
Abstract
Objectives
To explore the possibility of pathological change in the common carotid artery at the bifurcation and in the internal carotid artery beyond the bifurcation which could contribute to a reduced diastolic pressure as observed in primary open angle glaucoma.
Design
Duplex ultrasonic examinations of carotid bifurcations were conducted on 80 patients. Carotid artery defects were allocated into three types: no demonstrable flow defects, internal carotid artery abnormalities and disease in the carotid bulb.
Setting
Bristol Royal Infirmary Vascular Laboratory.
Participants
Eighty patients (mean age 69.6 years) providing a total of 160 sides to the analysis.
Main outcome measures
An estimated central retinal artery pressure, intraocular pressure and field loss were recorded for each side measured.
Results
Doppler investigations revealed significant levels of pathological change in the internal carotid distinct from changes at the carotid bulb. The disease revealed in the internal carotid artery was significantly associated with intraocular pressure (p = 0.032), with an effect small to medium in magnitude. The Q2 measure, derived from mean arterial pressure and intraocular pressure, was also substantively associated with disease in the internal carotid artery. Both intraocular pressure and the Q2 measure effectively discriminated between groups, with field loss providing rather less discriminating capability. There was a strong trend towards a higher intraocular pressures and a greater visual field loss with internal carotid artery disease.
Conclusions
Pathological changes in the extra cranial carotid artery in primary open angle glaucoma exceed those in the arteries classified as normal. The presence of disease specifically in the internal carotid artery emphasised the need for a mechanism for the evaluation of the internal carotid apart from the carotid bulb. A basis for clarifying the presence of an ischaemic zone is proposed.
Introduction
von Graefe 1 set out diagnostic features of what now known as primary open angle glaucoma – (POAG): raised intraocular pressure in the eye (IOP), optic atrophy with cupping at the papilla, nasal displacement of the vessels on the optic disc and evidence of a reduced pressure in the central retinal artery (CRA). The latter was seen as either a spontaneous diastolic pulse or a pulse elicited by slight pressure on the globe. These observations on the CRA were subsequently reaffirmed.2,3
A method for the measurement of pressure in the CRA using a spring-loaded instrument called an ophthalmodynamometer 4 drew attention to several features of CRA pressure. It was found that an artificial increase in carotid blood pressure did not produce an increase in IOP, and there was no association between systemic hypertension and IOP. Subsequently, 5 the lower diastolic retinal artery pressure (RAP) was established as a constant feature of POAG. Wieglin and Lobstein 6 amplified the method, demonstrating a consistent ratio between the RAPs and those measured at the brachial artery. They provided tables to adjust the CRA readings to allow for the effect of IOP on repeated measurements of CRA pressures, calculating the ratio of the CRA pressure (ophthalmic artery pressure) to the ipsilateral brachial artery pressure to be 63%. Their level differs from calculations of Reese and McGavic 7 who calculated the ratio to be 75% of the brachial artery pressure. They reported lower CRA pressures in POAG, but found these not to be as consistent as in Amaurosis fugax (AF). 6 Reese and McGavic also concluded that the majority of carotid lesions were in the extra cranial portion of the carotid artery.
The issue of a disparity between the IOP and a lower mean ophthalmic artery pressure was addressed by Lobstein 8 who concluded that ‘the most unfavourable contingency occurs when the pressures, IOP and CRA, come close to one another’. This is termed an efficient gradient.
The ability to study the pathological changes in the carotid artery was first advanced by radiological assessment of the carotid bifurcation. This revealed that the bifurcation had particular relevance to AF and strokes. Doppler ultrasonic investigations into blood flow followed, and with the advent of duplex scanning the ability to visualise the vessel wall at the carotid bifurcation and analyse any pathological change. 9 This can be supplemented by the measurement of resistance indices and velocity. Routine duplex Doppler ultrasound clarifies various aspects of flow in the three carotid vessels, the common carotid and the external and internal carotid vessels. Subsequently, duplex scanning has become the accepted standard investigation. 5 This was applied to POAG. 10
Vascular factors in the pathogenesis of POAG have been investigated6,8,10–15 demonstrating increased resistance and decreased blood flow in the extra cranial carotid artery. Other aspects of carotid artery flow such as elasticity and the baroreceptor reflex in the carotid, 16 and blood pressure and perfusion pressure decreases 15 can indicate reduced flow.
An important feature demonstrated when the IOP is measured is the presence of a transmitted pulse wave, increasing in amplitude as pressure is raised to 40 mmHg, and then declining rapidly. This offers a ‘cut off’ point. As mentioned by Baillart, 5 the pressure level in the central retinal vein is relevant. Currently there is no satisfactory form of clinical measurement of venous pressure and its contribution to optic disc capillary blood flow.
Lower mean CRA pressures have been consistently demonstrated in AF 17 : a condition not associated with raised IOP nor optic atrophy or cupping of the optic disc, although it can be associated with field loss. The combination of carotid artery abnormalities in POAG 12 and a lower diastolic pressure prompted an extended investigation.
Materials and methods
A study was initiated to explore the possibility of pathological change in the common carotid artery at the bifurcation and in the internal carotid artery beyond the bifurcation which could contribute to a reduced diastolic CRA pressure as observed in POAG, utilising duplex Doppler ultrasonography in eighty randomly selected cases of POAG. This study was supported by a research grant from the Special Trustees of the Bristol Royal Infirmary.
The non-invasive nature of the test and its purpose was explained to the patients before their consent was obtained. The IOPs reported were those found at diagnosis, before treatment. Cases of low tension glaucoma were excluded. Visual fields, tested on the Friedman visual field analyser, were those at diagnosis and compared with subsequent field tests for consistency. The technique of Esterman 18 was used to quantify the degree of field loss, with Grade 1 corresponding to 0–25% loss, Grade 2 corresponding to 26–50% loss, Grade 3 corresponding to 51–74% loss and Grade 4 corresponding to 75% loss or more.
Figure 1 illustrates a duplex scan of the carotid bifurcation showing callipers, enabling measurements of the wall thickness and narrowing of the lumen.
Duplex scan of the carotid bifurcation.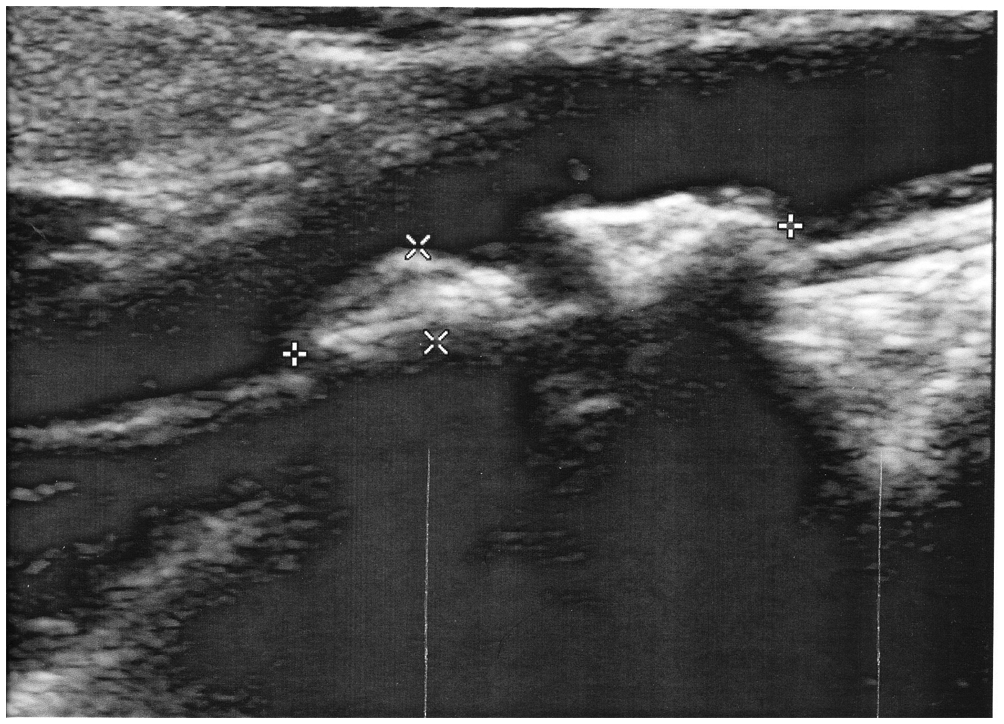
Ultrasonic examinations of the carotid bifurcations were undertaken at the vascular laboratory at Bristol Royal Infirmary in a temperature controlled room in a semi-recumbent position. After the patient had been rested for a short period, brachial artery blood pressure was measured, and from this the mean arterial pressure (MAP) was calculated and adjusted to represent the CRA pressures using the expression: (75% MAP–IOP), derived by Reese and McGavic. 7 This quantity was recorded as Q2.
Both carotid bifurcations were routinely examined, normally the right first. Bifurcations were classified on the basis of the observed form of the vessels and supplemented by flow measurements within all three vessels. An adjustable range gated 7.5 MHz Doppler probe was used to determine flow and resistance indices. This can sample centrally in the vessel lumen or close to the vessel wall.
The three sites where measurements were made were the common carotid below the bifurcation, the internal carotid beyond the bifurcation and the external carotid just beyond the bifurcation. Using the B mode of the duplex system, a classification was made of structural changes at the carotid bifurcation to determine any narrowing and change in vessel wall structure such as intimal thickness, vacuolation without or with fatty deposits and calcification.
Doppler flow measurements were made to determine the effect of any structural change and aided the categorisation of the bifurcation bulb defects. Flow in the internal carotid artery was assessed at the commencement of the vessel. An increased resistance was indicated by turbulence or abnormal readings. Objective measurements of turbulence were obtained from measurements taken from experienced ultrasonographers using the pulsatility index with supporting evidence from the Pourcelot index. Remaining cases were graded as normal.
The carotid artery defects were allocated into three types: Group 1 (those with no demonstrable flow defects); Group 2 (those with internal carotid artery abnormalities defined by increased resistance indices and turbulence, independent of the bifurcation); Group 3 (those with disease in the carotid bulb). A limit was set for this group to show greater than 25% occlusion of the vessel in the region of the bulb before being graded as Group 3.
For Group 2 defects, it would be expected that the altered resistance levels measured by the pulsatility index were greater than in the carotid bulb. Normal defects were so characterised using Doppler ultrasound records at Bristol Royal Infirmary to provide an upper limit based primarily on pulsatility index levels.
During examination, an abrupt cessation of diastole was observed on several occasions. A similar event can also be demonstrated in the CRA and the supra trochlear. The particular feature of this is a sharp systolic rise. Premature cessation of diastole indicates a diastolic event, suggesting an abnormal rigidity. 19
IOPs were recorded by the Goldman applanation tonometer. The significance of the estimated retinal (ophthalmic) artery pressure was examined in two ways. The formula of Reese and McGavic 7 of 75% of the MAP brachial artery was used to postulate the potential RAP. This was then recalculated once the individual IOPs had been deducted and reported as Q2.
Data analysis
Statistical analyses were undertaken using IBM SPSS (Version 20.0). Age profiles and outcomes were summarised descriptively. Univariate analyses of variance (ANOVA) were conducted on the data utilising the Q2, IOP and field loss variables to assess the effect of grouping on these measures. Field loss was modelled alternatively as both a categorical and interval variable due to the regularity of the category widths. An additional multivariate ANOVA (MANOVA) was conducted on the data to assess the effect of grouping on the above variables considered jointly. Follow-up univariate analyses and discriminant function analyses were also conducted as part of this procedure.
Results
Age profiles of duplex Doppler carotid artery studies in POAG.

Sixty-one sides (38.1%) were classified as Group 1, 43 sides (26.9%) were classified as Group 2 and 56 sides (35.0%) were classified as Group 3. Thus, 61.9% of cases were shown to have recognisable carotid artery pathology.
Symmetrical lesions, right and left, occurred bilaterally in 18 instances amongst patients classified as Group 1 (53.6%), in 13 instances amongst patients classified as Group 2 (52.4%) and in 17 instances amongst patients classified as Group 3 (54.8%).
Summary of outcome measures in the three study groups (mean (SD)).

All Q2 readings fell within a range of 32.05 mmHg to 87.25 mmHg. Values in Group 2 were generally lower than either Groups 1 or 3. Analysis of the Q2 variable revealed a trend towards lower mean pressures in Group 2 than in the other groups. Q2 values in Group 2 were skewed towards the lower end of the range, with 17 sides (40.4%) recorded under 50 mmHg, and only four sides (9.5%) recorded over 70 mmHg. By contrast in Group 1, 13 sides (22.0%) recorded under 50 mmHg and eight sides (13.5%) over 70 mmHg. In Group 3, 17 sides (30.9%) recorded under 50 mmHg, and 10 sides (18.1%) recorded over 70 mmHg.
A univariate one factor ANOVA conducted on the data using the Q2 as a test variable determined that values across the three groups were not significantly different at the 5% significance level (F2,157 = 2.87, p = 0.060). However, the p-value obtained indicates a degree of substantive significance of association, with a small effect (partial-η2 = 0.035). Post hoc analysis using Tukey’s honestly significant difference (HSD) test indicated that the significance was grounded primarily in differences between Group 1 and Group 2 sides, (p = 0.053, 95% confidence interval (−0.058, 11.2)). Other comparisons did not yield substantive or significant associations with respect to this outcome measure.
A univariate one factor ANOVA conducted on the data using the IOP as a test variable determined that values across the three groups were significantly different at the 5% significance level (F2,157 = 3.51, p = 0.032), with a small effect (partial-η2 = 0.043). Post hoc analysis using Tukey’s HSD test indicated that the significance was grounded primarily in differences between Group 1 and Group 2 (p = 0.046, 95% confidence interval (0.050, 6.55)). A substantive difference in IOP values between Groups 1 and 3 was also observed using Tukey’s HSD test (p = 0.098, 95% confidence interval (−0.37, 5.67)).
A univariate ANOVA conducted on the data using field loss readings (considered to approximate to an interval variable) determined that field loss across the three groups was not significantly different at the 5% significance level (F2,157) = 2.14, p = 0.122). However, a χ2 test for association between field loss (considered as a categorical factor) and group indicated evidence for a significant association at the 5% level (χ2(6) = 13.1, p = 0.041), with a small to medium effect (Cramer’s V = 0.203).
For both the IOP and Q2 variables, the findings indicated the presence of two homogenous subsets. Groups 1 and 2 are distinct: Group 3 may be effectively grouped with either Group 1 or Group 2. No homogeneous subsets were created with respect to the Field Loss variable.
Significant correlations of moderate strength were found to exist between IOP and field loss values (r = 0.360, p < 0.001), and between IOP and Q2 values, in which a negative association was observed (r = −0.329, p < 0.001): suggesting the requirement for a multivariate analysis. A multivariate analysis of variance (MANOVA) conducted on the Q2, IOP and field loss variables determined that these variables assessed jointly across the three groups were significantly different at the 5% significance level (Wilk’s Λ = 0.920, F6,310 = 2.19, p = 0.043). Individual follow-up univariate ANOVAs gave rise to p-values associated with the individual variables similar in magnitude to those derived in the univariate analysis above.
The MANOVA was also followed up with discriminant analysis, revealing a primary discriminant function which explained 77.4% of model variance (canonical R2 = 0.062). A second discriminant function did not significantly differentiate between groups. All variables loaded fairly highly on the primary discriminant function, with loadings similar in magnitude for IOP (0.74) and Q2 (−0.73), and a somewhat smaller loading for field loss (0.63). Hence the analysis confirms that both IOP and Q2 may effectively discriminate between the groups, with field loss discriminating rather less effectively.
Discussion
A significant level of bifurcation carotid pathology is revealed from the Duplex Doppler examinations in this study. The level for the combined Groups 2 and 3 is 61.9%: 38.1% were graded as no definitive defect. The incidence of 26.9% in Group 2 indicates the need to identify lesions in the internal carotid and to differentiate this from the pathological changes present in the carotid bulb. The presence of a small proportion of Group 1 showing an MAP below 50 mmHg indicates that it also contains an at risk sector, whether defined as an efficient gradient or an ischaemic zone.
Statistically the three groups have been shown to have distinguishing features. Group 2 differs from Group 1 on the basis of IOP at the 5% level (p = 0.046) and has a higher level of field loss. Group 3 is closer to Group 1 than Group 2 in all three outcome measures, though the difference with respect to IOP is small. These outcomes provide evidence that the groups are not the same, justifying their segregation. The prime bases for segregation are IOP and Q2. When considered as a categorical variant, group is significantly associated with field loss at the 5% level: it is not significant if field loss is treated as an interval-level variable. The effect of sizes associated with all comparisons of significant or substantive differences are small to medium in magnitude.
The importance derived from the linkage of IOP and the MAP, recorded here as Q2, is that it defines the original observations of von Graefe. 1 It provides a clearer basis for Baillart’s 5 observation of a lower CRA pressure in POAG, and links with Lobstein’s 8 efficiency gradient. Had the 63% level of brachial artery pressure been applied in this study, the prevalence of a gradient or quotient would have been much higher. A consequence of this might have been reflected in the clarification of field loss in the three groups.
The nature of changes in the carotid bulb, Group 3, coincide with similar lesions found in AF though not as markedly advanced: none came up towards the 75% occlusion level and the proportion between 50% and 75% would be expected to be greater in AF. There was no overt difference in terms of observed vacuolation or calcification between AF and POAG.
With the range of MAPs across all the groups between 32.05 mmHg and 50 mmHg, the overlap is readily seen, as 40.4% of Group 2 have MAPs below 50 mmHg, and therefore a diastolic level approaching the mean IOP at 27.4 mmHg, displaying the potential for an ischaemic zone more than Group 1 or Group 3. A reduced arterial pressure will lead to a reduced velocity in the optic disc capillaries. This would be reduced further through the differing arterial resistances between the three groups: this resistance index characteristically defines Group 2. A refinement of the technique by which resistance is calculated could help to clarify its role where lower MAPs are present in Groups 1 (22%) and 3 (30.9%).
Any untoward rise in IOP will also adversely affect venous drainage at the optic disc, there is currently no clinical means by which pressure in the central retinal vein can be measured. An increased vascular resistance in the arterial ‘loop’ could be reflected in the central retinal vein increasing, along with the IOP, the efficiency gradient in the optic disc capillaries.
The findings in this study provide an explanation for the original observations of Marmion and Aldoori. 17 One aspect of arterial disease in the orbit is the known association of exfoliation syndrome with arteriosclerotic disease in the conjunctival vessels and the vortex veins,20–23 providing a statistically significant association between pseudoexfoliation and angina, hypertension and cardiac infarction. A significantly lower flow mediated vasodilatation (p = 0.01) was found 24 in pseudoexfoliation syndrome.
Another study 25 did not find an association between pseudoexfoliation and coronary disease, aortic aneurisms or peripheral arterial disease. The presence of pathological change in small vessels in the eye and orbit adds weight to the importance of differentiating between the pathological changes seen in the carotid bulb which are more in conformity with atheroma 26 and potential arteriosclerotic changes in the internal carotid artery.
Conclusions
Pathological changes in the extra cranial carotid artery in POAG exceed the arteries classified as normal. The presence of disease specifically in the internal carotid artery at 26.9% emphasises the need for a mechanism for the evaluation of the internal carotid apart from the carotid bulb. A basis for clarifying the presence of an ischaemic zone is proposed.