
Abstract
Lesson
Fungi of the genus Phoma are common plant pathogens and saprophytes and are rarely pathogenic to animals.
Case report
We report a rare case of contact lens-related keratitis where a Phoma fungus was isolated from the corneal scrape.
A 79-year-old lady presented to eye casualty with a two-day history of redness in the right eye. She used daily disposable soft contact lenses on a regular basis for refractive correction of her myopia.
Her visual acuity was 6/12 on the right and 6/9 on the left. The bulbar conjunctiva on the right eye was injected. There was an epithelial defect on the right cornea measuring 1 mm in diameter at 2:00, just off the pupillary border. There were a few fine keratic precipitates on the cornea around the area of abrasion. Occasional cells were seen in the anterior chamber. The epithelial defect healed with topical ofloxacin but she returned four weeks later with a corneal infiltrate 1 × 1 mm with overlying epithelial defect 1.8 × 1.7 mm (Figure 1). Her ulcer failed to respond to empirical treatment with topical ofloxacin and econazole and the defect increased to 3.5 × 3.5 mm with a central abscess. A corneal scrape was negative on Gram staining and culture grew a coagulase-negative Staphylococcus, considered to be a contaminant. Subsequently, she underwent a corneal biopsy and samples were sent for culture and histology.
Right eye corneal infiltrate and the non-healing epithelial defect.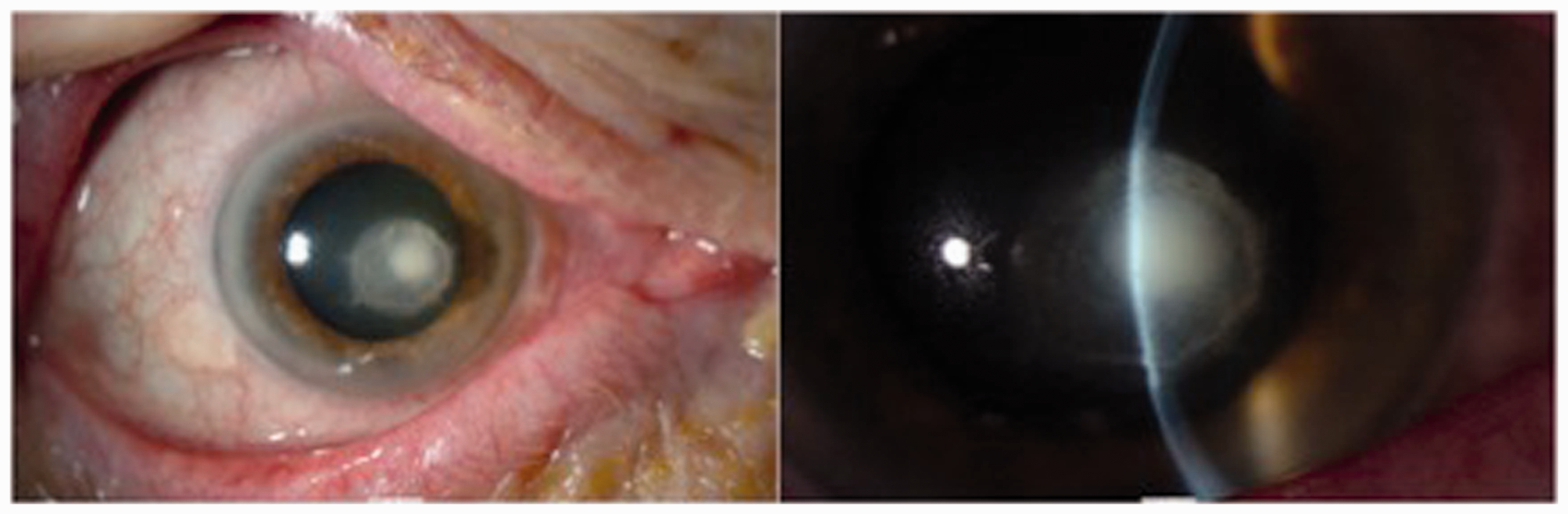
Fungal filaments were identified on histology (Figure 2). The corneal biopsy grew a mould fungus after five days of incubation at 30°C. The isolate was sent to the Health Protection Agency Mycology Reference Laboratory (MRL), Bristol where the fungus was identified as a Phoma species on morphological criteria. The DNA was sequenced and compared with the European Molecular Biology Laboratory database. This confirmed its membership of the Phoma genus but failed to give a close match with any Phoma species in the database, indicating a novel species. Sensitivity testing was performed by the MRL using the NCCLS M38A protocol and the isolate was found to be sensitive to amphotericin B (MIC 1.0 mg/L), itraconazole (MIC 0.5 mg/L), econazole (0.25 mg/L) and voriconazole (0.125 mg/L).
Fungal filaments on histology.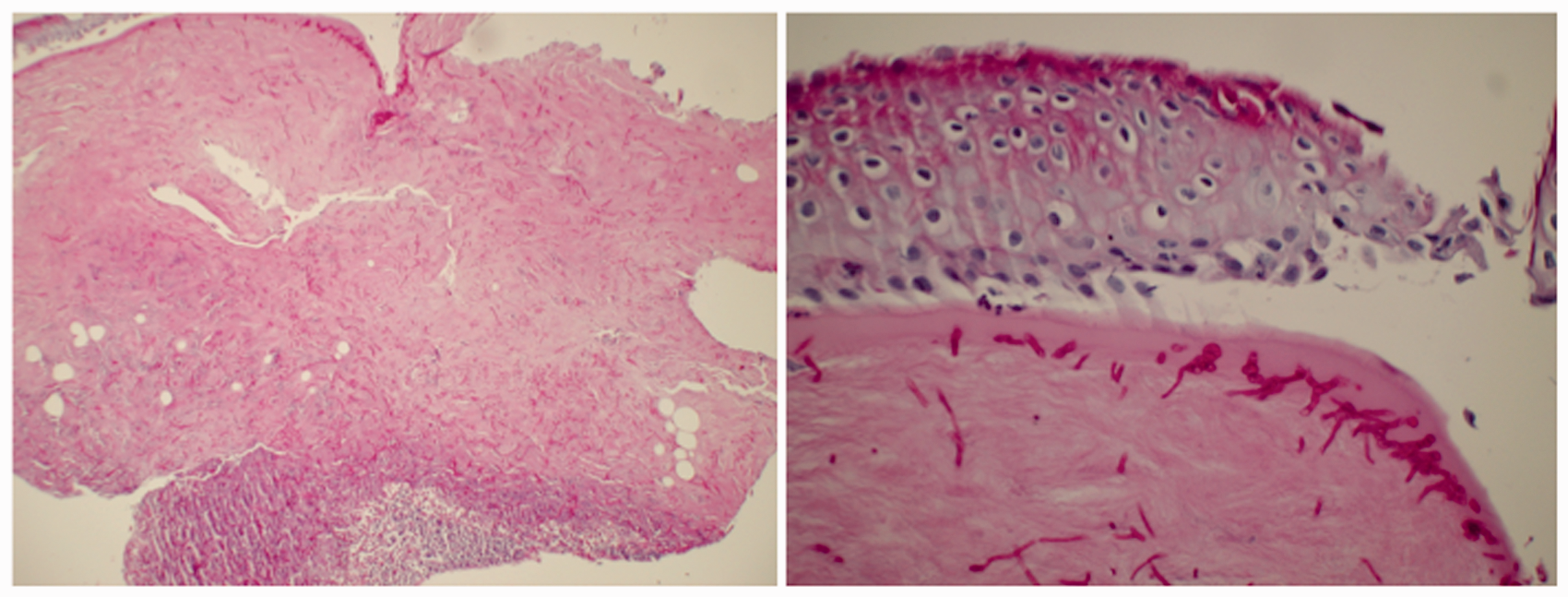
She was started on systemic itraconazole 100 mg/day and she was treated with amphotericin eye drops. While being on treatment, the patient’s cornea perforated requiring keratoplasty. Postoperatively, the patient was on oral itraconazole, topical dexamethasone and topical cyclosporine 0.5% qds, and chloramphenicol 0.5% qds. The inflammation subsided over the next few weeks. Visual acuity improved from hand movements to 6/18 corrected.
Discussion
There are a number of predisposing factors for fungal keratitis. They include trauma, contact lens wear, corneal surface disorders, dry eye, exposure keratitis and bullous keratopathy.1–3 There have been reported cases of fungal keratitis following refractive surgery. 4
In a recent study conducted in the UK, it was found that the most common aetiological agents of fungal keratitis came from the genus Candida (57.5% cases of fungal keratitis) and the most common filamentary fungus isolates were of the genus Aspergillus (17.5% of cases 5 ). However, studies in the developing countries of the tropics have shown that filamentous fungi of the Fusarium species and Aspergillus species are the major aetiological agents of fungal keratitis. 3
A filamentous fungus of the genus Phoma caused infection in this case. Phoma species are common plant pathogens and soil saprophytes. The first human Phoma infection (cutaneous lesion of the leg) was described by Bakerspigel. 6 Most reported human Phoma infections occur in immunocompromised individuals and affect the skin and subcutaneous tissue. 7 To our knowledge, there is only one other detailed reported case of keratitis due to Phoma infection and this was associated with ocular trauma. 1 Punithlingam 8 published a short communication with no clinical history and Carmichael et al. 9 published a case series of corneal ulcers, one of which was caused by Phoma eupyrena.
Histopathological examination, microbiologic culture and DNA sequencing were used to diagnose the infection in this patient. Phoma fungal infections can be successfully treated with antifungal agents such as itraconazole, ketaconazole, voriconazole and amphotericinB. 10
Topical steroids can aggravate fungal keratitis and our current strategy is to use systemic and topical cyclosporine (instead of topical steroids) in such cases, in order to minimise the risk of graft rejection while preserving the phagocytic function of mononuclear cells.
There are previous reports of Phoma fungus-related keratitis.11,12 However, our report gives a detailed description of the investigations including microbiology and histology slides and the outcome of intensive treatment. There are also a couple of reports in literature about Phoma isolates in asymptomatic contact lens wearers.11,12
Fungal infection should be considered in the differential diagnosis of cases of infective keratitis, especially when unresponsive to standard treatment. Treatment should be tailored according to individual patient characteristics and prolonged treatment and close monitoring is usually required in order to achieve the best outcome. A multidisciplinary team approach involving the ophthalmologist, microbiologist and histopathologist may help to deliver the best care for these patients.