
Abstract
Summary
Objective
To compare the educational priorities patients and students raise concerning the management of multiple sclerosis (MS).
Design/setting
A single-centre comparative questionnaire survey conducted in a foundation trust hospital which provides teaching for one UK medical school.
Participants
A total of 255 people with multiple sclerosis (pwMS) and 125 final year medical students attending a mandatory module were invited to participate.
Main outcome measurements
Questionnaires were developed and piloted for this study and analysed on the basis of the International Classification of Functioning, Disability and Health terminology.
Results
Questionnaires were returned by 125 (50%) pwMS (age range 36–86 years; median 58) and 96 (77%) medical students (age range 22–37 years; median 23). The most commonly reported priority listed by people with MS and students concerned ‘environmental contextual factors’ (95.5% and 99%, respectively). PwMS focused primarily on the ‘social and attitudinal aspects’ of the environment (53.6%), while students expressed greater interest in the use of medications (91.7%) and investigations (14.6%) (p < 0.001). People with greater psychological or physical impact of the condition were more likely to prioritise ‘health condition’ topics.
Conclusions
PwMS and medical students identify different topics when asked to list aspects of management of MS which they deem to be important for medical student teaching. These differences in educational priorities should be taken into consideration when teaching students about MS. The findings may also apply to other long-term neurological conditions and warrant further investigation.
Introduction
During the last decade, there has been a growing interest in the contribution patients can make to the understanding that students have of long-term conditions (LTC). Patients now publish their own experiences in medical journals, act as expert patients, assist in the design of medical curricula and can also act as mentors. 1 Irrespective of these shifts in the delivery of medical education, no study has yet determined whether patients and students raise the same educational priorities regarding the management of LTC. In this study, we focused on multiple sclerosis (MS) as an exemplar of an LTC because it is a frequent cause of physical disability in young and middle-aged adults.
Objectives
The primary objective was to identify what people with multiple sclerosis (pwMS) feel medical students should learn about the management of MS and to compare these priorities with those listed by medical students.
The secondary objective was to determine whether patient and student priorities for medical education are related to any demographic or personal characteristics.
Methods
Design, settings and participants
This was a single-centre comparative questionnaire survey for which a favourable ethical opinion was obtained (reference number: 08/H0401/96).
PwMS ( > 16 years) were recruited from a rehabilitation medicine outpatient registry in a large teaching hospital which serves a population of more than 600,000 people. The medical students were recruited from all final year students attending introductory rehabilitation medicine lectures.
Outcome measures
Two questionnaires were devised (one for pwMS; one for medical students). Both questionnaires were circulated initially to a panel of experts and modified in response to their feedback. The questionnaires were distributed to 24 students and 28 patients, as part of a pilot study to test the clarity of questions and estimate the response rate. Twenty-two (92%) students and 15 (54%) patients responded. As some questionnaires were returned with missing data, the format was simplified to improve clarity.
The final version of each questionnaire invited respondents to record their age, gender and to list in order of priority five aspects of the management of MS which they felt were important for medical student teaching. PwMS were asked additional questions about their MS subtype, the year of symptom onset, the year of diagnosis, which medical follow-up appointments they attended regularly and to complete the Multiple Sclerosis Impact Scale (MSIS-29). The MSIS-29 is a disease-specific measure of the health impact of MS and provides a Physical and a Psychological Impact Score.2,3 Each score ranges from 0 to 100, higher values indicating a greater physical or psychological impact. Published administration and scoring instructions were followed, and missing values were substituted with a respondent-specific mean score, provided at least 50% of the scale items had been completed. Students were asked additional questions (e.g. had they undertaken a previous degree; did a close friend or family member have MS or another disabling LTC).
Questionnaires were posted to pwMS with an information sheet and a stamped addressed envelope, followed by a second invitation one month later. Questionnaires and information sheets were distributed to students at the beginning of an introductory lecture concerning rehabilitation and collected at the end of the session. Consent to participate in the study was assumed once a completed questionnaire was received.
Categorisation of learning priorities
The International Classification of Functioning, Disability and Health (ICF) provides a framework for describing illnesses and their impact on the individual, 4 complementing purely condition-related information, using domains for body structures and functions, activity and participation and personal and environmental contextual factors. We used the ICF as our underlying theoretical construct because its use of the bio-psychosocial model of disability would enable classification of the priorities each group of respondents listed and identify areas of overlap or difference.
A summary of the ICF domains and subcategories used to categorise the learning priorities listed by patients and students.

While mapping the priorities (see Table 1), each researcher made a list of any potential sources of error and difficulties encountered. Initially, a few discrepancies occurred in the manner each assessor categorised the patient and student priorities. These differences in understanding were discussed, and the categorisation rules were refined accordingly. It was noted, for example, that some of the priorities could be mapped to one domain only, whereas others involved two or more domains. It was agreed that priorities would be mapped to more than one domain, if appropriate. References to fatigue or pain alone were allocated to category 2 [Body functions and structures], whereas, references to fatigue or pain management were allocated to categories 2 [Body functions and structures] and 5 [Environmental contextual factors].
It was agreed that references to the involvement of friends or family members in the provision of care would be allocated to category 5 [Environmental contextual factors] as part of the wider multidisciplinary team. Similarly, references to ‘alternative therapies’ and ‘support groups’ (Table 1) were mapped to category 5. If the priority focused on the impact of the condition on family relationships, this was judged to be a ‘social and attitudinal’ response which was also allocated to category 5 [Environmental contextual factors].
The inter-rater reliability of the categories assigned by the researchers was tested using the kappa coefficient5,6 and were interpreted on the basis of Landis and Koch’s 7 ranges of agreement. The mean kappa values and 95% confidence intervals are reported.
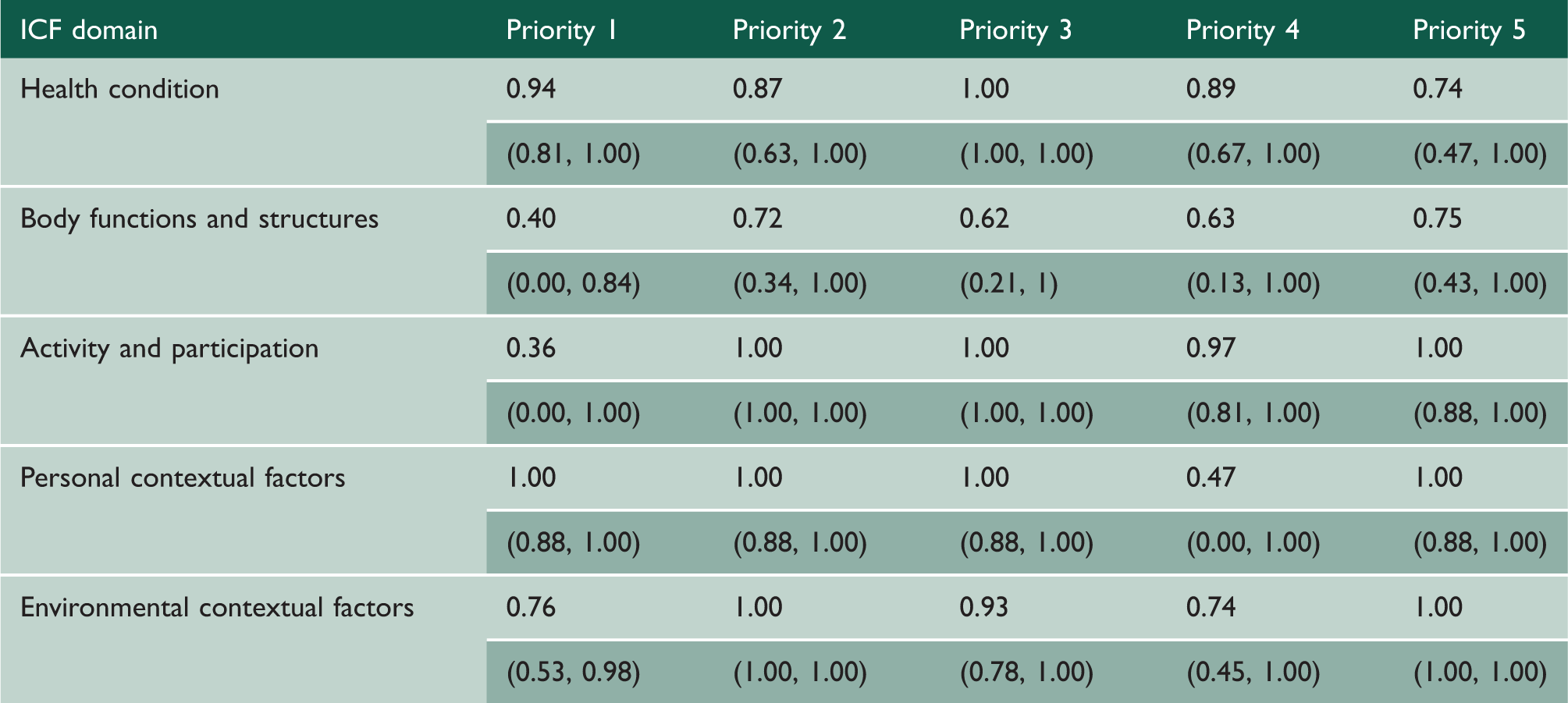
Summary of mean (95% confidence interval) kappa coefficients obtained for categorisation of patient priorities for each ICF domain.

Summary of mean (95% confidence interval) kappa coefficients obtained for categorisation of student priorities for each ICF domain.
Sample size
The sample size was derived from an estimate of ± 10% in the precision of the questionnaire results (an expected estimate 50%) at a 95% confidence interval. This indicated that at least 97 questionnaires should be completed by each group.
Statistical analysis
Statistical analysis was conducted using SPSS v18.0.3. Descriptive statistics were used to summarise the demographic characteristics of each sample and analyse the frequency of learning objectives listed. Continuous variables were tested for normality using their histograms. The age, year of symptom onset, disease duration and MSIS-29 Scores were not normally distributed. Therefore, results are presented as medians (and interquartile ranges). The association between each of these variables and each priority listed by pwMS or students was tested using the Mann U Whitney Test. The Fisher’s Exact Test was used to examine the association between the categorical variables (gender, type of MS, holding a previous degree or existence of a friend/family member with MS) and each priority.
The priorities, irrespective of their rank position, identified by patients and students were also compared collectively between the two groups using the Fisher’s Exact Test. Topics which fell within the ‘environmental contextual factors’ ICF domain were categorised further into the seven subsidiary categories (namely: assessments, investigations, drugs, therapy, aids and adaptations, physical and social or attitudinal features of the environment) as these were reported more commonly than any other subject and described very different aspects of the environment. These data were also examined using Fisher’s Exact Test to determine whether patients and students expressed similar interests.
Results
Participants with MS
Initially, 290 pwMS were identified from the database of outpatients with MS held by the Department of Rehabilitation Medicine. Checking the hospital Patient Administration System identified that seven patients had died, leaving a population of 283. Every 10th patient was invited to participate in the pilot study (n = 28). These participants were excluded from the main study leaving a residual population of 255 people. This group was further reduced to 251, as three relatives wrote to explain that the patient had died recently and a fourth person wrote to explain that the original diagnosis had been changed. Questionnaires were returned by 125 (50%) patients (Figure 1) and therefore exceeded the required sample size.
Patient selection.
Medical student participants
A total of 131 students were timetabled for introductory lectures, of whom 125 (95%) attended. Questionnaires were completed by 96 (77%) students. While this was one short of the required sample size, it did not affect the precision of estimates.
Participant characteristics
PwMS
There were 38 (30%) males, 80 (64%) females and seven (6%) pwMS who failed to report their gender. Age ranged from 36 to 86 years [median 58 years, (51–66)]. Twenty-two (18%) reported having primary progressive MS (PP-MS), 46 (37%) secondary progressive MS (SP-MS), 19 (15%) relapsing-remitting MS (RR-MS) and 38 (30%) did not complete this question. The median disease duration was 18 years (9–28), the median physical impact score obtained in the MSIS-29 was 68 (44–85) and median psychological impact score was 40 (23–65). One hundred and five (84%) patients reported that they were followed up regularly.
Medical students
The sample included 42 (44%) males, 53 (55%) females and one (1%) student who did not report his or her gender. Age varied from 22 to 37 years [median 23 years, (22–28)]. A previous degree had been undertaken by 37 (39%). Nine (9%) students reported they had a friend or a family member with MS, of whom five also reported they had a friend or family member with a disability. A further 31 (32%) students reported they had a friend or a family member with some form of disability.
Compared priorities
Comparison of all priorities identified by patients and students, irrespective of their rank position.

After analysing the environmental subcategories in greater detail, it was evident that patients were more likely to prioritise the ‘social and attitudinal features’ of the environment than medical students (53.6% and 8.3%, respectively) (p < 0.001). In contrast, medical students were more likely to express an interest in the use of medicines than patients (91.7%, 25.9%, respectively) (p < 0.001). The same distinction between students and patients also applied to ‘investigations’ (14.6%, 0.9% respectively) (p < 0.001) and ‘therapy related’ topics (88.5%, 77.7%) (p = 0.044).
The following patient extracts illustrate the nature of their interest in ‘social and attitudinal features’ and their concerns for medical student teaching: ‘Treat all patients as individuals with individual MS symptoms’ [ID 10, female, RR-MS] ‘Listen and hear what patient is saying’ [ID 46, female, PP-MS], [ID 55, female, RR-MS], [ID 102, female, SP-MS] ‘Unsteadiness when walking makes me self conscious as people think I am drunk’ [ID 73, female, SP-MS] ‘Do not patronize – give patient time’ [ID 93, female, SP-MS] ‘Because the body doesn't work doesn't mean the brain doesn't work’ [ID 89, female] ‘Not being recognized as having an illness’ [ID 107, female] ‘Be kind, understanding and listen to patient’ [ID 67, male, SP-MS] ‘The effect it has on the family e.g. restricting going out – wheelchairs etc’ [ID 40, male]
Patient priorities
Patients with more severe physical symptoms (as indicated by the MSIS Physical Impact Score) [median 81.25, (50.63–92.50)] were more likely to list a ‘health condition topic’ as their first educational priority, than those with a lower Physical Impact Score [median 62.56, (42.50–83.75) (p = 0.036)]. No comparable distinctions were found for the first priority among patients with more severe psychological symptoms (as indicated by the MSIS Psychological Impact Score), nor among those with longer disease duration or who were older.
When all of the priorities were examined collectively, no statistically significant difference was found between young and older patients in the category of topics expressed. Those who were more physically disabled [median physical impact score 79.38, (55–88.75)] were more likely to identify ‘health condition topics’ than those with a lower physical impact score [median 62.50, (39.38–81.88) (p = 0.014)]. Similarly, those who were more psychologically disabled [median psychological impact score 50, (27.7–72.97)] were more likely to identify ‘health condition topics’ than those with a lower psychological impact score [median 37.84, (18.24–59.46) (p = 0.042)]. In contrast, those who had been diagnosed for a shorter duration [median 16 years, (8–25)] were more likely to identify topics which applied to ‘body structures and functions’ than those with a longer disease duration [median 22 years, (13–34) (p = 0.011)].
Student priorities
Older students [median age 26 years, (22–30.5)] were more likely to report ‘health condition’ topics as their first educational priority, than those who were younger [median age 22, (22–25) (p = 0.006)]. Similarly, students who had undertaken a degree previously (45.9%) were more likely to report ‘health condition’ topics as their first educational priority when compared to those who had not (22%) (p = 0.023). The sample was too small to explore the relationships between age, prior degree and choice of topic in more detail.
When all of the priorities within each ICF domain were examined collectively, these distinctions were no longer evident; nor did prioritisation of topics differ significantly between males and females or between young and older students when the priorities were pooled and examined per ICF domain.
Students who had a friend or family member with a disability (n = 36) were more likely to list ‘activity and participation’ topics as an educational priority (36.1%) than those who did not (n = 60), (16.7%) (p = 0.047). No comparable distinction was found between those who had a friend or family member with MS and those who did not.
Discussion
The principle finding of this study is a clear difference between aspects of management which pwMS and medical students raise as priorities for medical student teaching. PwMS were more likely to prioritise the ‘social and attitudinal features’ of the environment, while medical students were more interested in medicines or investigations and in ‘therapy related’ topics than patients, although this latter distinction was less marked. Many pwMS also felt they had experienced discrimination due to an aspect of their health condition (e.g. dysarthria, unsteady gait).
Those pwMS with more severe physical symptoms or a higher psychological impact score had a greater tendency to state that a ‘health condition’ topic was their first priority for teaching. Those with a more recent diagnosis gave priority to topics pertaining to ‘body structure and function’.
While the main strength of this study is its aim of identifying what people with a specific LTC feel medical students should learn about its management, this study has several weaknesses. The pwMS surveyed in this study were selected through a rehabilitation medicine department and therefore at the more disabled end of the spectrum. Medical students may have prioritised therapy-related topics more commonly than patients because the study was undertaken during an introductory lecture on rehabilitation medicine in their final year. Future studies could examine priorities at an earlier stage of training, when basic history taking and examination skills are taught. The suggestions offered by both sets of respondents might have been influenced by the professional background, perceived expectations and interests of the researcher who invited their participation. The median age of the patients was higher than the medical students, which might account for some of the differences in priorities each group expressed. Cognitive and coordination impairments in pwMS could have affected their ability to complete the questionnaire and might explain why some items (e.g. age or gender) were omitted. It is also possible that relatives or carers assisted with questionnaire completion and in some cases they may have projected their own opinions.
It is worth emphasising to students that pwMS can sense discrimination and feel misunderstood and, because of this, to ensure that they give adequate time to pwMS during their consultations to listen actively and carefully to them.8,9 This finding is consistent with the results of a recent survey undertaken by the Multiple Sclerosis Society, in which 1400 pwMS and 2000 without MS took part. This survey revealed evidence of stigma, lack of knowledge and misinterpretations of behaviour. 10 Irrespective of changes made to the undergraduate curriculum in 1993 and 2002,11,12 our results indicate that misunderstandings in communication may still arise.
Since ‘health condition’ and ‘body structures and functions’ topics were a priority for many pwMS, it remains fundamental that these are taught well, in addition to social and attitudinal features. The ICF can be used as a framework for covering these dimensions when teaching students. 13
Although this study highlights both discrepancies and agreements between what pwMS and medical students think about what should be taught, the effect of putting such teaching into practice is not known. The study is also specific to one medical school in the UK, and the findings may not generalise to others. Future studies could therefore include a more comprehensive sample of both pwMS and students.