligible patients (Table 1). It is recommended that the vaccine be routinely offered via GP surgeries, to people aged 70 years. There will also be a catch-up programme of limited duration for those aged 79 years. The efficacy of the vaccine declines with age and so it is not recommended for people ≥80 years old. 7 Information leaflets for patients have been produced to support the introduction of the shingles vaccine, and a factsheet has been developed for health professionals. These are available on the UK government’s immunisation webpage (www.gov.uk/government/collections/immunisation).
In a clinical trial, a single dose of Zostavax was assessed in 17,775 adults aged ≥70 years. The vaccine reduced the incidence of shingles by 38%, and the incidence of post-herpetic neuralgia by 66.8%. 18 The vaccine has a good safety profile, is well tolerated and is also immunogenic in individuals who have had a history of shingles prior to vaccination. 19 The impact of vaccination in the UK is predicted to be 11,000 fewer cases of shingles and 1500 fewer cases of post-herpetic neuralgia each year in England and Wales. 17
Changes to the schedule
Meningococcal C vaccine
The Meningococcal C (MenC) vaccination programme was introduced into the UK childhood immunisation programme in 1999 (Figure 1). Since then, invasive meningococcal disease (IMD) caused by meningococcal serogroup C has fallen by over 95% and cases are now at an extremely low level. 7 It is estimated that 13,000 cases of disease and 1300 deaths have been prevented. 20
From June 2013 significant changes were made to the MenC vaccination schedule based on advice from JCVI. This included the removal of the second dose at age four months from the routine schedule for infants, and the introduction of an adolescent booster dose at around 14 years of age.
The dose at four months has been removed from the schedule on the basis of evidence that a single dose of some varieties of MenC vaccine at three months of age is sufficiently immunogenic in infants to provide protection against serogroup C meningococcal disease in the first year of life until the first booster at 12–13 months of age when Hib (Haemophilus influenzae type b)/MenC vaccine is offered. 21 Of the three licensed MenC conjugate vaccines available in the UK, Meningitec, NeisVac-C and Menjugate Kit, only NeisVac-C and Menjugate Kit are suitable as a single dose for infants. 21 Additionally, recent evidence shows that immunity conferred by MenC immunisation in early childhood provides a short-term protective immune response. 22 Protection given by vaccination at 12 months wanes by the teenage years, but vaccination later in childhood provides higher levels of antibody that persist for longer. 23 Following consideration of the evidence, JCVI recommended the introduction of an adolescent booster to be given at the same time as the teenage tetanus, diphtheria and polio vaccine (Td/IPV) (Table 1), to extend protection into early adulthood. From August 2014, there will also be a catch-up programme of limited duration (probably five years) to offer the MenC vaccine to first time university entrants <25 years of age (i.e. those who will not have been vaccinated under the revised schedule at around age 14 years).
Pertussis vaccine in pregnancy
Before the introduction of pertussis immunisation in the 1950s, the average annual number of notifications exceeded 120,000 in the UK. 7 Severe complications and deaths occur most commonly in infants under six months of age.
A temporary pertussis vaccination programme for pregnant women was introduced in October 2012 in response to a significant rise in the number of pertussis cases across the UK. 24 The highest rates were in infants aged under three months, including several deaths among young babies. 24 In May 2013, DH announced this temporary programme was to continue until further notice following advice from JCVI based on preliminary data on the evaluation of the immunisation programme, including immunisation coverage in pregnant women and surveillance data of the impact of the programme on disease in infants and on the safety of the vaccine in pregnant women. The key aim of the programme is to protect vulnerable infants from birth in the first months of life, before they can be fully protected by routine infant immunisation. DH recommends vaccination of pregnant women between 28 and 38 weeks’ gestation. 7 Immunisation of women in the later stages of pregnancy has been shown to boost pertussis antibodies, which may then be passed from mother to baby and so protect the infant until given the vaccine at two months of age. 24 Pertussis vaccine is only available in combination with other vaccines (diphtheria, tetanus, polio) and DH advises that the combination vaccine Repevax (diphtheria, tetanus, pertussis and polio vaccine (dTaP/IPV)) be used as a pertussis booster in pregnant women. 7 A challenge anticipated for this programme was the possible reluctance among pregnant women to receive a vaccine, as this is contrary to the usual advice about avoiding medication in pregnancy. Indeed, the average monthly pertussis vaccine coverage for pregnant women between October 2012 and September 2013 was only 53.9%. 25 However, there is no evidence of risk from vaccinating pregnant women with inactivated viral or bacterial vaccines or toxoids such as those included in Repevax. 7 Information flyers and leaflets for pregnant women and health professionals have been produced to communicate this message.
The pertussis immunisation in pregnancy programme in England has shown high levels of protection against pertussis in babies born to vaccinated mothers. 26 For the first nine months of 2013 compared with the same period in 2012, there was a 78% reduction in confirmed cases and a 68% fall in hospitalisations in infants younger than three months. 26
Catch-up campaigns
Measles, mumps and rubella vaccine
In 1998, the Lancet published a study by Wakefield et al. of a small case series of children with autism suggesting a link with measles, mumps and rubella vaccine (MMR). 27 This attracted considerable negative publicity for MMR in the mainstream media, and despite good scientific evidence against such an association, 28 adverse media coverage was sustained over the next few years. Although the Wakefield paper was eventually discredited and retracted by the Lancet, 29 the impact was a dramatic reduction in MMR vaccine coverage. 30 Whilst uptake of MMR vaccine has now improved markedly, large numbers of unvaccinated children in the cohorts most affected by the decline in coverage have reached their teenage years, when the risk of transmission increases. In April 2013, in response to large outbreaks of measles in south Wales and other parts of the UK, DH announced a national MMR catch-up campaign. The campaign specifically targeted unvaccinated children aged 10–16 years with the aim of protecting them and preventing further outbreaks in secondary schools, and therefore onward transmission to young infants and other vulnerable groups. The strategy included raising demand through targeted communications, identification of unvaccinated children through primary care and child health registers and provision of vaccination in primary care or other settings such as schools. By August 2013, approximately 60,000 previously unvaccinated 10–16 year olds had received one dose of MMR and the number of measles cases was falling. 20
Discussion
Immunisation is the most important way of protecting individuals and the population from vaccine preventable infectious diseases. The UK immunisation schedule is continuously being reviewed and revised as new vaccines become available, in response to specific outbreaks or as evidence accumulates about their impact. For all vaccine-preventable infections in the UK, enhanced national surveillance is in place to monitor vaccine coverage, the impact of the vaccination programmes on burden of disease and vaccine safety.
Communication is the key to successful implementation of a new vaccine policy, in particular to allay public fears and mitigate potential media scares. Multiple routes are employed so that health professionals and the public understand the change and the actions that they need to take to facilitate its implementation. Health professionals can keep up to date with UK immunisation changes and the rationale behind them by consulting the online version of the Green Book 7 and other resources available on the UK government’s immunisation webpage (www.gov.uk/government/collections/immunisation). For the public, promotional resources include: leaflets; fact sheets; press, television, and radio advertisements; videos and Internet materials, including ‘Q and A’ formats and frequently asked questions (FAQs). A multi-professional approach involving policymakers, healthcare professionals as well as schools and teachers for child and adolescent schedules, is vital for the success of vaccination programmes in the UK. It is especially important that they remain enthusiastic and committed to delivering a high-quality immunisation service through ongoing changes in organisational and operational structures set out in the recent national health reforms implemented from April 2013.