
Abstract
Ablation in octogenerians is effective and allows rationalisation of pharmacotherapy. Advancing age should not be a barrier to its use.
Introduction
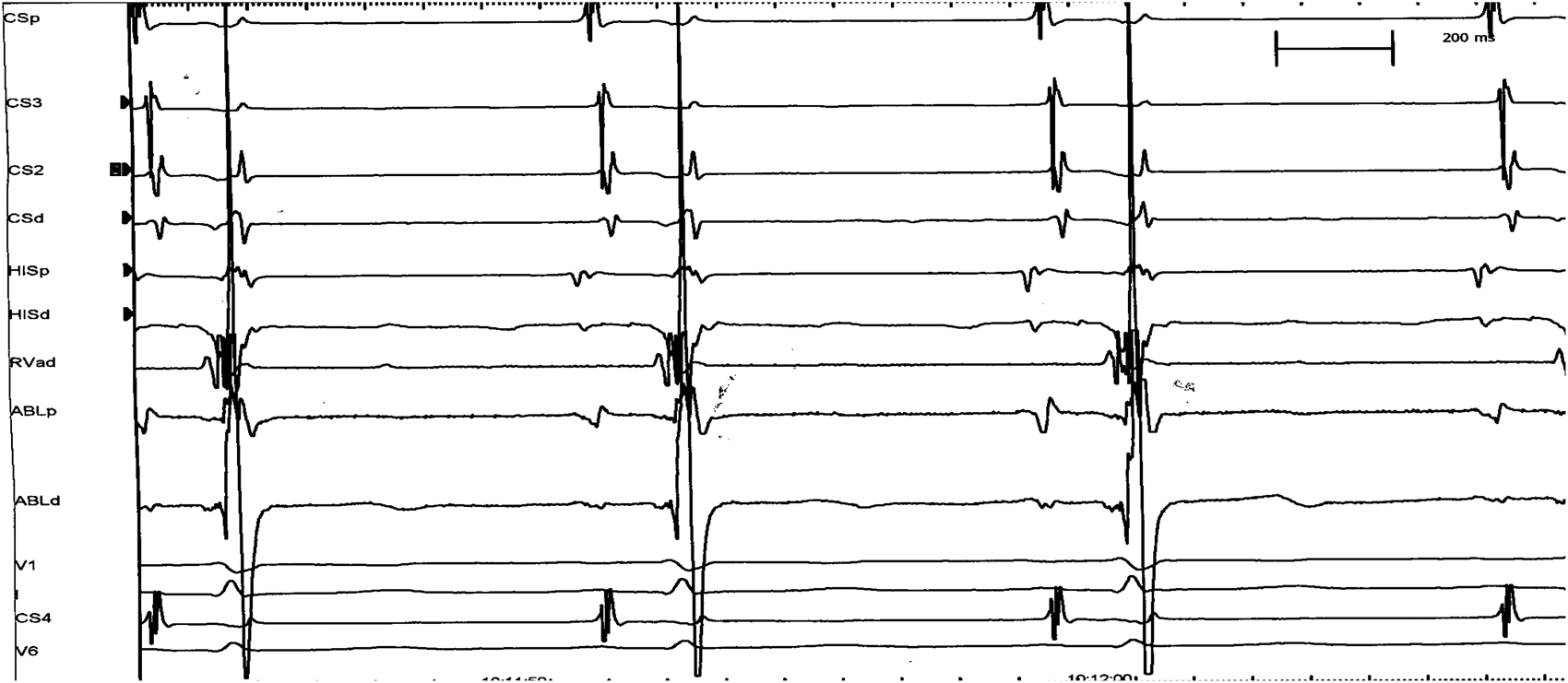
Radiofrequency catheter ablation (RFCA) involves the use of an electrode catheter to destroy small areas of myocardial tissue or conduction system that are integral to initiation or maintenance of a tachyarrhythmia (Figures 1 and 2). This provides a curative therapeutic option for some tachycardias, including atrioventricular nodal reentrant tachycardia (AVNRT).
Fluoroscopy demonstrating the position of the diagnostic recording electrode catheters a) LAO projection; bundle of His (1), within the coronary sinus (3), right ventricular apex (4) and the ablation catheter mapping the presence of the slow pathway in the triangle of Koch (2), b) same catheters in a simultaneous RAO projection. Intra-cardiac tracings during sinus rhythm prior to ablation (CSp = Coronary sinus proximal, CSd = coronary sinus distal, RVad = right ventricle apex, HISp = His bundle proximal, HISd = His bundle distal, V1, I & V6 = standard surface ECG leads, ABLp = ablation catheter proximal, ABLd = ablation catheter distal).
Success rates of >95% can be achieved with an incidence of procedural complications of <5%. 1 In contrast, antiarrhythmic medication often fails to provide satisfactory control of symptoms and is frequently associated with adverse effects. 2
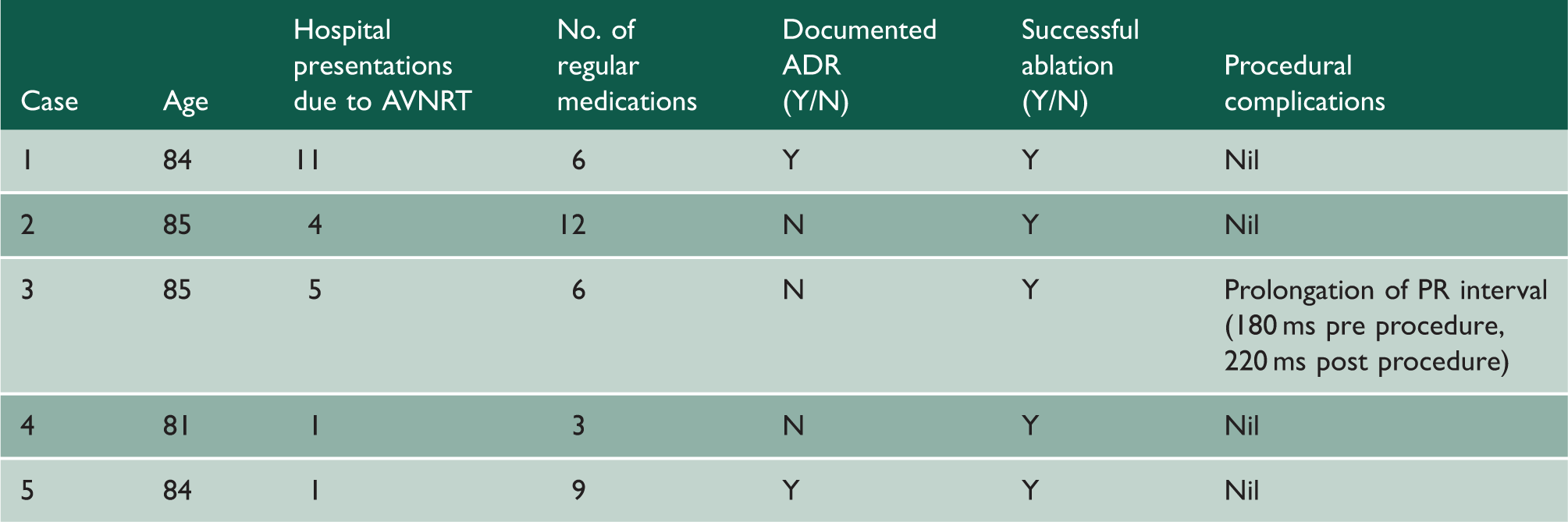
Patient characteristics.
Case 1
An 84-year-old male had a two-year history of episodic palpitations, associated with dyspnoea, collapse and syncope. His comorbidities included ischaemic heart disease, polymyalgia rheumatica and peripheral neuropathy. These symptoms resulted in multiple hospital admissions over an 18-month period, which impacted on his ability to act as carer for his wife.
Electrocardiograph (ECG) done during his palpitations showed a regular narrow complex tachycardia at a rate of 150–180 beats per minute (bpm) (Figure 3(a)), which could be terminated with intravenous (IV) adenosine.
12 Lead ECGS demonstrating patient tachycardia (Cases 1–4) and implantable loop recorder trace (Case 5).
Verapamil was ineffective in reducing his symptoms. Beta blockers were subsequently tried but were poorly tolerated.
Electrophysiological study confirmed AVNRT. The slow pathway was successfully ablated, curing his tachycardia.
Case 2
An 85-year-old male had a three-year history of intermittent palpitations, associated with chest pain. This resulted in recurrent presentations to hospital. ECG showed a narrow complex tachycardia (Figure 3(b)). His chest pain would resolve on reversion to sinus rhythm.
He had multiple comorbidites including coronary artery disease, severe aortic stenosis, essential hypertension, peripheral vascular disease, end-stage renal failure on three times weekly dialysis, prostatic carcinoma, pleural plaques and transient ischaemic attacks.
He was commenced on Verapamil but continued to have further episodes of symptomatic tachycardia, which compromised the amount of time he was able to spend on dialysis.
Electrophysiological study confirmed AVNRT. The slow pathway was mapped and ablated successfully and he was discharged home the following day.
Case 3
An 85-year-old male had a four-year history of palpitations, occurring every few weeks. He had no medical history of note and was still working as a precision engineer.
During one episode, he became syncopal, fell and consequently fractured his hip. Following this, he had four further presentations to hospital over a three-month period with prolonged palpitations. ECGs showed a narrow complex tachycardia at a rate of 170–180 bpm (Figure 3(c)).
Both beta blockers and Verapamil failed to limit his tachycardia. Electrophysiological study induced narrow complex tachycardia in keeping with AVNRT. He underwent successful ablation and has since remained off all antiarrhythmic medication.
Case 4
An 81-year-old hypertensive male had experienced intermittent palpitations for 30 years.
He presented to hospital during one episode, feeling lightheaded and unsteady on his feet.
He was found to have a narrow complex tachyardia which reverted to sinus rhythm following administration of IV adenosine (Figure 3(d)).
Electrophysiological study confirmed AVNRT and he proceeded to successful slow pathway ablation. He was discharged home the following day.
Case 5
An 84-year-old retired nurse reported an 18 month history of episodic fast palpitations. The palpitations were associated with dyspnoea, chest heaviness and syncope. She was living alone and these episodes had become a worrying threat to her safety and independence.
Due to failure to capture an episode on ECG, a implantable loop recorder (‘Reveal®’ device) was inserted. Following hospital admission with a further episode, interrogation of the device revealed a narrow complex regular tachycardia (Figure 3(e)). Electrophysiological study confirmed AVNRT. The slow pathway was successfully ablated and she was discharged home the following day.
Discussion
Polypharmacy and adverse drug reactions in the elderly
Many elderly individuals require multiple concomitant medications, due to several co-existing diseases.
Drug reactions, interactions and toxicities are often an issue. This is due to a number of factors including polypharmacy, deterioration in hepatic and renal function and alteration of drug pharmacokinetics and pharmacodynamics with advancing age.
Adverse drug reactions (ADRs) produce an increased rate of hospital admissions in elderly patients. 3 An Italian study of the elderly population found ADRs to be the primary cause for admission in 3.4% of cases. 4 The number of concomitant drugs taken was the single most important factor associated with ADR-related hospital admissions.
Cardiovascular drugs have been identified as the class of drugs responsible for the largest proportion of ADRs in the elderly, with a strong association with age. In Western Australia, cardiovascular drugs were responsible for 12.5% of ADR-related hospital stays at 60–69 years, 17.9% at 70–79 years and 21.7% at 80+ years. 3 In Italy, cardiovascular drugs were responsible for nearly 45% of ADR-related hospital admissions in the elderly population. 4
RFCA in the elderly
Both tachyaarrhythmias and antiarrhythmic medications are less well tolerated in the elderly. RFCA offers a superior therapeutic option compared to antiarrhythmic drugs, combining effective treatment with the benefit of avoiding medication burden and adverse drug effects.
Despite these advantages, it has not been widely adopted in those aged above 80 years of age. There is often a tendency to avoid invasive treatments in this population and persevere with medications which may provide suboptimal clinical effectiveness.
Several studies over recent years have shown that the longterm efficacy and safety of ablation in the >65 years group is comparable to that observed in younger adults. There are fewer studies including patients >80 years, but results have been encouraging.
Pedrinazzi et al. compared data for RFCA treatment of various arrhythmias in those aged <70 years, 70–79 years and ≥80 years and found no significant difference in the rate of major procedural complications between the groups (1.2% vs. 1.4% vs. 2%) and no significant difference in the longterm sucess rates (92% vs. 88% vs. 88%). 5
Zado et al. 6 reported results of RFCA for supraventricular and ventricular arrhythmias in octogenerians demonstrating success rates in the ≥80 years age group of 97% versus 94% in the 60–79 age group and 95% on the <60 years age group, with no significant difference in complication rate between the age groups.
Meiltz et al. 7 found that despite a higher incidence of structural heart disease in older individuals, there was no significant difference in procedure success rate, procedure duration or complication rates.
There has been some concern that advanced age increases the risk of inducing atrioventricular block when using RFCA in AVNRT. However, a study by Rostock et al. 8 exploring this concern showed that there was no increase in the rate of this complication in the ≥75 years age group, compared to those in the <75 years age group. In addition, the procedural success rate was as good in the ≥75 years group.
These findings are also supported by a large study of German Ablation Registry data published by Hoffmann et al. 9
Conclusion
In elderly patients, RFCA is increasingly considered a safe and effective treatment for AVNRT. It offers a superior therapeutic option compared to antiarrhythmic drugs by providing definitive treatment, whilst avoiding ADRs and reducing medication burden.