
Abstract
Summary
Objectives
Varicella and Herpes Zoster are common infectious diseases. Various studies have estimated rates of infection for both manifestations of these infections; however rates of hospital admissions across the country have not previously been described. This paper presents data on hospital admissions in England for Varicella and Herpes Zoster from 2001/2002 to 2010/2011.
Design
Time trends study of all hospital admissions for Varicella and Herpes Zoster from 2001/2002 to 2010/2011 in England.
Setting
Hospital admissions across England from 2001/2002 to 2010/2011.
Participants
We included all patients admitted to hospital from 2001/2002 to 2010/2011 diagnosed with Varicella and Zoster according to the International Classification of Diseases version 10 (ICD-10).
Main outcome measures
The main outcome measures were admission rates by year and diagnosis and age-specific admission rates for Varicella and Zoster from 2001/2002 to 2010/2011.
Methods
We analysed data from Hospital Episode Statistics which include patient characteristics such as age which was used here in order to standardise rates to the relevant population. We also used mid-year population estimates from the Office for National Statistics for standardisation purposes. All analyses were conducted using Stata v12.0.
Results
The hospital admission rate for Varicella cases has risen by 1.8% over the 10-year study period. While the overall admission rates for Herpes Zoster have decreased by 4% from 2001/2002 levels. The vast majority of Varicella and Zoster admissions were not associated with any complications.
Conclusion
The introduction of Herpes Zoster vaccine is anticipated to decrease hospital admissions in older age groups further. A repeat of this study after a further period of time would help to evaluate the impact of the introduction of Herpes Zoster vaccine in England on hospital admissions.
Introduction
Varicella and Herpes Zoster are common infectious diseases seen throughout England. Various studies have estimated rates of infection for both manifestations of these infections; however, rates of hospital admissions across the country have not previously been described. This paper presents data on hospital admissions in England for Varicella and Herpes Zoster over a 10-year period.
Varicella Zoster Virus is responsible for two diseases: Varicella (Chicken Pox) which occurs mainly in childhood and Herpes Zoster (Shingles) which occurs mainly in older adults. A reactivation of the patient’s Varicella virus causes Herpes Zoster (Shingles). Herpes Zoster is more common in the elderly but can affect children and immunosuppressed individuals of any age. 1
Chickenpox and shingles are not notifiable diseases but Varicella Zoster is a causative organism notifiable under the Health Protection (Notification) Regulations 2010 in England and Wales. The estimated incidence of Varicella in England and Wales is approximately 1290 cases per 100,000 person-years 2 while the estimated incidence of Herpes Zoster infection is approximately 880 to 960 cases per 100,000 people per year for those aged 70 to 79 years. 3
Preventive vaccination is available for both manifestations of Varicella Zoster virus. However, vaccination for prevention of Varicella infection is only recommended in England in specific circumstances. A live attenuated vaccine (Varivax) is available for non-immune healthcare workers and also recommended for healthy susceptible close household contacts of immune-compromised patients. 1 In September 2013, a vaccine for Herpes Zoster for older people between 70 and 79 years old was introduced in England. 4 The aim of the introduction of the vaccination is to reduce morbidity and mortality from Herpes Zoster infections in this group; information from studies of GP consultations in England and Wales indicates that more than 50,000 cases of Herpes Zoster occur annually in older people aged 70 years and above. 4
This paper can provide valuable information about the hospital burden of the disease to inform healthcare planners, clinicians and commissioners before the introduction of routine vaccination for Herpes Zoster. We will examine trends in the rates of hospital admissions and the conditions where Varicella and Herpes Zoster were mentioned as co-morbidity in England during the period 2001/2002 to 2010/2011.
Methods
Data for this study came from Hospital Episode Statistics (HES). 5 HES is an administrative database which records episodes of care in hospital funded by the National Health Service (NHS) in England. HES data use the International Classification of Diseases version 10 (ICD-10) 6 to code up to 20 diagnoses present in patients, both as a ‘primary’ (or reason for admission) and ‘secondary’ (or comorbid) diagnoses. We included both primary and secondary diagnoses and used the ICD codes B01 for Zoster and B02 for Varicella. HES data also include patient characteristics, including demographic information such as age which was used here in order to standardise rates to the relevant population. During hospital stays, patients may be under the care of different consultants, each of which is known as a ‘finished consultant episode’. These were aggregated into hospital spells (i.e. admissions to hospital) using a method recommended by the NHS Information Centre, based on dates of admission and discharge as well as patient identifiers. 7 Mid-year population estimates came from the Office for National Statistics 8 and the information was used for standardisation. All analyses were conducted using Stata v12.0.
Results
Admission rate per million population (number) for Varicella and Zoster admissions by year and diagnosis, 2001/2002–2010/2011.
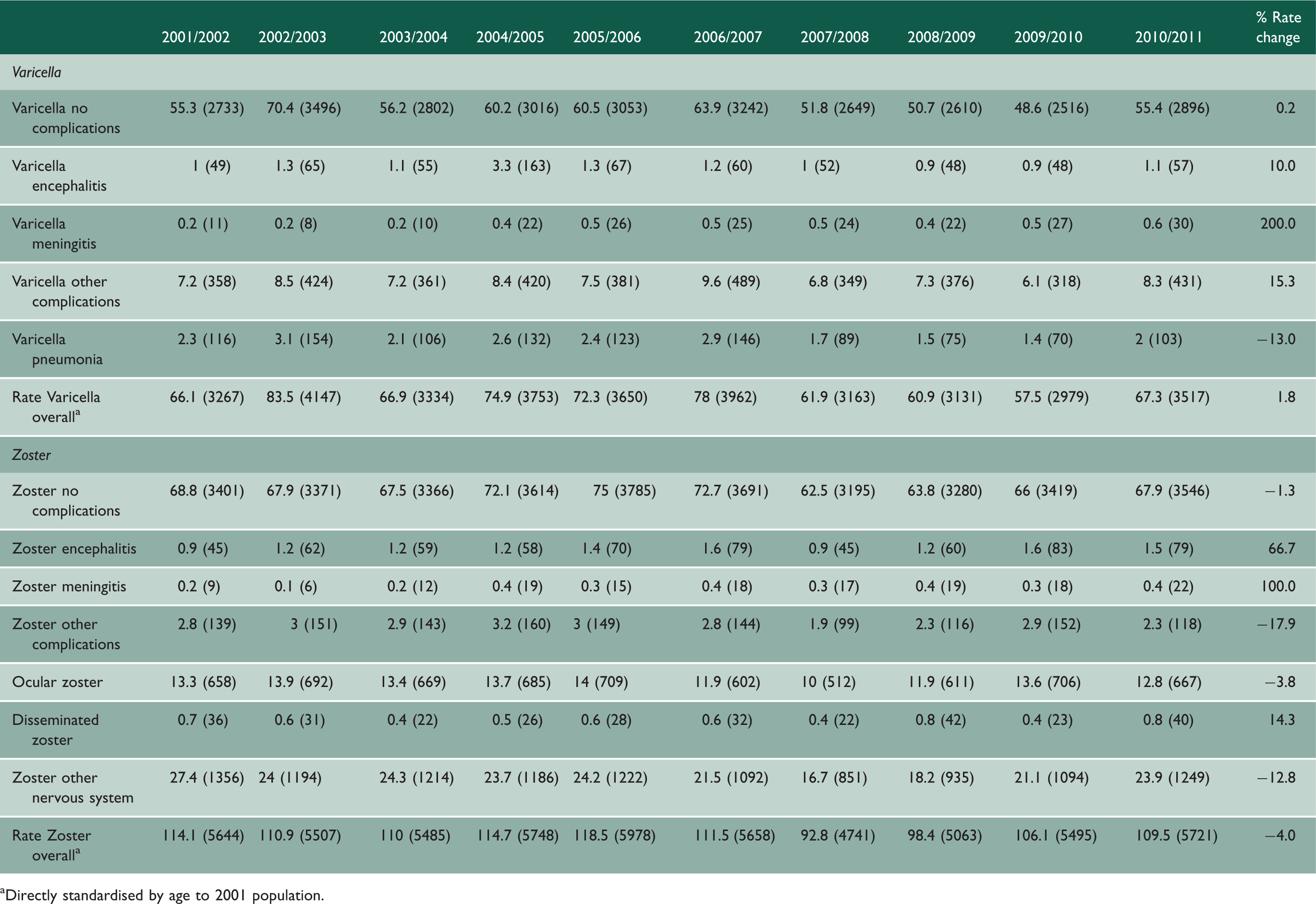
Directly standardised by age to 2001 population.
The vast majority of Varicella admissions were not associated with any complications (82% in the year 2010/2011). Over the 10-year time period analysed, there was a 15.3% increase in admitted Varicella cases with complications with a 10% increase in Varicella encephalitis. Varicella meningitis as a complication has increased from 0.2 per million population in 2001/2002 to 0.6 per million population in 2010/2011 which represents a 200% increase from 2001/2002 levels. There was a 13% decrease in Varicella pneumonia but rates of cases with Varicella pneumonia have fluctuated over the time period. However, other than a steady increase in the rate of Varicella meningitis the rate for other complications of Varicella infections has fluctuated over time.
In 2010/2011, there were 5721 hospital admissions of Herpes Zoster virus cases compared to 5644 in 2001/2002. The overall admission rates for Herpes Zoster have declined slightly from 114.1 per million population in 2001/2002 to 109.5 per million in 2010/2011. This represents a 4% decrease from 2001/2002 baseline levels. The rates were fluctuating during this period. The vast majority of zoster admissions were not associated with any complications but Herpes Zoster associated meningitis has increased from 0.2 per million population in 2001/2002 to 0.4 per million population in 2010/2011 which represents a 100% increase from 2001/2002 levels. Also, there was a 66.7% increase in Herpes Zoster encephalitis cases and a 14% increase in disseminated Herpes Zoster in the same period. However, there was a 17.9% decrease in other Herpes Zoster complications.
Age group specific admission rates per million population (number) for Varicella and Zoster admissions, 2001/2002–2010/2011.

Directly standardised by age to 2001 population.
In 2010/2011, there was approximately a 30% rise in hospital admissions for patients over 60 years old compared to 2001/2002 levels; however, there was a 30% decrease in hospital admissions in the 15–59 year age group in the same period.
Generally, the admission rates for Herpes Zoster were decreasing in 2010/2011 compared to 2001/2002. For that period, there was 13.3%, 14.6% and 7.2% decrease in hospital admissions in the <15 years, 60–74 and over 75 years age groups, respectively. Over the 10-year period, there was a marked difference in rates of admissions for Herpes Zoster between those recorded in a peak year of 2005/2006 (5978 admissions, a rate of 118.5 admissions per million of the population) and those recorded in the year 2007/2008 (4741 admissions, a rate of 92.8 admissions per million of the population).
Discussion
Main findings of this study
This study found that rates and numbers of admissions for Varicella have remained relatively steady over the last 10 years although there was a slight increase in 2002/2003 and a fall in 2007/2008. The overall hospital admission rate for Herpes Zoster has fallen over the study period by 4%. However, for both infections, the rate of complications has increased which may lead to longer hospital admissions and increased morbidity and mortality.
The age distribution of Varicella and Herpes Zoster admissions is in line with the epidemiology of their associated illnesses with highest rates of Varicella admission in the young (Varicella is mainly a childhood illness) and the older age group. 9 Herpes Zoster rates of admission were steady in working age adults, but falling slightly in other age groups.
The increase over time in rates of complications such as Varicella and Herpes Zoster meningitis was also reported in a study based in three Italian Paediatric Hospitals over a four- to five-year period. 10 The findings revealed that 32% of hospital admissions for Varicella had neurological complications (particularly in older children) and that this was linked to a longer hospital stay. The Italian study was able to provide useful background information before the introduction of Measles, Mumps, Rubella and Varicella vaccination into the Italian routine childhood immunisation schedule.
To our knowledge, this is the first study looking at trends of hospital admissions of Varicella and Herpes Zoster across the whole of England. One study looked at admission rates for Varicella to an Infectious Diseases Unit over a 26-year period (reviewing admissions in three five-year time periods). 11 This study noted that over time there was an increase in the mean age of adult admissions. The study reported that smokers were six times more likely to develop pneumonitis than non-smokers. Our study did not have access to pre-admission or social factors influencing outcome or complication rates which would have been interesting to review. The Infectious Diseases Unit study noted that males in all age groups showed a trend towards more severe disease. A breakdown of disease complications by gender for this study would have allowed for more comparison with previously published findings.
Limitation of this study
The main limitation of this study is the weakness inherent in missing, inaccurate or incomplete routine data, such as incorrect hospital diagnoses and coding. Since the introduction of diagnosis base payment however there has been an improvement in the data quality. There was no examination of multiple admissions or re-admission rates for patients with these infections which could have enhanced the analysis.
Implications for policy and clinicians
Hospital admission rates for both Varicella and Herpes Zoster have stayed reasonably steady over the study period. The Joint Committee for Vaccination and Immunisation has agreed to roll out Herpes Zoster vaccination for 70–79 year olds from September 2013. It is important to monitor trends in diseases especially after introducing the Herpes Zoster vaccine. This study allows for a baseline in interpretation of the effectiveness of the vaccine in prevention of hospital admissions related to Herpes Zoster and the associated rates of complications.
Unanswered questions and future research
The main strength of this study is that it includes all NHS hospital admissions in England rather than for individual units or groups of hospitals as in the previously published literature. There is a need for more detailed work in the future to consider the factors which contribute to infection and/or complications of infection. A repeat of this study over time following the introduction of Herpes Zoster vaccination into the routine immunisation schedule would provide valuable information about its efficacy in preventing complications that lead to hospital admission.
Conclusions
The rise and fall in rates of admission to hospital over the 10-year period of the study is not unexpected given that there are peaks and troughs in rates of infection with a seasonal variability. It is important to recognise these variations in rates when commissioning inpatient services for infectious diseases related admissions.
The hospital burden of Varicella has slightly increased during the 10 years of the study period in England while Herpes Zoster admissions have decreased slightly. The introduction of Herpes Zoster vaccine is anticipated to decrease hospital admissions in older age groups further. A repeat of this study after a further period of time would help to evaluate the impact of the introduction of Herpes Zoster vaccine in England on hospital admissions.