
Abstract
Summary
Objectives
To estimate trends in infection/colonisation with meticillin-resistant Staphylococcus aureus (MRSA) in an intensive care unit (ICU).
Design
Observational study of results of ICU admission and weekly screens for MRSA.
Setting and Participants
All ICU admissions in 2001–2012.
Interventions
ICU admissions were screened for MRSA throughout. In late 2006, screening was extended to the whole hospital and extra measures taken in ICU.
Main outcome measures
Prevalence of MRSA in ICU admissions and number acquiring MRSA therein.
Results
In all, 366 of 6565 admissions to ICU were MRSA positive, including 270 of 4466 coming from within the hospital in which prevalence increased with time prior to transfer to ICU. Prevalence in this group was 9.4% (8.2–10.6) in 2001–2006, decreasing to 3.4% (2.3–4.5) in 2007–2009 and 1.3% (0.6–2.0) in 2010–2012, p < 0.001, due to decreased prevalence in those spending >5 days on wards before ICU admission: 18.9% (15.6–22.2) in 2001–2006, 7.1% (4.0–10.2) in 2007–2009 and 1.6% (0.1–3.1) in 2010–2012, p < 0.001. In addition, 201 patients acquired MRSA within ICU, the relative risk being greater when known positives present: 4.34 (3.98–4.70), p < 0.001. Acquisition rate/1000 bed days decreased from 13.3 (11.2–15.4) in 2001–2006 to 3.6 (2.6–4.6) in 2007–2012, p < 0.0001. Of 41 ICU-acquired MRSA bacteraemias, 38 were in 2001–2006. The risk of bacteraemia in those acquiring MRSA decreased from 25% (18.1–31.9) in 2001–2006 to 6.1% (0–12.8) thereafter, p = 0.022.
Conclusions
Following better hospital-wide infection control, fewer MRSA-positive patients were admitted to ICU with a parallel decrease in acquisition therein. Better practice there reduced the risk of bacteraemia.
Keywords
Introduction
In 2004, we reported the problems posed by meticillin-resistant Staphylococcus aureus (MRSA) in the intensive care unit (ICU) of this hospital. 1 Our experience was similar to that of others.2,3 Prevalence in admissions approached 10%, acquisition of MRSA within ICU was common and campaigns to improve control were ineffective. 1 One-fifth of those acquiring MRSA progressed to bacteraemia associated with a 20% excess absolute mortality. 4
Within this ICU, patients have been screened for MRSA at admission and weekly thereafter with eradication therapy and segregation/cohort nursing for positives since 1996. There were no systematic hospital-wide control measures for MRSA until late 2006 when this practice was extended to all hospital wards, with a dedicated ward for positives, together with a programme of ward cleaning, campaigns on hygienic hand cleansing, a dress code for medical staff and additional measures in ICU. 5 Thereafter, prevalence of MRSA in admissions to ICU decreased, and fewer patients acquired MRSA therein with a reduction in ICU-acquired MRSA bacteraemias. 5 Preliminary analysis suggested fewer MRSA-positive admissions as the sole mechanism. 6
This report re-analyses previously published data1,5,6 and extends observation to the end of 2012 and seeks to determine whether the decrease in MRSA positives has continued and whether prolonged observation might detect an effect of the additional measures within ICU.
Patients and methods
The characteristics of our ICU, infection control and microbiological methods have been described in detail.1,4,5,7 Throughout the study, the ICU had nine beds including two single rooms and a two-bed bay, and it admitted adults from all specialities and accepted transfers from elsewhere. Details of all admissions were entered into a database, and day one APACHE II score calculated for eligible patients. 8 Admissions classified as coming from the emergency department (ED) included patients from the medical and surgical assessment units transferred within 24 h. These patients had minimal exposure to the hospital environment prior to ICU admission. The study includes all admissions to the ICU between 1 January 2001 and 31 December 2012.
Till late 2006, infection control measures included hygienic hand cleansing on entering and leaving ICU and between patient contacts. Bed bays were cleaned daily and between admissions. MRSA-positive patients were identified as such, treated with Mupiricin and/or Triclosan, and segregated and/or cohort nursed where possible, and those attending wore gowns and gloves, with thorough cleaning of the bed space daily and at discharge. 1 In late November 2006, the ICU was deep cleaned, re-decorated and ventilation upgraded, and wipeable keyboards and theatre scrubs for medical staff introduced. 5 Care of vascular lines was standardised, and all patients washed daily with Stellicept (4% undecylenamidopropyltrimonium methosulphate and 2% phenoxyethanol) irrespective of MRSA status. 5
In late November 2006, screening was extended to all hospital wards with eradication therapy and segregation in a dedicated ward for positives. 5 A ‘bare forearms’ dress code was introduced for those attending patients, ward cleaning regimes strengthened, with repeated campaigns to encourage hand hygiene of staff and visitors 5 and further standardisation of antibiotic prescribing policy.
Throughout the study, all patients coming to ICU had nasal and groin swabs at admission and each Monday thereafter. Other cultures were taken as clinically indicated. During the study, different selective media were used: mannitol sugar agar with salt broth enrichment (Bio-Merieux, Basingstoke) 2001–3, oxacillin-resistant screening agar (2003–2005) and then MRSA Id Chromogenic agar (Bio-Merieux, Basingstoke). Organism identification was confirmed by automated biochemical and sensitivity testing (Vitek 2, Bio-Merieux, Basingstoke). As previously reported at times of change, old and new methods were run in parallel. 5 Results of cultures were stored on the Microbiology database.
Cultures from which MRSA was grown were entered on a spreadsheet to show the number of positive patients in ICU each day, which were assumed to remain positive until discharge or a subsequent negative culture from the same site. MRSA grown from admission screens or any site within 48 h was considered imported, while any first positive culture on or after the fifth day was deemed ICU acquired. 5 This definition of ICU-acquired infection was derived from a study of 1400 blood cultures in this ICU 7 and used by us thereafter.4,5 Twelve patients with a first growth between 48 h and the fifth day were plotted on the spreadsheet but excluded from further analysis. ICU-acquired MRSA bacteraemia was defined as a first positive blood culture on or after the fifth day in patients with no growth of MRSA from any site within 48 h of ICU admission.4,5,7 The rate of acquisition of MRSA within ICU was estimated as the number with a first positive culture on or after the fifth day divided by the number of bed days occupied by all patients staying five or more days who were free of MRSA at admission less bed days after the first positive culture in those acquiring MRSA. This is a modification of our previous method, which excluded the first four days in ICU from the denominator. 5 A patient was classified as having acquired MRSA in the presence of a positive patient if at least one was present for at least one day between admission or last negative weekly screen and first positive culture. If no known positives were present in this interval, then acquisition was classified as in the absence of known MRSA. For each patient free of MRSA at admission staying ≥5 days, the number of bed days during which known MRSA positives were present and absent was calculated from the spreadsheet, and hence the total bed days when positives were present and absent for this group derived. If the risk of acquiring MRSA each day is r(+) when positives are present and r(−) in their absence and if during a patient’s stay positives are present on d(+) days and absent on d(−) days, then the probability of that patient acquiring MRSA is [(r(+) × d(+)) + (r(−) × d(−))]. For all patients remaining ≥5 days, r(+) = the number acquiring MRSA when positives were present/total bed days when positives were present less the bed days occupied post acquisition, and r(−) = the number acquiring MRSA in the absence of positives/total bed days when positives were absent. 6 The estimate of r(+) so derived agrees well with the estimate of r(+) derived from those patients during whose stay MRSA patients were present continuously. 6
Each patient admitted from ED with growth of MRSA from admission screens or other site within 48 h was matched with a control of the same age and sex admitted in the same calendar year free of the organism at admission. From hospital records and the Microbiology database, admissions to this hospital in the preceding two years and previous growth of MRSA were determined in the two groups.
Results are expressed as mean ± standard deviation or 95% confidence intervals. Regression analysis and Chi-squared have been used as appropriate. Statistical calculations were performed using Excel (Microsoft) or Casio fx-3600P scientific calculator.
As this study was of results of investigations which were part of normal clinical care, did not require any additional resources, and individual patients cannot be identified, formal ethical approval was not sought.
Results
The number of admissions to ICU each year, the number with positive admission screens or growth of MRSA from any site within 48 h (MRSA+), prevalence (Prev), and 95% confidence interval (CI).

2001–2003 vs. 2004–2006, p = 0.04.
2004–2006 vs. 2007–2009, p < 0.001.
2007–2009 vs. 2010–2012, p = 0.03.
The number of patients (n) and MRSA positives (+) from each source; wards within the hospital (WARDS), the emergency department (ED), from theatres/recovery (Post-Op), and transfers from other hospitals (Hosp).

In the two right hand columns, prevalence and 95% confidence intervals for ward and post-operative patients, P (CI), for each three-year period of the study.
Prevalence in admissions from wards: 2001–2003 vs. 2004-6, p = 0.466; 2004–2006 vs. 2007–2009, p < 0.0001; 2007–2009 vs. 2010–2012, p = 0.008.
Prevalence in postoperative patients: 2001–2003 vs. 2004–2006, p = 0.001; 2004–2006 vs. 2007–2009, p = 0.342; 2007–2009 vs. 2010–2012, p = 0.054.
Prevalence of MRSA infection/colonisation in patients admitted to ICU from within the hospital in relation to the number of days spent in hospital prior to transfer to ICU.
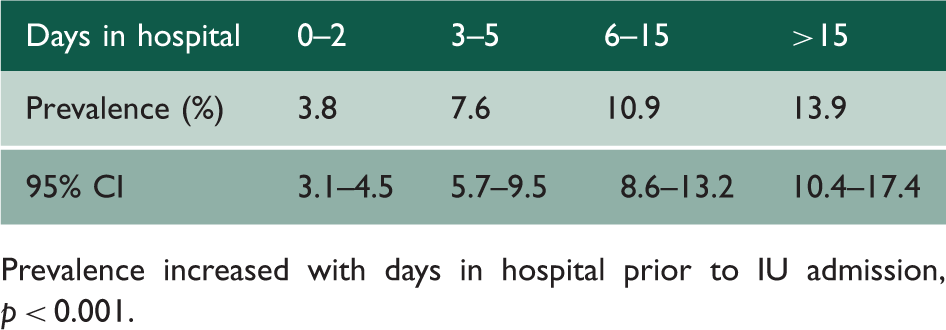
Prevalence increased with days in hospital prior to IU admission, p < 0.001.
Table 2 shows that 78 of 1840 patients admitted to ICU from ED were MRSA positive on arrival. Of these 78, 43 (55.1%, 44.1–67.1) had been an inpatient in this hospital in the preceding two years, compared to 21 of 78 (26.9%, 17.1–36.7) age- and sex-matched patients admitted from ED who were MRSA negative on arrival in ICU, p < 0.001. In 24 of the 78 (30.8%, 20.6–41) MRSA-positive admissions from ED, the organism had been grown during a previous admission, whereas there had been no prior growth of MRSA in the controls, p < 0.0001.
Prevalence of MRSA infection/colonisation in patients admitted to ICU from within the hospital in relation to time in hospital prior to transfer in each three-year period of the study.

0–5 days: 2004–2006 vs. 2007–2009, p < 0.001; 2010–2012 vs. 2007–2009, p = 0.007.
>5 days: 2004–2006 vs. 2007–2009, p < 0.001; 2010–2012 vs. 2007–2009, p = 0.003.
Acquisition of MRSA within ICU by patients initially free of the organism.

Acquired MRSA: the number of patients with no growth of MRSA within 48 h of admission to ICU who subsequently had a positive culture on or after the fifth day in ICU; acquisition rate: the estimated rate of acquisition per thousand bed days and 95% confidence intervals (see ‘Methods’ section for explanation of calculation); acquired MRSA bacteraemia: the number of patients with no growth of MRSA from any site within 48 hours of admission to ICU in whom MRSA was grown from at least one blood culture taken on or after the fifth day in ICU.
Acquisition rate: 2001–2003 vs. 2004–2006, p = 0.888; 2004–2006 vs. 2007–2009, p < 0.0001; 2007–2009 vs. 2010–2012, p < 0.0001.
Of the 201 who acquired MRSA within ICU, 167 did so when at least one known MRSA positive was present in ICU. The estimated rates of acquisition/1000 bed days when positives (imported or acquired) were present and absent were 12.6 (10.7–14.5) and 2.9 (1.9–3.9), respectively; relative risk 4.34 (3.98–4.70), p < 0.001. Table 5 shows that the acquisition rate changed little between 2001 and 2006 but decreased progressively thereafter. The estimated rates of acquisition/1000 bed days when positives were present were 15.1 (14.4–15.8) in 2001–2006 and 6.8 (6.0–7.6) in 2007–2012, p < 0.0001, and the corresponding estimates for when no MRSA positives were present were 5.6 (4.7–6.5) and 2.2 (1.9–2.5), p < 0.006.
Moreover, 41 patients with negative admission screens and no growth of MRSA from any site within 48 hours of admission to ICU subsequently developed MRSA bacteraemia. With one exception, the organism was grown from another site before or at the same time as the first positive blood culture. Table 3 shows only three acquired MRSA bacteraemias since 2006, the most recent in 2009. Overall, 20.4% (14.8–26.0) of those acquiring MRSA in ICU had a bacteraemia; 25% (18.1–31.9) in 2001–2006 and 6.1% (0–12.8) in 2007–2012, p = 0.004.
In all, 17% (16.5–17.5) of available bed days were occupied by known MRSA-positive patients in 2001–2006 and 5.5% (5.2–5.8) in 2007–2012, p < 0.0001. The percentage decreased each year from 2007 to 1.5% (1.3–1.7) in 2012.
Discussion
This study reports a continuing decrease in prevalence of MRSA in admissions to our ICU due largely to fewer positives coming from the hospital wards following the extension of admission and weekly screening with eradication therapy for positives to the whole hospital and improvements in general infection control. There was a parallel reduction in the number of patients acquiring MRSA within the ICU and a larger decrease in ICU-acquired MRSA bacteraemia.
This study has limitations. Without discharge screening the number acquiring MRSA is an underestimate 1 but with a similar proportionate error throughout the study small in comparison to the observed reduction. Without typing, persistent carriage and re-infection cannot be distinguished, a causal relation between presence of positive patients and acquisition is speculative, and changes in predominant strain over the study period cannot be excluded. But analysis of results of cultures taken as part of the normal care of several thousand patients allows long-term analysis of this important problem for no additional cost.
The increase in prevalence of MRSA at arrival in ICU with time in the hospital prior to transfer establishes a strong link between risk of infection/colonisation and exposure to the hospital environment. From 2006, the progressive decrease in the difference in prevalence of MRSA between those spending >5 days and ≤5 days in hospital prior to arrival in ICU demonstrated a continuing reduction in the risk of acquisition of MRSA while on the wards. Although observational studies should be interpreted with caution, the timing and continuance of this decrease suggests that it was consequent upon the new hospital-wide measures.
Late in the study patients coming from the ED, essentially direct admissions from the community became the major source. The MRSA positives in this population had a high incidence of previous hospital admission and prior growth of MRSA. Patients with repeated admissions are an important source. 9
The increased risk of acquiring MRSA in ICU when known positives are present is consistent with the model of transmission whereby positive admissions are the source with spread via transient carriage on the hands of healthcare workers. 10 If the basic reproduction number, the number of new cases arising from each index case, is less than one, stochastic models show that following admission of an MRSA-positive patient, no transmission or single or small clusters of cases will be common but self-perpetuating outbreaks rare. 10 The ratio of new cases to positive admissions is a surrogate for the reproduction number 11 and was <1 in this study. Hence, control of MRSA within ICU was sufficient to prevent self-perpetuation, so persistence of MRSA required high prevalence in admissions.
Fewer positive admissions will result in fewer new cases within ICU. 10 Stochastic models show a wide range of possible outcomes from an initial set of conditions emphasising the need for prolonged observation of small populations. 10 In our preliminary report, we used an estimate of acquisition rate in the presence of known positives as a measure of effectiveness of MRSA control independent of prevalence and found no significant decrease. 6 In this longer study, this measure did decrease, suggesting some contribution from the new measures within ICU. But such was the decrease in the number of bed days occupied by positive patients that presence of more than one was rare so density of exposure decreased, and the practicalities of segregation and cohort nursing became easier. Hence, this may not have been a specific effect. The decrease in acquisition rate in the absence of known positives suggests that as overall infection control improved other means of spread within ICU, such as unidentified positives, carriage on the hands of the many visiting hospital staff and contamination of the inanimate environment also decreased.3,12
Extended observation showed reductions in both the number of MRSA bacteraemias and the proportion of those acquiring MRSA progressing to bacteraemia, the latter an improvement independent of prevalence. The mechanism is uncertain. Better care of lines should reduce bacteraemias caused by many pathogens 13 while daily washing with a bactericidal agent should reduce those where skin contamination is an important precursor. 14 After the new measures, we reported no decrease in bacteraemias due to major pathogens other than MRSA5,15 but growth of coagulase-negative Staphylococcus aureus from fewer blood cultures, 15 suggesting better skin decontamination. 16
The efficacy of screening for MRSA in ICU has been long debated.17–20 A recent study proposes a strategy of decolonisation of all ICU patients without screening, 21 a policy which has received strong support. 22 This study shows that control of MRSA in ICU is critically dependent upon infection control in the whole hospital. The epidemiology of MRSA in hospitals has been of successive waves, 23 so the welcome decrease in MRSA bacteraemias in UK hospitals23,24 does not exclude further waves. Stochastic models show that MRSA can switch abruptly from epidemic to endemic status, 25 and our data suggest that this happened in our hospital at an unknown time prior to 1996. 5 It is salutary that it was 10 years before effective hospital-wide measures were deployed. Modelling predicts that it may take many years to regain control. 25 The improvements reported here follow six years of diligent application of new measures by all hospital departments and has fostered awareness of the importance of infection control. We are unable to estimate the efficacy of each of our additional measures, so premature abandonment of any element of our current policy might risk the return of the unacceptable levels of prevalence and acquisition seen so recently.