
Abstract
A type VI acromioclavicular joint injury with a supracoracoid location of the distal end of the clavicle (VIa) may be associated with low energy injuries and, in association with a clavicle fracture, can successfully be treated with reduction of the dislocation, fixation of the clavicle, and may not require reconstruction of the acromioclavicular ligaments. An infracoracoid location (VIb) is highly suggestive of a higher energy injury.
Introduction
We report a rare injury of the acromioclavicular joint with ipsilateral clavicle fracture and discuss subclassification of type VI injuries.
Case report
A 40-year-old woman presented with persistent right shoulder pain and a clavicle fracture following a fall down stairs three weeks previously. The exact mechanism of the injury was unclear, but it was thought she had held onto the bannister as she fell pulling her right arm into extreme abduction and external rotation.
Prior to our review, she had attended two separate Emergency Departments complaining of persistent pain at the fracture site and in the shoulder. She also reported intermittent paraesthesia of her right hand with occasional, transient blue or white discolouration of her right arm. Both Emergency Departments had diagnosed a mid-shaft clavicle fracture and a fracture of the posterior aspect of the right third rib, but neither had appreciated the dislocation of the acromioclavicular joint (Figure 1).
Anteroposterior view showing a fracture of the right clavicle and third rib with inferior dislocation of the acromioclavicular joint (at initial presentation).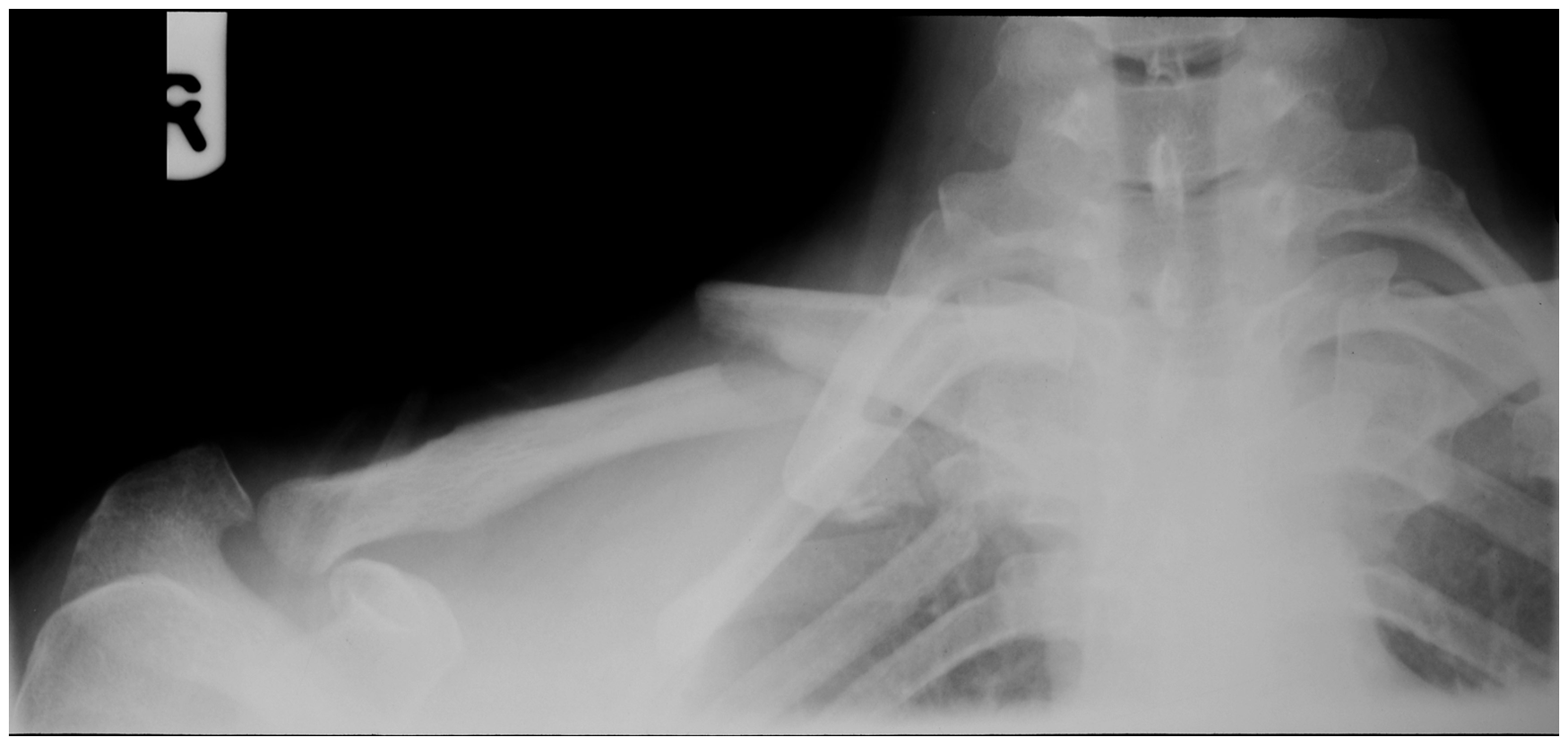
Following diagnosis of the type VI injury, she was offered operative reduction of the dislocation and plate fixation of the clavicular fracture. This was performed 10 weeks following the injury; at operation, early callous was present at the fracture site, and the inferiorly dislocated distal end of the clavicle was found to be encased in scar tissue. The scar tissue was excised and the fracture reduced. With this, the distal end of the clavicle reduced anatomically onto the acromion. Following fracture reduction, the acromioclavicular joint was found to be stable intra-operatively. The clavicular fracture was held reduced with a six-hole reconstruction plate and lag screw. Iliac crest autograft was applied to the fracture site.
Post-operatively, the intermittent paraesthesia and arm discolouration resolved. At nine-month follow-up, she had regained a full and pain-free range of movement of the right shoulder. Radiographs revealed fracture union with normal alignment of the acromioclavicular joint (Figure 2). She was discharged from further follow-up.
Nine-month follow-up radiograph showing anatomically reduced acromioclavicular joint with healed clavicle shaft fracture and plate in situ.
Discussion
Injuries to the acromioclavicular joint are common. They are usually caused by a fall onto the point of the shoulder with the arm in adduction. In 1984, Rockwood 1 updated Tossy and Allman’s classification of acromioclavicular dislocations to include six categories of increasing severity.
Type VI injuries are characterised by inferior displacement of the clavicle; the distal end of which lies in either a subacromial or subcoracoid position. They are rare injuries and have been postulated to be caused by extreme abduction, external rotation and retraction of the scapula, which tears the acromioclavicular and coracoclavicular ligaments. However, in the subacromial variety, the coracoclavicular ligaments have been found to be intact. 2
They usually occur in high-energy accidents and may be associated with concurrent head injuries, 3 other fractures (including rib fractures), 4 abdominal bleeding 5 or pneumo- or haemothoraces. There can also be an associated brachial plexus injury.
Type VI acromioclavicular joint injuries are rare. A search of the literature has revealed just three previously reported subacromial supracoracoid dislocation with associated clavicular fracture.6–8
Koka and D’Arcy 6 noted that the injury had been missed on initial presentation. They stated: ‘Subacromial dislocation of the outer end of the clavicle with an associated fracture is rare and can easily be overlooked unless careful attention is paid to the initial radiographs’. 6 We would concur with this opinion.
Due to the nature of this type of dislocation, the integrity of the coracoclavicular ligaments is not a concern, thus following reduction and fixation of the clavicle, stability of the acromioclavicular joint may be satisfactory. In contrast, subcoracoid dislocations have often been found to be associated with disruption of the coracoclavicular ligaments, requiring their reconstruction.3–5,9–12
Reports of neurological symptoms with type VI subcoracoid acromioclavicular joint dislocations are quite common. Four previously reported cases had neurological symptoms, mainly in the distribution of the upper part of the brachial plexus.3,4,11,13 Two of these cases also had associated ipsilateral clavicle fractures. There are, however, no previous reports of type VI dislocations being associated with vascular symptoms or of subacromial supracoracoid dislocations having neurological symptoms. Our patient complained of intermittent paraesthesia of her right hand and transient blue or white discolouration of her right arm. Although these symptoms were not investigated at the time on the basis of normal neurovascular clinical examination, they fully resolved following surgery suggesting that the symptoms were the result of direct pressure. 3
It is our opinion that subacromial supracoracoid dislocations are quite different from subcoracoid dislocations. The latter are almost invariably associated with high-velocity accidents and have other significant injuries. They are associated with disruption of the coracoclavicular ligaments, and therefore operative procedures need to address this anatomical deficiency. Subacromial supracoracoid dislocations, however, are associated with lower velocity accidents and less severe concomitant injuries. In addition, the coracoclavicular ligaments remain intact.
Due to these differences, we feel that subclassification of type VI acromioclavicular joint dislocations into type VIa (subacromial, supracoracoid) and VIb (subcoracoid) dislocations would be clinically useful, as previously suggested by Juhn and Simonian 7 and supported by Grossi and Macedo. 8
Conclusion
In conclusion, type VI subacromial supracoracoid dislocation of the acromioclavicular joint is a rare injury and should be subclassified as type VIa. Delayed diagnosis is likely if careful examination of the patient’s radiographs is not performed. In addition, reassessment of the radiographs should always be undertaken in any patient with a clavicular fracture who has neurovascular symptoms in the ipsilateral arm. Once identified, even if the diagnosis is delayed, surgical treatment can be expected to give a good outcome.