
Abstract
Lesson
While well described in text books, acute presentations of hypo-pituitarism are rare and must be considered when patients present with vague symptoms with poor response to standard resuscitation procedures.
Keywords
Case presentation
A 34-year-old woman with a history of polycystic ovarian syndrome self-presented to the emergency department, complaining of malaise, nausea and feeling cold. Her only previous hospital admission was for the birth of her first child one month earlier.
An obstetric history revealed that during the antenatal period, she developed severe headache and was investigated with a magnetic resonance imaging (MRI) brain in the 30th week of her pregnancy. This showed an enlarged pituitary gland with a cranio-caudal length of 12 mm. She was reviewed along with her imaging by the Neurologist, who felt the pituitary enlargement was physiological for her stage of pregnancy and the headache a manifestation of migraine.
She had a difficult vaginal delivery requiring the use of ventouse and forceps for shoulder dystocia with documented blood loss of 500 mL during delivery. Subsequent history from the patient revealed that during the in-hospital post-partum period, she experienced significant fatigue and generalised weakness. Further, the baby was commenced on formula feed due to lactation failure. The general malaise continued upon discharge, her mobility was poor, with muscle weakness and postural dizziness requiring assistance with various activities of daily living. She also noticed involution of her breasts and considerable weight loss of 6 kg from her pre-pregnancy weight. She spent a large proportion of the post-natal period in bed, a considerable change from her previously active lifestyle with hobbies including hiking and rock climbing.
Biochemistry results on admission and one month post-discharge, with local normal reference ranges.
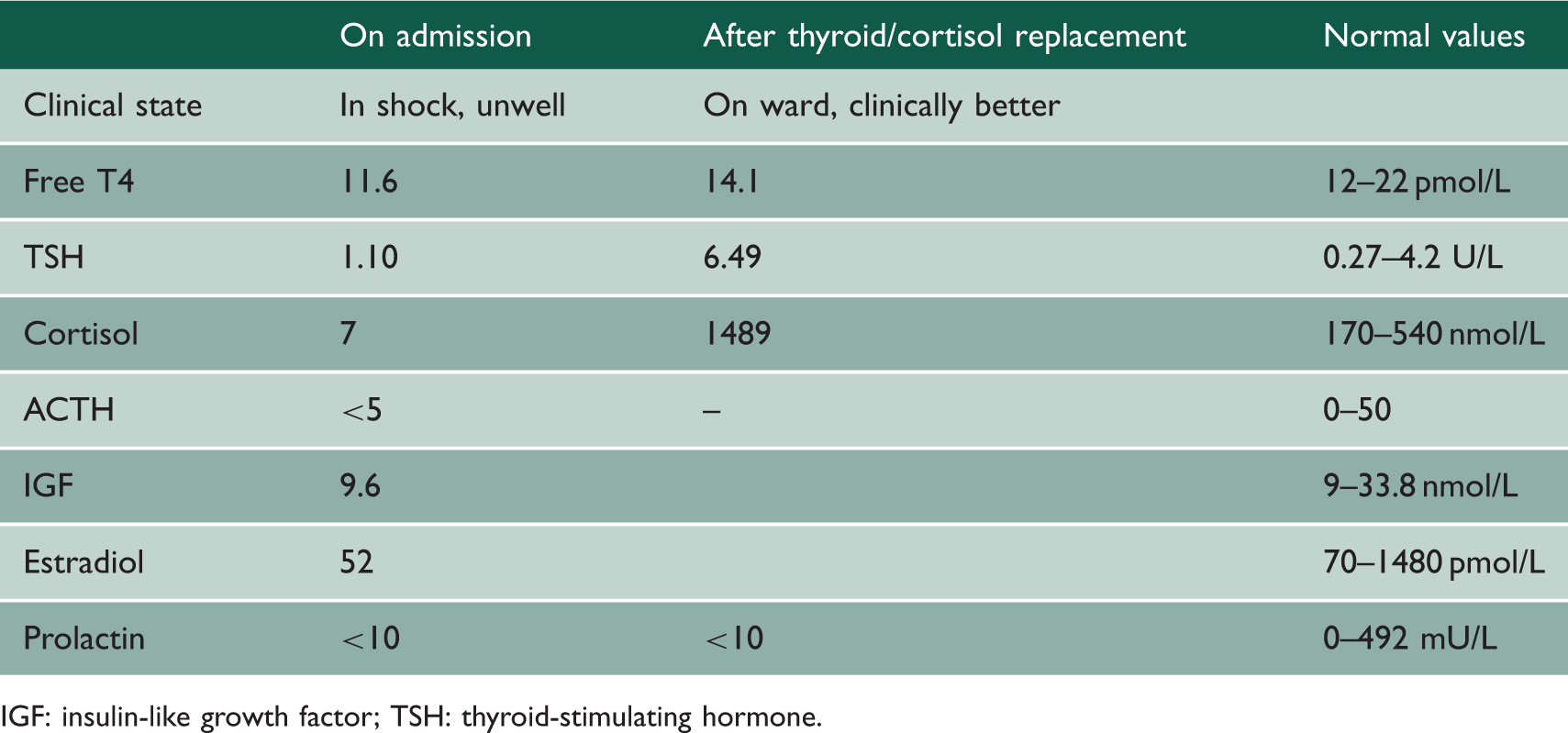
IGF: insulin-like growth factor; TSH: thyroid-stimulating hormone.
Within two days, the patient was fit for discharge and was followed up on an outpatient basis within the endocrine department. Pituitary axis tests performed one month after discharge confirmed an ongoing cortisol deficiency. Low insulin-like growth factor further confirmed hypo-pituitarism. Prolactin remained low throughout the episode – this in itself a strong marker of a destructive process affecting the anterior pituitary. Estradiol was low, suggesting hypo-gonadotropic hypo-pituitarism secondary to pituitary infarction. Expectedly, luteinizing hormone and follicle stimulating hormone were low throughout this episode, and menses had not returned at endocrine outpatient follow-up one month later.
Discussion
Post-partum necrosis of the anterior pituitary was first described in 1937 by Sheehan. 1 While Sheehan’s syndrome is rare in the developed world due to improvements in obstetric care, its prevalence is perhaps higher than expected, estimated at five per 100,000 patients in a recent study. 2
The majority of patients has non-specific problems such as weakness and fatigue and thus go undiagnosed (therefore, untreated) for a many years post-partum. The case described here, with a presentation of acute hypo-pituitarism one month after delivery, is rare. 3 The large variation in the duration between post-partum haemorrhage and clinical manifestation makes this a potentially difficult diagnosis to make. However, severe pituitary insufficiency can result in coma or death, making it imperative for clinicians to recognise and instigate prompt management.
Clinical presentations are varied, with damage to more than 75% of the pituitary gland needed before clinical signs become apparent. 4 Presenting features depend on the precise hormones involved. Growth hormone tends to be affected first and may cause fatigue and altered body composition. 4 ACTH/cortisol deficiency will cause fatigue, weakness, weight loss and low blood pressure. Thyroid-stimulating hormone deficiency will result in a hypo-thyroid state, with fatigue, feeling cold and constipation. Prolactin deficiency will cause problems with lactation. 4
In terms of imaging, as mentioned in the case presentation, this patient’s MRI scan during her pregnancy confirmed enlargement of the pituitary gland. Pituitary enlargement during pregnancy is common due to increased vascularity 5 and may well have contributed to increased susceptibility of the pituitary to infarction in the setting of acute blood loss during labour. Interestingly, when MRI pituitary was performed on this patient one month after presentation, pituitary size was described as normal. An ‘empty sella’ may be the expected MRI findings following pituitary necrosis, but the pituitary often undergoes enlargement followed by gradual shrinkage which can take months to years to appear radiologically. 6
This case highlights the need for thorough assessment in particular with regard to the clinical history and the challenges of recognising the symptoms and signs of acute pan-hypo-pituitarism.