
Abstract
Lesson
Delirium secondary to pneumonia is expected in the elderly, but when persistent and incongruent with expectation, cerebral abscess should be considered.
Case report
A functionally independent 89-year-old woman with a background of hypertension, atrial fibrillation and diverticular disease presented with delirium.
On examination, she was drowsy, pyrexial, tachycardic and desaturating in air. Auscultation revealed an ejection systolic murmur and crepitations in the right lung. Abdominal examination was normal. Neurological examination was unremarkable. Inflammatory markers were raised and chest radiograph revealed consolidation in the right mid-zone. Delirium secondary to community-acquired pneumonia was diagnosed and intravenous teicoplanin and clarithromycin commenced, following hospital guidance for penicillin allergy.
Despite 72 h of treatment, she remained unresponsive and pyrexial, with rising inflammatory markers. Antibiotics were changed to aztreonam and teicoplanin for four days, with linezolid for two days, to which there was a good biochemical response.
Blood cultures on admission (BacT/Alert 3D, Biomerieux) and three subsequently were all negative. Coliforms were isolated from urine. Streptococcus pneumoniae and Legionella pneumophilia serogroup 1 urinary antigens were negative (Alere BinaxNOW®). Transthoracic echocardiogram identified no valvular lesion or vegetation. Due to frailty, a transoesophageal echocardiogram was not considered. On day 8, duplex ultrasound identified deep vein thrombosis in the right calf for which she was anticoagulated with therapeutic dose low-molecular-weight heparin.
Despite good oxygenation and biochemical improvement, our patient’s confusion persisted. Glasgow coma score remained fluctuant, 8–15, and neurological examination revealed right-sided neglect and bilateral up-going plantars. Computed tomography (Figure 1) and diffusion-weighted magnetic resonance imaging of the brain found approximately 30 lesions, up to 20 mm in diameter, characteristic of abscesses throughout the cerebral and cerebellar hemispheres. Subsequently, antibiotics were changed to meropenem 1 g 8 hourly for 44 days and metronidazole 500 mg 8 hourly for 19 days.
Initial computed tomography of the brain showing rim enhancing lesions within the posterior fossa, basal ganglia and throughout the cerebral hemispheres.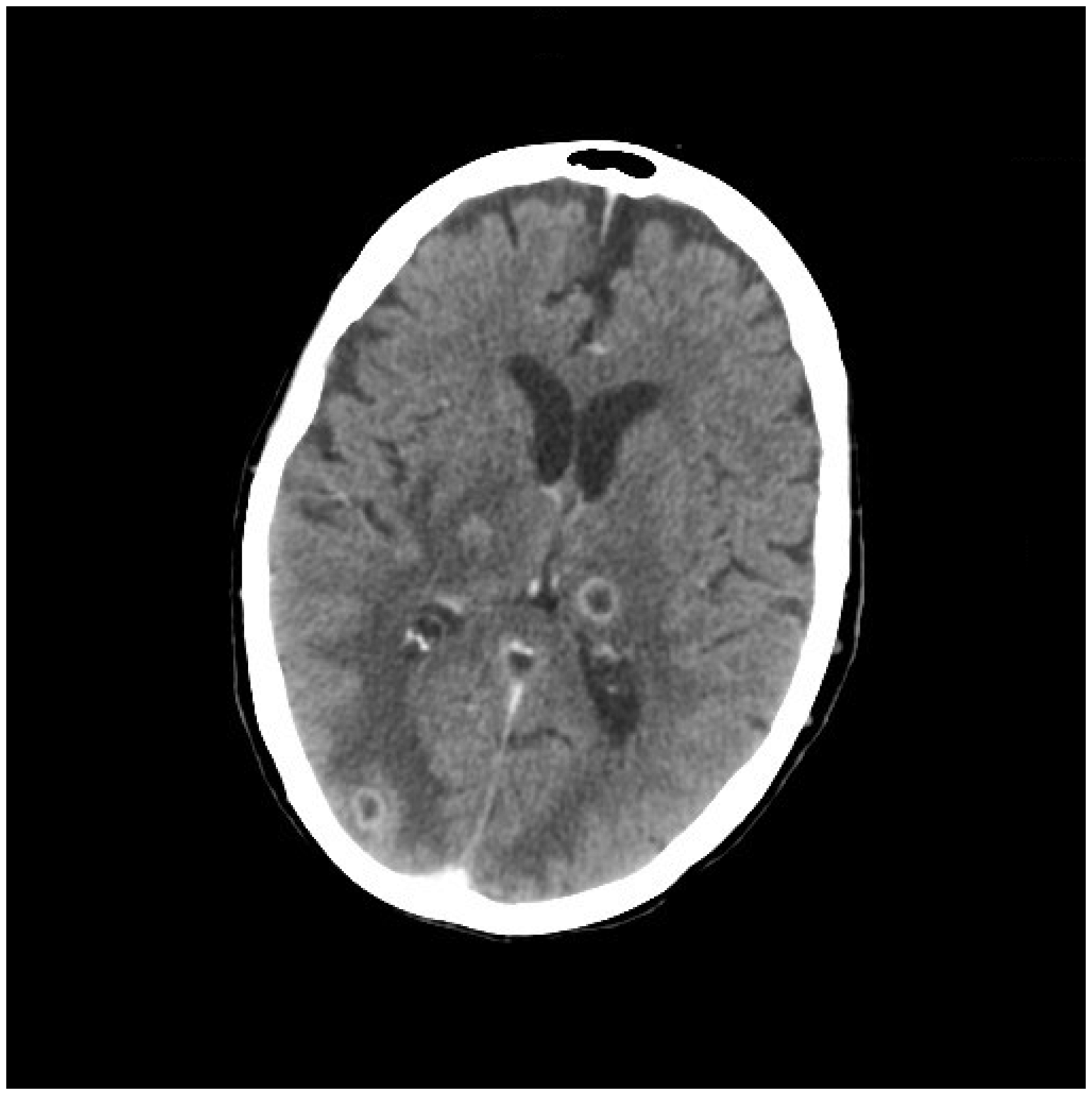
Following discussion with neurosurgeons, it was felt inappropriate to proceed with tissue aspiration due to frailty, anticoagulated state and number of abscesses. Anti-Toxoplasma gondii total immunoglobulin (VIDAS® TOXO Competition) and Hydatid serology were also negative.
Our patient’s clinical condition began to improve from day 20 onwards, with subsequent brain imaging on day 27 showing reduced abscess size with intense rim enhancement.
Although our patient’s sepsis was successfully managed with timely broad spectrum antibiotics, our patient has suffered significant cognitive decline and requires assistance with feeding and personal care which she now receives in a nursing home.
Discussion
Cerebral abscess is a relatively rare diagnosis with significant morbidity and mortality. 1 The majority originates from infection of contiguous cranial structures (40–50%), followed by haematogenous spread from a remote site. Immunosuppression secondary to transplant or chemotherapy also increases risk of infection from atypical organisms. However, in at least 15% of cases, no source can be identified. 2
Pneumonia is a common diagnosis in the elderly; however, the literature reflects the rarity with which cerebral abscesses are a complication. 1 In our patient, the initial focus of sepsis was pulmonary. We believe therefore that haematogenous spread from this site is the most likely route of infection given the diffuse distribution of lesions and lack of other risk factors. In such cases, the most frequently isolated microorganisms are streptococci and staphylococci species.3–5
Conservative management of cerebral abscesses carries a higher risk of mortality over neurosurgical intervention; however, success has been seen with early initiation of treatment.3,6 Guidance for the duration of treatment remains limited, with four to six weeks’ intravenous antibiotics widely considered appropriate when the organism is unknown. 3 Serious complications include intraventricular rupture, with survivors at increased risk of recurrence, and neurological sequelae including hemiparesis, cognitive dysfunction and 30–50% risk of seizure. 7
Conclusion
Many elderly patients who present with pneumonia and delirium might have features of reduced conscious level, pyrexia and headache, which are consistent also with cerebral abscess. Although there is no indication to consider brain imaging in the short term, should the confusion persist despite appropriate therapy, cerebral abscess should be considered and investigated appropriately.
Key points
Cerebral abscess originating from a distant site is extremely rare. Pulmonary infection is common, with which delirium is also a common complication in the elderly. In cases where delirium is out of keeping with the clinical picture, brain imaging should be considered to investigate other causes.