Abstract
Lesson
This case offers a starting point for a literature review on peritoneal ultrafiltration in refractory heart failure.
Case report
In July 2010, a 64-year-old man was referred to our unit because of refractory congestive heart failure (HF). He had a history of chronic bronchitis, interstitial lung disease and arterial hypertension. In 1990, he had a large inferior myocardial infarction complicated by left ventricular aneurysm and HF, NYHA class III. In 1991, he underwent ventricular aneurysmectomy and mitral pericardial annuloplasty, complicated by mediastinitis. In 2004, he underwent restrictive mitral annuloplasty and in 2005 a cardioverter-defibrillator was implanted. The patient was neither eligible for heart transplantation nor for left ventricular assist device insertion. In August 2010, he presented worsening of dyspnea (NYHA class IV) and his Charlson's comorbidity index was 8 (1-year survival of 63%). His treatment was: frusemide 125 mg/day alternate to 250 mg/day, aldactone 100 mg/day, digoxin 0.125 mg 5 days/week, ramipril 2.5 mg/day and warfarin. In August 2010, he had severe peripheral oedema, his body weight was 85.7 kg and blood pressure 85/60 mmHg. Blood tests showed: creatinine 1.58 mg/dL, estimated GFR (eGFR) (four variables MDRD formula IDMS) 44 mL/min/1.73 m2, urea 25 mg/dL, sodium 130 mEq/L, potassium 3.08 mEq/L, calcium 8.9 mg/dL, haemoglobin 9.8 g/dL, albumin 3.8 g/dL, alanine transaminase (ALT) 5 IU/L, gamma glutamyl transpeptidase (GGT) 88 IU/L. Chest X-rays showed cardiomegaly, peribronchial thickening with initial perihilar consolidations and bilateral pleural effusion. At echocardiography, left atrium was enlarged (30 cm2) with severe mitral valve insufficiency and left ventricular enlargement (end diastolic volume 248 mL, end diastolic diameter 68 mm) with diffuse hypokinesis (ejection fraction 33%), while right atrium and ventriculum were normal. Estimated systolic pulmonary arterial pressure (sPAP) was 52 mmHg. Despite medical therapy, he had recurrent worsening of dyspnea and oliguria. High doses of IV frusemide were administered, followed by hypokalemia (3 mEq/L) and severe hyponatremia (113 mEq/L) without significant increase in diuresis. From March 2009 to August 2010 he was hospitalized 10 times and he spent 100 days in cardiac intensive care unit (CICU). At this stage of congestive refractory HF, according to both European Society of Cardiology and American College of Cardiology Foundation/American Heart Association guidelines (class IIa, level of evidence B),1,2 ultrafiltration is indicated. In August 2010, patient started home peritoneal UF. Daily therapeutic schedule included one icodextrin exchange (1 L 7.5%, 10 h dwell). Occasionally, 3.86% dextrose exchange (1 L, 2 h dwell) was administered according to clinical indications (dyspnea, body weight, ultrafiltration volume, diuresis). In November 2010, three months later, his therapy was unchanged except for withdrawal of ramipril and administration of bisoprolol 1.25 mg/die and darbepoetin alfa 60 mcg SC once weekly. His body weight was stably 81 kg and blood pressure 120/70 mmHg. He still had peripheral oedema. Blood tests were: serum creatinine 1.44 mg/dL, eGFR (MDRD) 49 mL/min/1.73 m2, serum urea 29 mg/dL, sodium 134 mEq/L, potassium 3.42 mEq/L, calcium 9.2 mg/dL, haemoglobin 11.3 g/dL, albumin 3.5 g/dL, ALT 17 IU/L and GGT 90UI/L. Chest X-rays showed reduction of interstitial oedema signs and only right pleural effusion. Echocardiographic data were unchanged except for decrease of sPAP (40 mmHg). The patient had no complications related to peritoneal UF. From August 2010 to January 2012 he was admitted twice to hospital for worsening dyspnea and spent in CICU only 10 days. In April 2011, he underwent biological mitral implantation with poor results and in January 2012, after further deterioration of cardiac function and acute worsening of HF, he died. In the 17 months following peritoneal UF, our patient improved his life quality, returning to a more normal life style.
Discussion
HF is a serious and common disease affecting 1–10% of the adult population in developed countries. In patients with HF, neurohormonal activation leads to fluid overload that may be treated by means of high doses of frusemide unless hyponatremia and diuretic resistance occur. End-stage congestive HF can become refractory to medical treatment even in patients with normal renal function. These patients require frequent hospitalizations for dyspnea, orthopnea, paroxysmal nocturnal dyspnea, electrolyte imbalance and oliguria. In some cases of refractory HF, UF is needed. While extracorporeal UF is commonly used as emergency treatment, peritoneal UF should be taken into account for long-term management of selected HF population.
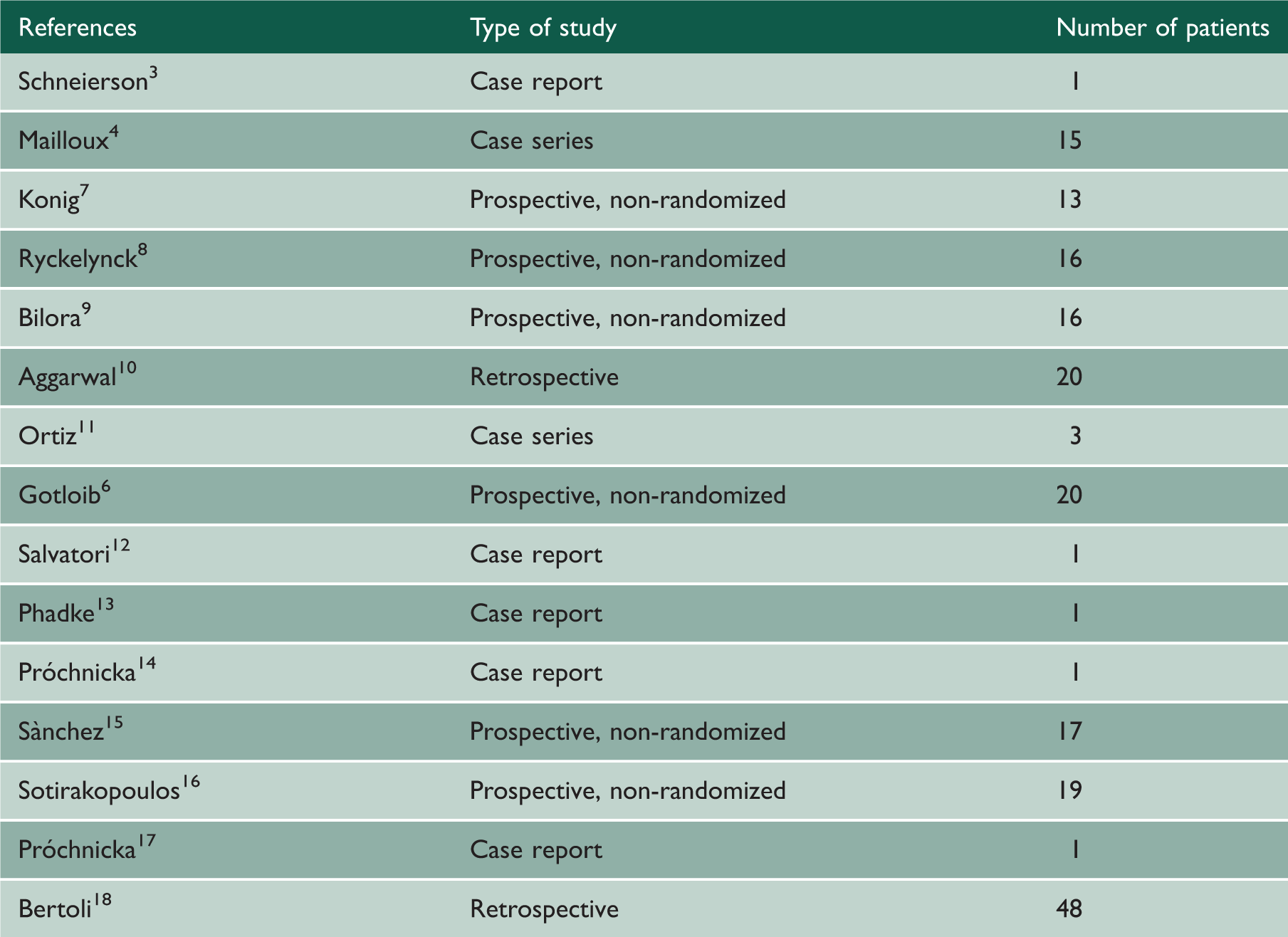
Schneierson 3 was the first to report the successful use of peritoneal UF in HF. Mailloux et al. 4 concluded that peritoneal UF can be useful in HF patients under selected clinical conditions: concomitant renal disease, electrolyte imbalance, preparation for heart surgery and rapid deterioration of a previously stable cardiac situation. Since then, it is known that peritoneal UF does not change the course of HF, but improves the congestive state by renewed response to diuretic agents, correction of electrolyte imbalance, weight loss and overall clinical improvement. 4 In 2005, a prospective non-randomized study involving 20 patients with HF NYHA class IV showed regression to NYHA class I, recovery of systolic left ventricular function, first-year mortality lower than that expected according to comorbidity index and significant reduction of hospitalization days (13 vs. 157; p < 0.001). 5 In this study, however, patients involved had also advanced renal failure with mean baseline eGFR 14.84 ± 3.8 mL/min/1.73 m2. In 2010, a prospective non-randomized study involved 17 patients with refractory HF and a mean baseline creatinine clearance of 35 mL/min (range 15–68), initially treated by extracorporeal and then with peritoneal UF. All patients improved their NYHA functional status within the first three months and, after one year, the number of hospitalization days/patient/year decreased from 62 to 11 (p < 0.003). 6 Similar to literature data, in our patient, peritoneal UF did not change the course of the underlying heart disease, while it improved his functional status from NYHA class IV to NYHA class II, and reduced from 100 to 10 the days of hospitalization in a 17-month period.
The use of intraperitoneal solution like icodextrin promotes slow and effective peritoneal UF that preserves better residual renal function, is less invasive and more tolerated by the cardiac patients, with improvement of clinical symptoms and life quality.
Reports on peritoneal UF in HF without end-stage renal disease.