
Abstract
Lesson
There is an association between inflammatory bursitis with rice body formation and use of bioabsorbable suture anchors.
A 60-year-old man underwent arthroscopic repair for a supraspinatus tear of his left shoulder. A single 5.5-mm poly-L-lactic acid anchor (Spiralok™, DePuy Mitek) was threaded with two strands of #2 (Orthocord™) suture. His medical history does not include rheumatoid arthritis, tuberculosis or previous allergies.
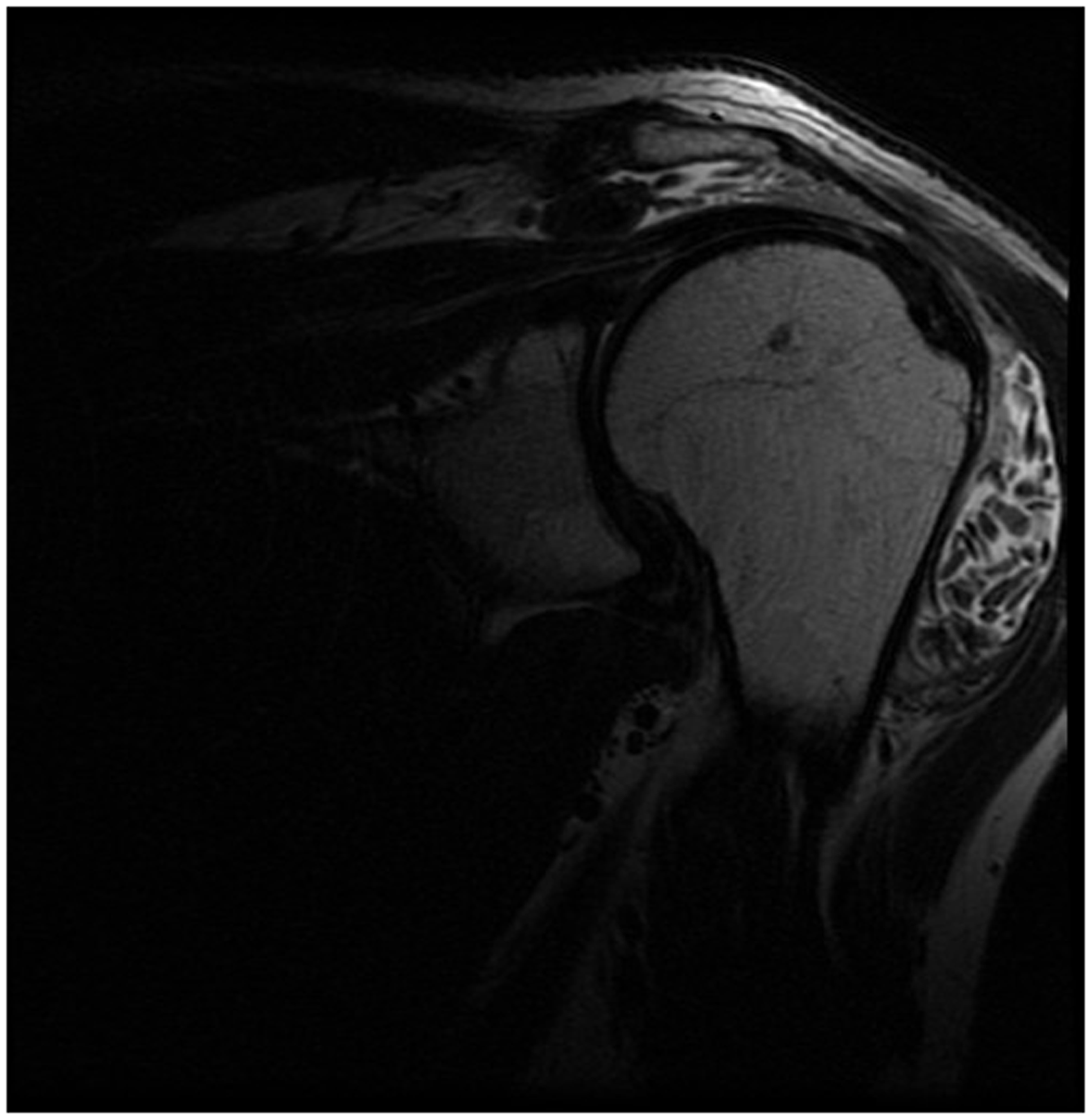
At three-month follow-up, the patient reported a constant low-grade dull left shoulder ache. At nine months, the pain had worsened. He described ‘crunching sensation’ with shoulder movement. Physical examination revealed a swelling over the anterior aspect of the left shoulder. His range of movements was as follows: external rotation to 50°, elevation to 140°, abduction to 95° and internal rotation to the third lumbar vertebra. Movement was painful and produced crepitus. The visual analogue pain score was 8/10. C-reactive protein, leukocyte and erythrocyte sedimentation levels were normal. Plain radiographs of the shoulder showed no abnormality. A magnetic resonance imaging showed fluid distended subacromial and subdeltoid bursae, containing numerous small bodies of intermediate density on proton density sequences (Figures 1 and 2).
T2-weighted STIR sequence magnetic resonance image, showing multiple nodules clearly delineated within the fluid distended subdeltoid bursa. Coronal T2-weighted magnetic resonance image showing extensive synovitis and rice bodies.
The patient underwent a left shoulder arthroscopic debridement, evacuation of loose bodies, poly-L-lactic acid anchor and suture removal. Intra-operatively, hundreds of grain-like loose bodies filled the subacromial and subdeltoid bursae. The supraspinatus repair was partially disrupted. No macroscopic evidence of infection could be seen. The poly-L-lactic acid anchor showed no fragmentation. No organisms were grown from operative specimens (early and late cultures).
Microscopically, the loose bodies were found to be inflammatory rice bodies, with an inner amorphous core of acidophilic material, surrounded by a plasma and lymphocytic cell infiltrate, with an outer rim of fibrin-like material. No foreign body granulomas or polymer debris were seen microscopically. Allergen testing using the British Contact Dermatitis Society standard extensive series, as well as patch testing to both anchor and suture material were negative. Post-operatively, the patient’s pain improved almost immediately. Two months later, a magnetic resonance imaging scan showed complete resolution of the rice bodies, with mild residual subacromial and subdeltoid bursitis.
The patient regained a full range of shoulder movement but continued to complain of pain and weakness with overhead activity. Six months post-arthroscopic debridement, a revision arthroscopic rotator cuff repair was performed using a 5.5-mm Titanium anchor loaded with suture (Orthocord™). At 12-month follow-up, the patient was pain-free. He remained asymptomatic at two years’ post-operation.
Discussion
Bioabsorbable suture anchors are playing an increasing role in attaching tendons and ligaments to bone. Their properties minimise the problems associated with anchor loosening, migration, interference/artefacts on imaging as well as reducing the need for later implant removal. 1
Poly-L-lactic acid anchors are made of the polymerised levorotatory form of lactic acid. Polymer degradation releases lactic acid, which undergoes oxidation to pyruvate. Although poly-L-lactic acid anchor implants are labeled as ‘non-immunogenic’, their rapid degradation is associated with a foreign body immune response. 2 This case report illustrates the use of poly-L-lactic acid suture anchor in a rotator cuff repair that was complicated by severe inflammatory synovitis and rice body formation.
Poly-L-lactic acid anchor polymers are known to cause an immune reaction in the latter stages due to biodegradation. 2 As part of this adverse immune response, they can lead to osteolysis, sinus tract formation, chondral defects, synovitis and intraosseous granulomas.1,2 A study by Kim et al. 3 which looked at 209 patients found that cysts were observed in 97 instances (46.4%). There were 41 grade 1 cases (19.6%), 16 grade 2 (7.7%), 22 grade 3 (10.5%), and 18 grade 4 (8.6%) cases of osteolysis. Several publications suggest that poly-L-lactic acid anchor polymers may have immune and complement activating potential. Mastrokalos et al. 4 reported a systemic allergic reaction to poly-L-lactic acid anchor interference screws, used in an anterior cruciate ligament reconstruction. In addition to the adverse reactions, a study by Wright et al. 5 concludes from an in vitro study that FiberWire-anchor construct is significantly weaker when bioabsorbable anchors are used instead of metal anchors.
Rice body formation is a rare complication of chronic subacromial and subdeltoid bursitis, usually associated with rheumatoid arthritis, sero-negative inflammatory arthritis, septic arthritis and tuberculous arthritis.6,7 Use of poly-L-lactic acid anchor implants resulting in subdeltoid bursitis with rice body formation has yet to be reported in English literature.
This case study reports a patient who developed a non-foreign body inflammatory synovitis related to the poly-L-lactic acid anchor. This is illustrated by:
The early onset of clinical symptoms; The absence of poly-L-lactic acid anchor implant fragmentation; The presence of inflammatory rice bodies; The absence of microscopic evidence of a foreign body reaction.
The absence of adverse reaction using the same suture material for the rotator cuff repair excludes the suture material as a contributory factor for the initial inflammatory response.
Conclusion
Bioabsorbable suture anchors, such as poly-L-lactic acid anchors, used in rotator cuff repairs can induce an inflammatory synovitis with rice body formation. As part of our management, we undertook arthroscopic debridement implant removal.