
Abstract
Summary
Objective
To investigate how hypochondriacal attitudes and beliefs, attitudes towards complementary and alternative medicine (CAM) and modern health worries (MHWs) related to patient satisfaction with their general practitioner.
Design
Participants completed a five-part questionnaire anonymously which measured satisfaction with one’s doctor, hypochondriacal beliefs, attitudes to CAM, MHWs and personality.
Setting
England
Participants
Included 215 adults from a variety of cultural backgrounds.
Main outcome measure
The Illness Attitudes Scales measuring the attitudes, fears and beliefs associated with hypochondriasis; Worry about Illness; Concerns about Pain, Health Habits, Hypochondriacal beliefs; Thanatophobia, Disease phobia, Bodily preoccupations; Treatment experience and Effects of symptoms.
Results
Correlations (around r = .10 to .25) and Regressions (R square from .06 to .09) showed demographic and personality variables only modestly related to patient satisfaction. Hypochondriasis, CAM and MHWs were associated with greater patient dissatisfaction as predicted with the former as the most powerful correlate.
Conclusion
The study indicates the different needs of potential patients in a typical medical consultation. It is important to ascertain patients’ health beliefs and practices with regard to medical history, attitudes to CAM and MHWs to increase consultation satisfaction.
Introduction
Research on patient satisfaction has focused a great deal on the specific variables that determine patient satisfaction of care. 1 These variables can be divided into physician and patient characteristics; features of the health concerns such as experienced pain; illness chronicity; as well as the consultation process. Patient satisfaction has also been associated with the likelihood that an individual will change his/her healthcare provider, 2 will adhere to treatment plans 3 and positive outcomes such as improved health status.
This study examines three patient factors and how they relate to satisfaction with their doctor: hypochondriasis, beliefs about and use of complementary medicine and modern health worries (MHWs).
Medically unexplained symptoms and the consultation
A great deal of the reported dissatisfaction comes from patients who present their general practitioners (GPs) with medically unexplained symptoms (MUS). 4 These include patients who may have irritable bowel syndrome 5 and chronic fatigue syndrome. 6 Somatoform disorders are also common. 7 The attitudes of the doctor are also associated with MUS patient dissatisfaction, with stigmatisation and feelings of being neglected/ignored most predictive of consultation perceptions. 8
With regard to somatoform disorders, a small percentage of general medical outpatients (prevalence 4–6%) will be diagnosed with hypochondriasis. 9 An integral feature of hypochondriasis is the characteristic preoccupation with fears and thoughts with regard to the idea that the individual has a serious illness that is based on the catastrophic misinterpretation of bodily symptoms. 10 However, this categorical approach has been refuted by those who argue that hypochondriasis is more likely to be an individual difference variable lying on a continuum. 11 There have also been extensive reports of hypochondriasis being positively associated with the higher-order personality domain of Neuroticism12,13 and negatively associated with Extroversion. 14 Its relationship with neuroticism is most interesting because neuroticism itself is often described as a predisposition to experiencing ‘somatopsychic distress’. 15 Neuroticism has been associated with increased attention to danger signals like pain and fear; 16 greater harm-avoidance behaviour 17 as well as ease of conditioning. 18 Therefore, it has been suggested that if the Big Five Factor of neuroticism is moderately to strongly correlated with subjective health complaints;19,20 preferences of doctor styles 21 and satisfaction with health-related services, 22 then hypochondriasis, as a lower-order domain of neuroticism, should also be associated with negative healthcare evaluations.
Hypochondriacal patients have medical histories that are extensive, listing high rates of GP visits, speciality consultations, requested laboratory tests and surgical procedures; 23 they often report that their experience of healthcare is both frustrating and unsatisfactory. 24 Conversely, physicians also reported these patients as more demanding within the consultation yet help-rejecting compared to other patients.
Complementary and alternative medicine and consultations
There have been several studies attempting to ascertain why complementary and alternative medicines (CAM) are continuously utilised despite the inconclusive evidence as to their effectiveness.25–27 Satisfaction with CAM therapies tends to be high, with studies showing that 63.3% of CAM users perceived their therapy to be very and extremely effective. 28 One explanation is that the consultation processes predict patient satisfaction.
CAM use appears to be associated with dissatisfaction of the cost of orthodox treatments and clinic waiting times 29 compared to CAM consultations. CAM practitioners are said to take a holistic approach to treatments,30–32 treating not just the health concern, but also the psychological aspects that may interact with the medical problem. 33 This interacts with the increasing desire for personalised health services on the part of the patient. 34 Also, CAM therapists’ use of the holistic approach would mean that consultation times are longer, which would also affirm their persuasiveness in the face of GP consultations. 32 Evidence has shown that brief GP encounters leave patients feeling disempowered, 35 whereas CAM consultations seem to provide individuals with an increased perception of self-health control. 36
However, it is likely that characteristics of CAM users all mediate the perceived success of consultations. Patients who are more likely to use CAM therapies believe that the emotional states play an integral role in self-health and that GPs often neglect this aspect of healthcare. 37 They are generally more health conscious and report themselves as having less faith in ‘provider care’, essentially that medicine cannot singularly resolve ill health. 27
Modern health worries
Negative perceptions of modern living such as the problems posed by increases in drug resistant bacteria, environmental pollution and pesticide use have led to heightened health perceived vulnerability. 38 These MHWs have been used to evaluate one theory of how individuals interpret their unexplained medical symptoms.38,39
Increased utilisation of the healthcare services, 40 as well as positive attitudes towards CAM therapies41,42 have been associated with MHWs. Suggested consequences of these associations are that the heightened concerns of ill-health drive patients to consume more healthcare products, whilst CAM practitioners may focus on emphasising the issues of modern living behind MHWs. 41 This, therefore, reinforces their health concerns, such that CAM therapies validate their MHWs and perpetuate their overall health beliefs. Subjective health complaints have been found to mediate the relationship between MHWs and orthodox and alternative healthcare utilisation, 40 such that people are more likely to interpret their symptoms as a serious illness in which over-the-counter medicines will not be sufficient.
The current study
This study aimed to investigate various hypotheses: that hypochondriacal attitudes and beliefs will be significantly negatively associated with doctor satisfaction (H1); that positive attitudes towards CAM are associated with greater doctor dissatisfaction (H2); and that high MHWs will be associated with Medical Care dissatisfaction (H3). In addition, the study aimed to investigate which of the factors examined: hypochondriasis, CAM attitudes and MHW were the most powerful predictors of patient satisfaction.
Methods
Subjects
In total, 215 participants took part in this study. In all, 73% (157) of the sample were female, whilst 27% (58) were male. Ages ranged from 18 to 67 with a mean age of 29.59 years (SD = 12.17). In all, 66.50% of subjects were Caucasian; 12.60% were Asian; 5.10% were Afro-Caribbean and the remaining 15.8% fell into the category of ‘Other’. A third were graduates. Within the sample, 29.30% had received some form of counselling; 70.20% reported that they had not received counselling and 18.6% had been hospitalised in the past 12 months. The mean rating for self-health was 6.07 (SD = 1.38), whilst rating of self-health compared to others of the same age was on average 6.33 (SD = 1.40).
Questionnaires
The Europep questionnaire 43 is a measure of patient satisfaction with their GP. There are 23 questions in total with five subscales. Participants rate the quality of their experience with their GP on a scale from 1 (Poor) to 5 (Excellent).
The Illness Attitudes Scales (IAS)44,45 were designed in order to assess the hypochondriacal spectrum. Overall, there are nine self-rating scales measuring the attitudes, fears and beliefs associated with hypochondriasis; Worry about Illness; Concerns about Pain, Health Habits, Hypochondriacal beliefs; Thanatophobia, Disease phobia, Bodily preoccupations; and Treatment experience and Effects of symptoms.
Use and perception of CAM was investigated through a 12-item questionnaire. 33 The first question explicitly asks about the participant’s experience with CAM therapies, while subsequent questions refer to evidence that CAM therapies work (3 questions); the reputation of CAM (5 questions); safety (1 question) and the manner of the CAM practitioners (1 question).
MHWs were measured by an adapted 25-item questionnaire. 46 These items were designed to assess concerns regarding particular aspects of modern living that may have an effect on health. There are four subscales: toxic interventions, environmental pollution, tainted food and radiation.
Personality was assessed by the 10-Item Personality Inventory. 47 This is a short questionnaire designed to assess the Big Five Factors of personality: Neuroticism, Extroversion, Openness to Experience, Agreeableness and Contentiousness. 48 Participants are asked to rate dyads of adjectives on how they see themselves as relating to the adjectives.
Procedure
Departmental Ethics permission (UCL: CEHP/2013/514) was sought and received. Some participants (around 25%) were recruited from public places and asked to complete the paper questionnaire. The length of the questionnaire meant there was approximately a 60% response rate. Also, an online version of the questionnaire was distributed through Kwiksurveys.com. There was no overall difference in the background of the two samples completing the question on paper and online.
Results
Demographic details
Demographic variables were correlated with patient satisfaction and predictor variables IAS scores, CAM and MHW. Patient satisfaction was not significantly associated with age, sex, education levels and self-health. It was positively correlated with compared health. There was a positive correlation between age and IAS (r = .18, p < .001) (CI = .14 to −.14) scores suggesting that as age increases hypochondriacal attitudes and beliefs increase. There was a negative correlation between self-health (r = −.34, p < .001) (CI = −.45 to −.21) and compared health (r = −.31, p < .001) (CI = −.21 to −.17), and IAS scores, suggesting as education levels increase perceived self and compared health and hypochondriacal attitudes decrease. Attitudes towards CAM were not significantly correlated to age, sex, education levels, compared health ratings and self-health ratings. MHWs were significantly correlated with age (r = .19, p < .01) (CI = .12 to −13), whilst correlations to sex, education levels, self-health ratings and compared health ratings were not significant.
Means, SDs and alphas for the main scales.

IAS: illness attitudes scales; CAM: complementary and alternative medicine; MHW: modern health worry.
Patient satisfaction
Descriptive statistics for Europep patient satisfaction questionnaire.

Correlations between IAS scores, CAM and MHWs and patient satisfaction and subscales.

IAS: illness attitudes scales; CAM: complementary and alternative medicine; MHWs: modern health worries.
†: n = 215; ‡: n = 210.
*p < .05, ** p < .01, *** p < .001.
Correlations between patient satisfaction, dimensions of patient satisfaction, IAS, CAM, MHWs and personality variables.
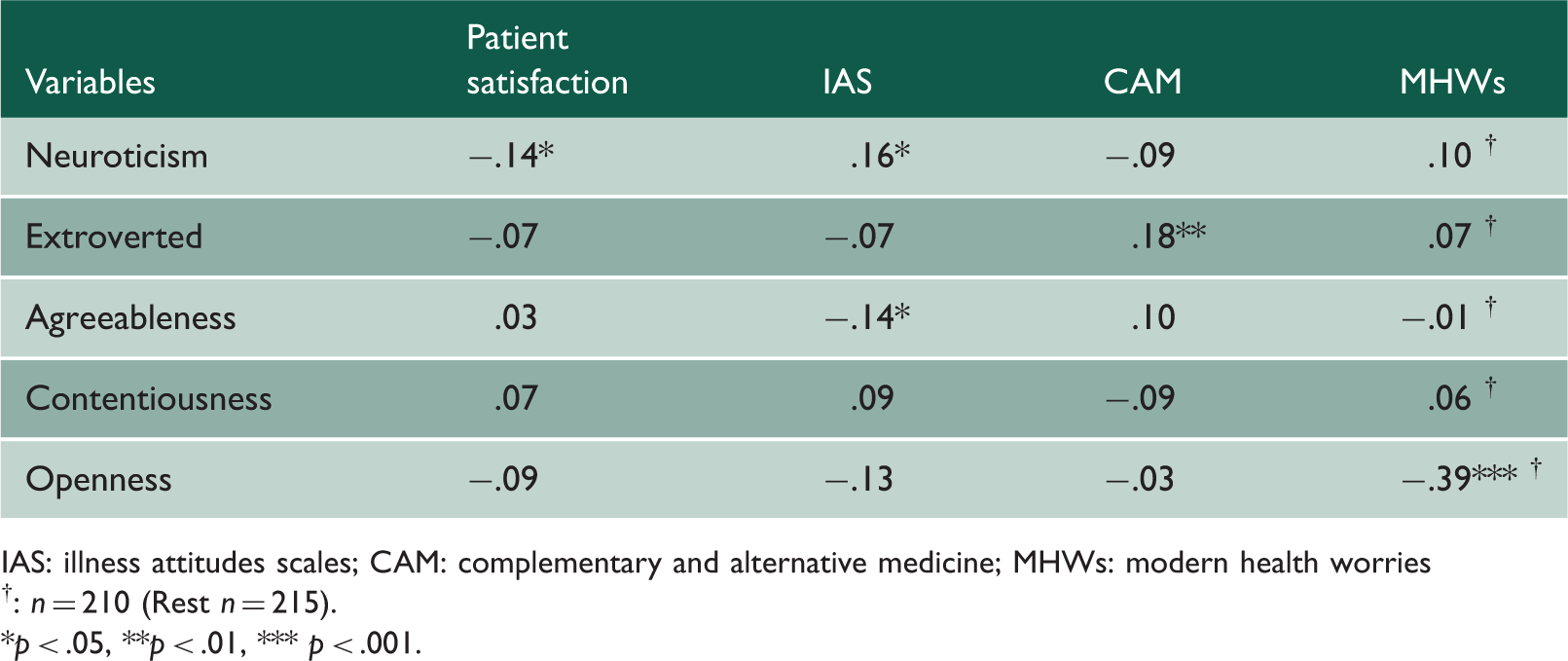
IAS: illness attitudes scales; CAM: complementary and alternative medicine; MHWs: modern health worries
†: n = 210 (Rest n = 215).
*p < .05, **p < .01, *** p < .001.
Hierarchical regression analysis for variables predicting doctor satisfaction (n = 209).
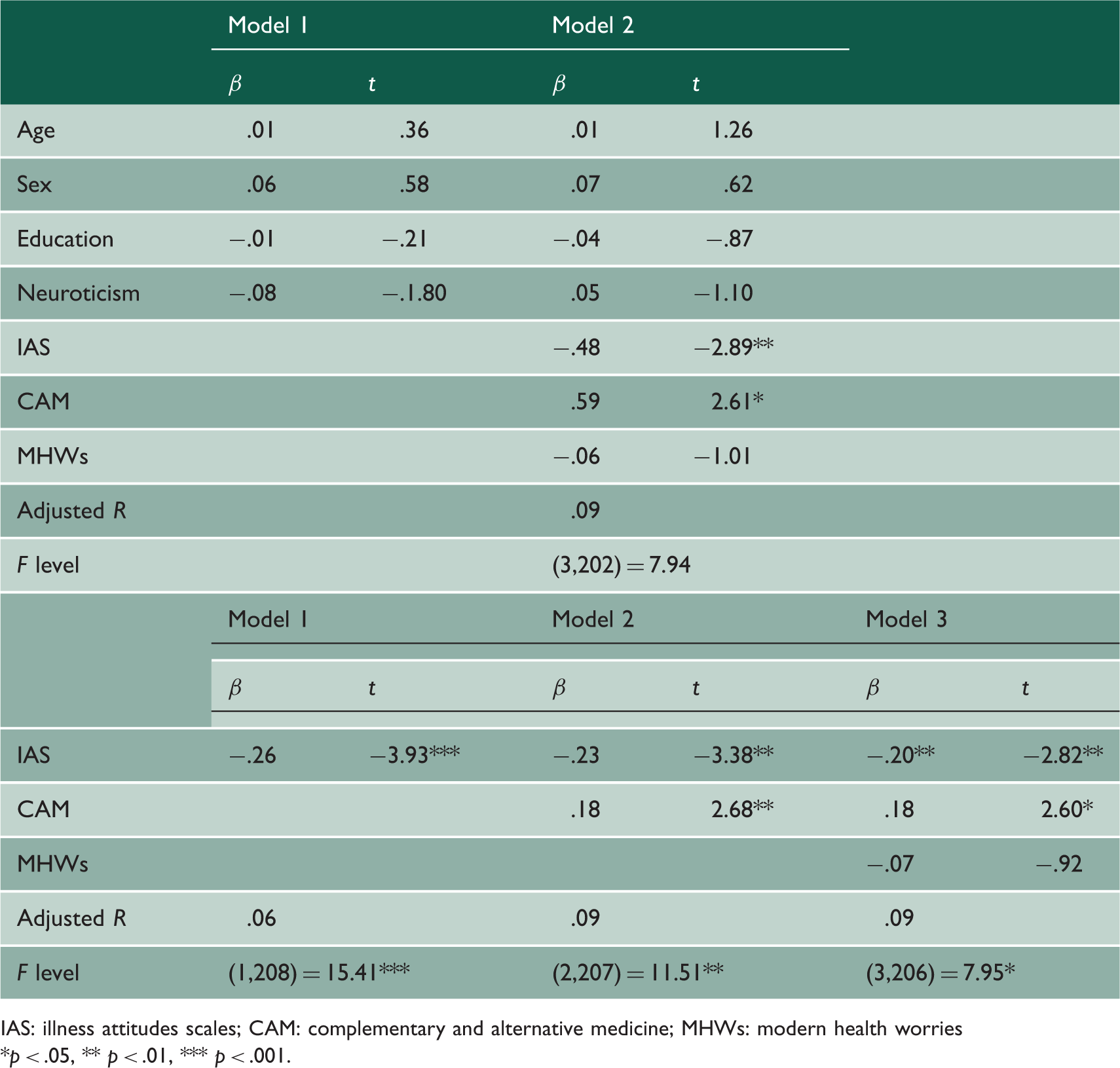
IAS: illness attitudes scales; CAM: complementary and alternative medicine; MHWs: modern health worries
*p < .05, ** p < .01, *** p < .001.
A second hierarchical regression was used in order to determine which of the predictor variables would best account for the variance in patient satisfaction. For this, IAS was entered into one block, CAM attitudes into the second and MHWs into the third block. Overall, the regression was significant (R2 = .10, F(3,206) = 7.95, p < .001). IAS scores accounted for 6.9% of the variance in patient satisfaction. When CAM attitudes were added to the model, there was a significant increase in R2 by 3.1% to 10%. However, there was no significant increase in the amount of variance accounted for by the model when MHWs were added. This suggests that hypochondriacal attitudes and attitudes towards CAM are better predictors of patient satisfaction compared to concerns over modern health issues.
Discussion
As predicted, hypochondriacal beliefs were negatively associated with patient satisfaction, showing that those who are high in hypochondriacal attitudes and beliefs are less likely to be satisfied with their doctors. 24 Hypochondriacal attitudes and beliefs explained 7% of the variance within patient satisfaction. The fact that those who have hypochondriacal attitudes and beliefs report greater dissatisfaction with the healthcare services could be due to an increased number of encounters with GPs. 23 Thus, the fact that they feel they have to persist until they find a GP who treats their perceived symptoms influences their negative appraisals of the healthcare services in general.
Consequently, those who have high hypochondriacal attitudes and beliefs could have different expectations regarding healthcare. Unmet expectations can be a significant predictor of patient satisfaction. 51 Their hypochondriacal beliefs could heavily influence these expectations; their attention to pain signals may result in the misinterpretation of bodily symptoms, 16 which in turn influence expectations that include extensive healthcare providence, such as clarification and tailored treatments. However, because they often encounter GPs who do not perceive their symptoms as an actual medical problem, these expectations are not met. Hypochondriacal attitudes and beliefs appear to be most associated with the relation, communication, information and support provided for by GPs. This could be explained in terms of the coldness they encounter from their GP.
Consistent with the literature, there was a significant relationship between those who scored high on Neuroticism scores on hypochondriacal beliefs. 13 Neuroticism could predispose individuals to experience negative emotional states, particularly that of anxiety. Anxiety could be transferred to perceived symptoms that are misinterpreted as life threatening. 16 This in turn validates their negative emotional state.
This study showed that personal health ratings were negatively associated with hypochondriacal attitudes and beliefs, such that perceptions of low self-health were more likely to be present in those who exhibited hypochondriacal attitudes and beliefs.20,52 The uncertainty and fear surrounding misinterpreted sensations are brought to the consultation process. Where the patients have a great deal of fears concerning the health issue and are more negatively emotionally involved with their perceived health problem, 53 they are more inclined to have expectations of the GP providing answers to their questions. 54 However, when met with a GP who perceives their symptoms to be medically unexplained the quality of the GP communication and patient treatment can be greatly reduced. Therefore, the patient does not receive the answers they need and their fears are not calmed.
CAM and satisfaction
Attitudes towards CAM were also significantly associated with patient satisfaction, such that those who had more positive views of CAM were less likely to report overall satisfaction. Interestingly, whilst attitudes to CAM were associated with the relation and communication of GPs as well as the information and support provided, CAM attitudes appeared not to be associated with medical care. Perhaps, it is because these patients are not motivated by the medical care aspect, but rather by the consultation process itself. CAM therapists are thought to take on a supportive role, treating the entire individual as opposed to GPs who focus in on the specific medical complaint exclusively.30,32 Emotional states appear to be generally viewed by individuals who use CAM as integral to gaining positive health. 37 In particular, the notion of self-health control 36 and empowerment, which is perceived to be missing from GP encounters but usually present in CAM consultations.
CAM attitudes were positively related to the personality dimension of Extroversion, indicating that those who are more positive in their appraisals of CAM are more likely to be out-going and assertive. Studies have failed to find conclusive results with regard to personality predictors of CAM users. 55 This may be because the type of CAM used attracts different personalities or that other variables such as health history are more predictive.
Modern health worries
MHWs were negatively associated with patient satisfaction. An increasing focus of the media on potential health hazards, such as the increasing resistance of bacteria to antibiotics and amplification of instances where environmental pollution has occurred, appears to play an important role in shaping responses to these issues. 46 The tendencies of individuals reacting to symptoms, such that the saliency of MHWs leads to a catastrophised interpretation, are similar to those exhibited by individuals with somatoform disorders 56 as well as changes in behaviours related to health problems. 46
Similar to those with hypochondriacal beliefs, their dissatisfaction could be a product of increased encounters with GPs. However, it is more likely to result from the already salient negative beliefs of modern medicine such that they regard their GPs with suspicion and often interpret their treatment plans as being unsafe. 57 Additionally, those with MHWs may be more active within their medical encounters, due to their high concerns over the efficacy and safety of modern medicine, resulting in higher likelihood of hostile confrontation with their GPs. This is also supported by the evidence that MHWs were most significantly associated with the medical care component of patient satisfaction, further suggesting that it is the nature of the treatment that GPs offer that is most likely to result in patient dissatisfaction.
MHWs were found to be negatively associated with the personality dimension of Openness, a finding that is contradictory to a positive relationship in previous literature. 58 It is possible that regarding modernity with scepticism could be influenced by the degree to which an individual is open to experiencing new technologies. If they are unwilling to experience these new technologies, then they could be more likely to have increased MHWs. However, this is speculative and future evidence is required.
Conclusion
Perhaps, the most important part of this study was the results of the regressions shown in Table 5. They indicated that more than any other factor examined, it was patient hypochondriasis that was most strongly related to satisfaction followed by CAM attitudes. Trait neuroticism and MHW though related to satisfaction ceased to be significant in the regressions. In all, 10% of patient satisfaction could be explained by just two short questionnaires. It must be noted, however, that the predictor variables examined here only accounted for a small amount of variance in patient satisfaction. This shows that whilst they are important, there are still other factors to be considered. These factors could interact with these predictors and perhaps better explain the variance in patient satisfaction. It should be noted that hypochondriasis has a small prevalence, even for its sufferers' extensive utilisation of the healthcare services, and that there are several other somatoform disorders, as well as MUS, that could account for the variance in patient satisfaction that focusing on hypochondriasis might miss.
Like all studies, this one had limitations. This study was limited to cross-sectional and self-report methodology on a non-representative sample. Whilst they are effective in determining associations between the variables and allowing explanations of the hypotheses, they do not allow testing casual relations. This study could have benefited from gaining a comprehensive medical history of the patients in order to compare it to their hypochondriacal attitudes and beliefs and determining their utilisation of healthcare services. Moreover, participants in this study were prompted to report their experiences of their GPs in the past 12 months. Finally, we did a number of analyses in this study which may have led to type II errors and over-reporting.