
Abstract
Summary
Objectives
To examine the indications for hospitalisations among haemodialysis patients.
Design
A retrospective observational study.
Setting
Alnoor Kidney Centre in Al Noor Specialist Hospital, Makkah City, Saudi Arabia, which is a Ministry of Health hospital.
Participants
Participants were prevalent patients with end-stage renal disease on regular haemodialysis in 2011, who had received haemodialysis for more than three months. Each patient was followed up retrospectively, from the first date of initiating haemodialysis to the end of 2011.
Main outcome measures
(i) The primary reasons for hospital admissions and (ii) risk factors that increase the number of hospital admissions and which increase length of stay in hospital.
Results
The primary reasons for hospital admissions associated with increases in the length of stay in hospital were diseases of the circulatory system (which increased hospital bed days by 70%; 95% CI: 11–161%; p value = 0.01 compared to all other reasons). The risk factors that increased the number of hospital admissions per patient-year at risk were increasing age (incidence rate ratio [IRR] = 1.02 per 1 year of age; 95% CI: 1.01–1.03; p value = < 0.0001); receiving haemodialysis through a catheter compared to arteriovenous fistula (IRR = 2.55; 95% CI: 1.14–4.97; p value = 0.001) and diabetes as a cause of renal disease compared to hypertension (IRR = 1.84; 95% CI: 1.29–2.63; p value = 0.001).
Conclusion
Indications for hospitalisation and consequences of practices related to hospitalisation for haemodialysis patients should be studied in further research to provide a comprehensive evidence-based management policy for haemodialysis patients in Saudi Arabia.
Background
The high cost of hospitalisation for haemodialysis patients has become a public health concern 1 because an increase in the haemodialysis population together with escalating healthcare costs are not sustainable worldwide.2,3 The United States Renal Data System report highlighted that the rates of hospital readmissions for end-stage renal disease (ESRD) patients are twice those in the general Medicare population. 4 Patients with chronic kidney disease in the late stages are often hospitalised with general medical problems, especially those patients who have reached the end-stage of renal failure and are receiving regular haemodialysis in dialysis centres. Patients on haemodialysis require more resources than patients on peritoneal dialysis or with renal graft need, 5 especially during the first year of dialysis treatment; these resources include vascular surgery, radiology, physician cost and hospitalisation. 6
In Saudi Arabia, the incidence and prevalence of renal replacement therapy (RRT) have been increasing continuously in the last three decades with a high prevalence of co-morbid conditions.7,8 The most common method for treating patients with ESRD in recent decades has been haemodialysis, which accounts for just over half of the RRT population. The Ministry of Health (MoH) in Saudi Arabia incurs the vast majority of haemodialysis care costs and provides around two-thirds of haemodialysis facilities. 7 Although the ESRD population accounted for only 0.08% of the total Medicare population in Saudi Arabia in 2008, the healthcare costs associated with those patients were around 3.8% of the total MoH expenditure. 7 Furthermore, there is a shortage in healthcare workers in Saudi Arabia including nephrologists and nurses,7,9 which can influence healthcare quality. 1 The British Renal Society National Renal Workforce Planning Group (2002) recommended that one whole-time equivalent renal physician is required for 75–100 patients on RRT, 10 while in Saudi Arabia, one consultant nephrologist will be required for 234 patients on RRT by 2015. 7 Furthermore, patients with ESRD who had received pre-ESRD care by nephrologists before initiating haemodialysis had a better outcome throughout haemodialysis with a reduced risk of hospitalisation and mortality compared to those patients who had not received nephrology care. 11 However, in Saudi Arabia, a large proportion of haemodialysis patients do not receive pre-ESRD care. 12
The risk of hospitalisation increases among patients on haemodialysis due to complications of either haemodialysis or haemodialysis vascular access, with a high prevalence of co-morbid conditions, particularly diabetes 13 and cardiovascular diseases. 14 The type of vascular access used in the dialysis process makes a significant contribution to prognosis and quality of life.15,16 Using a catheter at the initiation of haemodialysis or throughout the time on haemodialysis increases the risk of hospitalisation, particularly due to catheter-related infection. 15 Conversions from catheter to arteriovenous fistula (AVF) have lowered the risk of hospitalisation among haemodialysis patients.16,17 In Saudi Arabia, there is limited research of the risk of hospitalisation among haemodialysis patients particularly that associated with vascular access practice patterns. A few studies conducted in different areas of Saudi Arabia have shown that a large proportion of new ESRD patients initiated haemodialysis treatment with a temporary catheter as a result of a late referral to nephrology care, a practice which is associated with increased morbidity and mortality12,18,19 and increased costs of healthcare.
The need for hospitalisation and increased healthcare costs are also related to severity of patients’ co-morbid conditions. A study conducted in Riyadh City reported cardiovascular disease as the primary reason for hospitalisation, followed by vascular access complications and infections. 20 The only other Saudi study on hospitalisation conducted in Al-Madinah City reported vascular access-related problems as the primary reason, followed by infectious disease and cardiovascular disease. 21 Neither study reported the risk factors that might increase the rate of hospital admissions or the length of stay in hospital per patient-year on haemodialysis, which could reflect both the severity of patients’ co-morbid conditions and the quality of healthcare services. Therefore, we undertook this study in one of the most active MoH hospitals in Makkah City in Saudi Arabia. We aimed to examine the indications of hospitalisation among its haemodialysis patients, by investigating the primary reasons for hospital admissions and the risk factors associated with an increase in the rate of hospital admissions and those associated with increasing length of stay in hospital.
Methods
Study design and setting
A retrospective observational study was conducted in the Alnoor Kidney Centre (AKC) in Al Noor Specialist Hospital, which is a MoH Centre in Makkah City in the western region of Saudi Arabia.
Study population
Participants were prevalent patients with ESRD on regular haemodialysis in 2011, who had received haemodialysis for more than three months. Each patient was followed up retrospectively from the day of initiating haemodialysis until the end of 2011. All patients visiting the dialysis centre who did not have a documented medical history in medical records were excluded. No patients had advanced malignancy.
A search of electronic medical records identified 418 patients with ESRD on haemodialysis in 2011. Of these, 84 were patients who were visiting the dialysis centre without a medical history, and 16 were patients who had received haemodialysis for less than three months and so were excluded.
Variables and data collection
The extracted data included demographic information, date of starting dialysis, patient status throughout 2011, causes of renal disease, vascular access at first dialysis and during follow-up, co-morbid conditions, limitation in physical motion, ever received blood transfusion and hospitalisation (the main reason for admission, dates of admission and discharge). These were collected from medical records and stored in a customised Microsoft Office Access database.
Statistical analyses
The total number of hospital admissions (excluding admissions on the day that haemodialysis was started) and the time on haemodialysis were calculated for each patient, and the length of stay in hospital was calculated for each hospitalisation. Admissions for less than one-night observation were excluded from the analysis. The primary diagnoses for hospital admissions were classified using ICD-10 codes updated in 2011 and were grouped into diagnostic categories for analyses.
Data were analysed descriptively to describe patients’ characteristics, co-morbid conditions and the distribution of the most frequent reasons for hospital admissions after starting haemodialysis in the study sample. Negative binomial regression was used among patients who were hospitalised at least once, clustered by patients, to investigate which primary reasons for hospital admissions were associated with the greatest number of hospital bed days per patient-year on haemodialysis. This is adjusted for patients’ characteristics at onset of haemodialysis such as age, sex and causes of renal disease. Negative binomial regression was also used among all patients to investigate the risk factors associated with an increase in the number of hospital admissions during time on haemodialysis, clustered by patient. This estimates the incidence rate ratio (IRR) of the number of hospital admissions per patient-year at risk for vascular access type during follow-up and for causes of renal disease, adjusted for age and sex. An equivalent model was created to examine the effect of vascular access type at start of dialysis, with the same covariates. All analyses were performed using STATA 11 (StataCorp, College Station, TX, USA).
Results
Patients’ characteristics
Of our 318 patients, 208 patients on regular haemodialysis were hospitalised at least once in Al Noor Specialist Hospital, and 110 patients did not have any reported hospitalisation there (Figure 1). The median period of haemodialysis care (period of follow-up) was 4.3 years up to the end of 2011 (25%, 75% percentiles: 2.4, 8.7), and around 8.2% of patients (26/318) had received haemodialysis for one year or under. Of the study population, 58.2% were male, and 93.7% were Saudis. The mean age at onset of dialysis was 45.6 ( ± standard deviation [SD] = 16.9) years. The dominant cause of renal disease in the study sample was hypertensive nephropathy (58.8%), followed by diabetic nephropathy (23.9%) and glomerulonephritis (4.1%). Haemodialysis was initiated through a catheter in over 80% of patients; only slightly over 7% initiated haemodialysis through an AVF. However, most patients who started with the catheter switched to AVF, so that 95% were using AVF by the end of 2011. The prevalence of co-morbid conditions was high, particularly diabetes (24.8%) and hypertension (75.2%), hepatitis B (8.5%) and hepatitis C (47.5%) (Table 1). In 2011, 25 (7.9%) patients in the study sample died, and 10 patients underwent renal transplantation although eight of them rejected the transplants. The predominant causes of death were cardiovascular disease (7 patients) and sepsis (7 patients), followed by cerebrovascular accident (2 patients), cardiac arrest (2 patients), with unknown cause of death in the remaining seven patients.
Recruitment of study participants. Characteristics of study participants. AVF: arteriovenous fistula; AVG: arteriovenous graft; PD: peritoneal dialysis.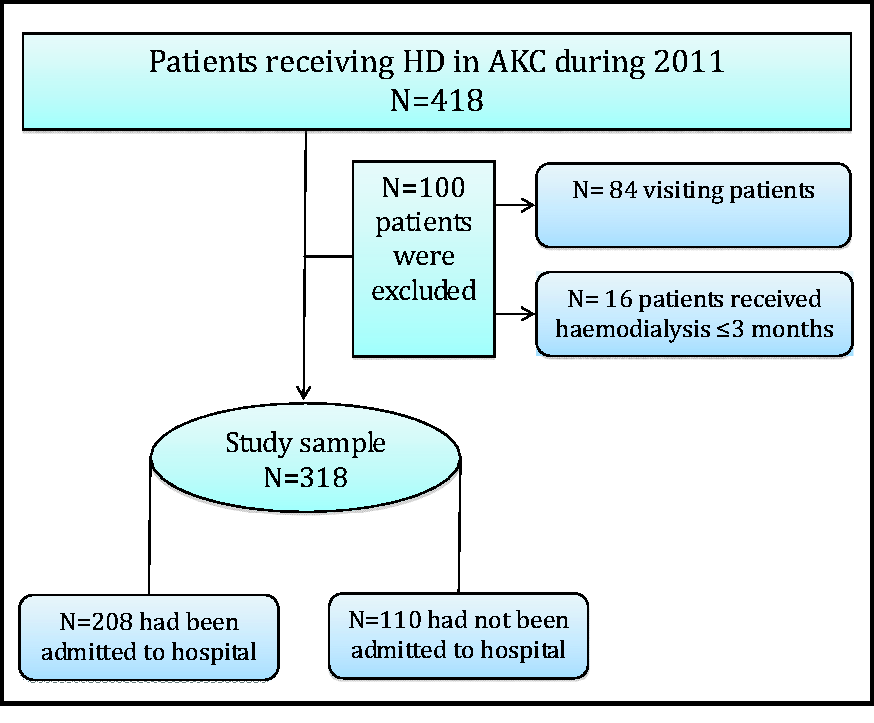

Primary reasons for hospital admissions and length of stay in hospital
Distribution of hospital admissions by diagnostic categories, and the ratio of the mean number of hospital bed days per patient-year on dialysis for each cause of hospital admission in turn, compared to all other disease groups combined.

CIs: confidence intervals.
Adjusted for age, sex, and causes of renal disease.
Reasons for the greatest number of hospital bed days per patient-year on haemodialysis among patients who were hospitalised
Adjusted ratio of the mean number of hospital bed days per patient-year on dialysis by patient characteristics at baseline.

CIs: confidence intervals.
Data are analysed separately for each reason for hospital admissions in turn.
Factors that increase the risk of hospital admissions per patient-year on haemodialysis
Incidence rate ratio (IRR) of number of hospital admissions per patient-year on dialysis.

CIs: confidence intervals; AVF: arteriovenous fistula; AVG: arteriovenous graft; PD: peritoneal dialysis.
Adjusted for age, sex, access type at start of dialysis, and cause of renal disease.
†Adjusted for age, sex, access type during follow-up, and cause of renal disease.
Discussion
This study gives an overview of the primary reasons and indications for hospitalisation among ESRD patients on haemodialysis in one of the most active MoH hospitals, which may reflect the severity of patients’ co-morbid conditions or the quality of healthcare practices. The length of stay in hospital usually reflects the severity of illness and underlying patient health status. This study shows that cardiovascular diseases had the highest impact on hospital bed days, among patients who are ever hospitalised. This increases hospital bed days per patient-year on haemodialysis by 70% compared to other reasons for hospital admission. While the most prevalent co-morbid conditions were diabetes and hypertension, which are strongly associated with an increased risk of developing cardiovascular disease, which may often occur before ESRD.22,23 This probably reflects poor management or lack of early detection of chronic diseases. Furthermore, this study found that an increase in one year of a patient’s age, which is an unmodifiable risk factor, had a significant effect in increasing the length of stay in hospital and the rate of admissions by 2% per patient-year on haemodialysis. Both diabetes and glomerulonephritis as causes of renal disease, and using a catheter as access point for haemodialysis, increased the rate of hospital admissions. In this study, only 7% of haemodialysis patients commenced dialysis with AVF, while the NKF/KDOQI and the Renal Association guidelines for vascular access have recommended that 65% of all incident haemodialysis patients should initiate dialysis with AVF.24,25 Although the vast majority of the study population commenced haemodialysis with a catheter as a result of late referral to nephrology care, most of them had converted to AVF, which reduced risk of vascular access complications, especially infections, hence lowering risk of hospitalisation. This study demonstrated that patients who had used a catheter throughout the follow-up period showed a 2.5-fold increase in the rate of hospital admissions compared to those who had used AVF. Therefore, the high prevalence of hospital admissions due to vascular access throughout haemodialysis was mainly attributed to creating AVF as a permanent vascular access rather than vascular access complications. This study demonstrates that the goals of vascular access placement for the NKF/KDOQI and The Renal Association guidelines24,25 have been achieved in AKC, whereas the prevalent functional AVF placement rate was around 95% of patients in AKC in 2011, which is higher than the recommended goal of over 65% in NKF KDOQI and 85% in the Renal Association. However, according to the Saudi Centre for Organ Transplantation data report in 2011, the prevalent functional AVF placement rate in all centres in Saudi Arabia was 71% of patients, 8 which is lower than the rate in AKC. This indicates the differences in haemodialysis practices and outcomes between healthcare centres, suggesting diversity in competencies and training between healthcare institutions and/or inequality in allocating relevant healthcare resources between healthcare centres in Saudi Arabia. 7
The potential limitations of this study were that the study was conducted retrospectively at a single centre for prevalent patients in 2011 due to time limitations for collecting data and a lack of national health information systems in Saudi Arabia. Therefore, it was not possible to examine the trend in the annual rate of hospitalisation by calendar year. Important data for many patients were missing, such as clinical and laboratory measurements at start of dialysis and the time at which all co-morbid conditions were diagnosed, limiting which variables were available for analyses. Around one-third of the study sample (who all came to AKC for dialysis) did not have any reported hospitalisation in Al Noor Specialist Hospital. Some of them (and some patients hospitalised also in Al Noor) may have been hospitalised in another hospital such as a private hospital, with others not needing hospitalisation. These issues could affect the precision of the results, as could any accuracy in hospital admissions data records. There may on occasion be inappropriate hospitalisation in the governmental hospitals in Saudi Arabia, which does not fully reflect patients’ health conditions, mostly because there was nobody able to look after the patients outside hospital, 26 particularly for elderly patients, who require more care than younger patients, as demonstrated in this study by the strong association of the increased length of stay in hospital and admissions rate that we found with increasing patient age, might also reflect the severity of patients’ co-morbid conditions disease.
This study reveals that the most frequent reasons for hospital admission among haemodialysis patients were cardiovascular disease, particularly hypertension and coronary artery disease, creation of vascular access via AVF after starting dialysis, infectious diseases particularly respiratory infectious disease and endocrine and metabolic disorders. Increased age, diabetes as a cause of renal disease and using a catheter as access point for haemodialysis have a significant effect in increasing the rate for hospital admissions per patient-year on haemodialysis. These indications for hospital admissions provide evidence for public health administrators and healthcare providers in Saudi Arabia to develop multidisciplinary strategies for improving pre-ESRD nephrology care practice and the quality of healthcare management for patients with multiple chronic diseases and their complications, patients’ health behaviours and awareness about their illness. These strategies would be valuable in the future to improve healthcare outcomes and reduce hospital utilisation and the cost of haemodialysis care.
Conclusion
This study suggests that early detection and effective management for patients with high risks to cardiovascular disease, such as diabetic and hypertensive patients, could reduce the risk of hospitalisation even before the onset of haemodialysis. Pre-ESRD nephrology care practice should be modified to reduce the rate of initiating dialysis with catheters as this is associated with an increased rate of hospital admission among haemodialysis patients. Health information systems must be developed in Saudi Arabia to allow further multicentre studies that include other key data such as clinical and laboratory measurements, and details of healthcare providers' specialist services; and the outcomes of hospitalisation for haemodialysis patients. This would help to provide comprehensive evidence-based guidance on the clinical management of haemodialysis patients in Saudi Arabia.