
Abstract
Through the detection of acute inflammation, edema, and fibrosis, cardiac magnetic resonance imaging provides a complete and safe evaluation of the myocardium in Churg-Strauss disease and is a useful tool for following the disease course.
Introduction
Churg-Strauss is a vasculitis of the small and medium sized arteries described in 1951 by Drs. Jacob Churg and Lotte Strauss. 1 It can affect any organ system, but commonly involves the lung and skin. The 1990 American College of Rheumatology criteria for the classification of Churg-Strauss Syndrome requires at least four of the following six criteria: asthma, eosinophilia >10%, mononeuritis or polyneuritis, non-fixed pulmonary infiltrates, paranasal sinus abnormality and extravascular eosinophils. 2 It is a rare condition with an estimated annual incidence of 1.0 to 4.2 people per million. 3
The management and prognosis of Churg-Strauss patients depend upon organ involvement and severity. Guillevin et al. 4 developed a ‘Factor Five Score’ to more precisely determine prognostic factors and aid in the treatment of patients. Their results demonstrated that patients presenting with proteinuria, renal insufficiency, gastrointestinal tract involvement, cardiomyopathy or neurologic involvement have a poorer prognosis needing more aggressive treatment. 4
Cardiac involvement associated with Churg-Strauss is considered one of the most serious manifestations accounting for approximately one-half of deaths. In a study by Neumann et al., 5 49 patients with Churg-Strauss were examined for evidence of cardiac involvement. Of these, 22 had evidence based on electrocardiogram, echocardiogram and cardiac magnetic resonance imaging (cMRI). Common findings included valvular insufficiency, pericardial effusions and heart failure. Endomyocardial involvement was found in 12 patients, representing a severe form of cardiac involvement.
Because of the high rate of mortality from cardiac involvement, early diagnosis is critical. cMRI is an important tool to determine the extent of cardiac involvement in Churg-Strauss, allowing for earlier and more aggressive therapy. We describe a patient who presented with Churg-Strauss and cardiac involvement, presenting important cMRI findings associated with this disease and its utility in following disease progression.
Case presentation
A 32-year-old white man presented to our emergency department with the primary complaint of one week of numbness and tingling in both hands. He also noted purple lesions on his hands and feet for two weeks, diffuse migratory arthralgias, watery diarrhoea and a 10-pound weight loss over two months. His medical history included asthma, allergic rhinitis and mitral valve prolapse with regurgitation.
On physical examination he was normotensive with a regular heart rhythm and rate. His temperature was 100.0°F. Cardiac findings included a grade III holosystolic murmur at the apex with radiation to the left axilla. Chest examination revealed decreased breath sounds in the right lower lung field. Dermatologic examination demonstrated warm and dry, erythematous non-tender macules that were 0.5–1.0 cm in diameter covering 5–10% of his palms, the dorsum and soles of the feet and the ankles and shins. The neurologic examination was unremarkable. Laboratory analysis was significant for a white blood cell count of 27,100 WBC/uL (normal 4500–10,000) with 69% eosinophils (normal 0.4–7.5%) and an elevated total creatinine kinase level of 438 Units/L (normal 30–300), CKMB of 30 ng/mL (normal <6.0), and troponin I of 5.5 ng/mL (normal <0.05). The C-reactive protein (CRP) level was 71.2 mg/L (normal 0–10) and the rheumatoid factor was 23 IU/mL (normal 0–15). The patient’s sedimentation rate was normal and his ANCA was negative. Chest X-ray demonstrated a right pleural effusion and borderline pulmonary vascular congestion. Electrocardiogram revealed normal sinus rhythm with left atrial abnormality and non-specific T wave abnormalities.
Given the patient’s presentation with a history of asthma and allergic rhinitis symptoms, vasculitic rash with hypereosinophilia, intermittent fevers, weight loss, elevated CRP and positive rheumatoid factor, the diagnosis of Churg-Strauss was made. He was admitted to the hospital and started on prednisone 0.5 mg/kg twice daily. An echocardiogram demonstrated normal biventricular size and function with mitral valve prolapse and moderate regurgitation. A cardiac catheterization demonstrated no significant coronary artery disease. A ventriculogram demonstrated three diverticuli extending from the left ventricular cavity at the anterolateral, anterobasal and apical walls. A cMRI revealed severe mitral regurgitation and extensive endomyocardial delayed enhancement of left ventricle consistent with myocardial involvement (Figure 1).
Baseline cardiac MRI with myocardial edema and fibrosis and follow-up cardiac MRI with persistent fibrosis. Baseline cardiac MRI: (a) Short-axis T2-weighted view of the mid-left ventricle at the level of the papillary muscles; (b) short-axis dark blood T2-weighted fast spin echo images through the mid left ventricle revealing hyperintense signal (white arrow) consistent with myocardial edema; (c) short-axis phase-sensitive T1-weighted (PSIR) images of the mid-left ventricle revealing myocardial delayed enhancement (white arrow) of the same region; (d) two-chamber PSIR images with fibrosis (white arrow). Follow-up cardiac MRI: (e) Short-axis T2-weighted view of the mid left ventricle at the level of the papillary muscles; (f) Short-axis dark blood T2-weighted fast spin echo images through the mid-left ventricle with resolution of myocardial edema; (g) short-axis PSIR images of the mid left ventricle with persistent fibrosis (white arrow); (h) two-chamber PSIR images with fibrosis (white arrows). (Images courtesy of Mark Lawson, MD, Director of Cardiac MRI Lab, Vanderbilt University, Nashville, TN.) MRI = magnetic resonance imaging; PSIR = phase-sensitive T1-weighted.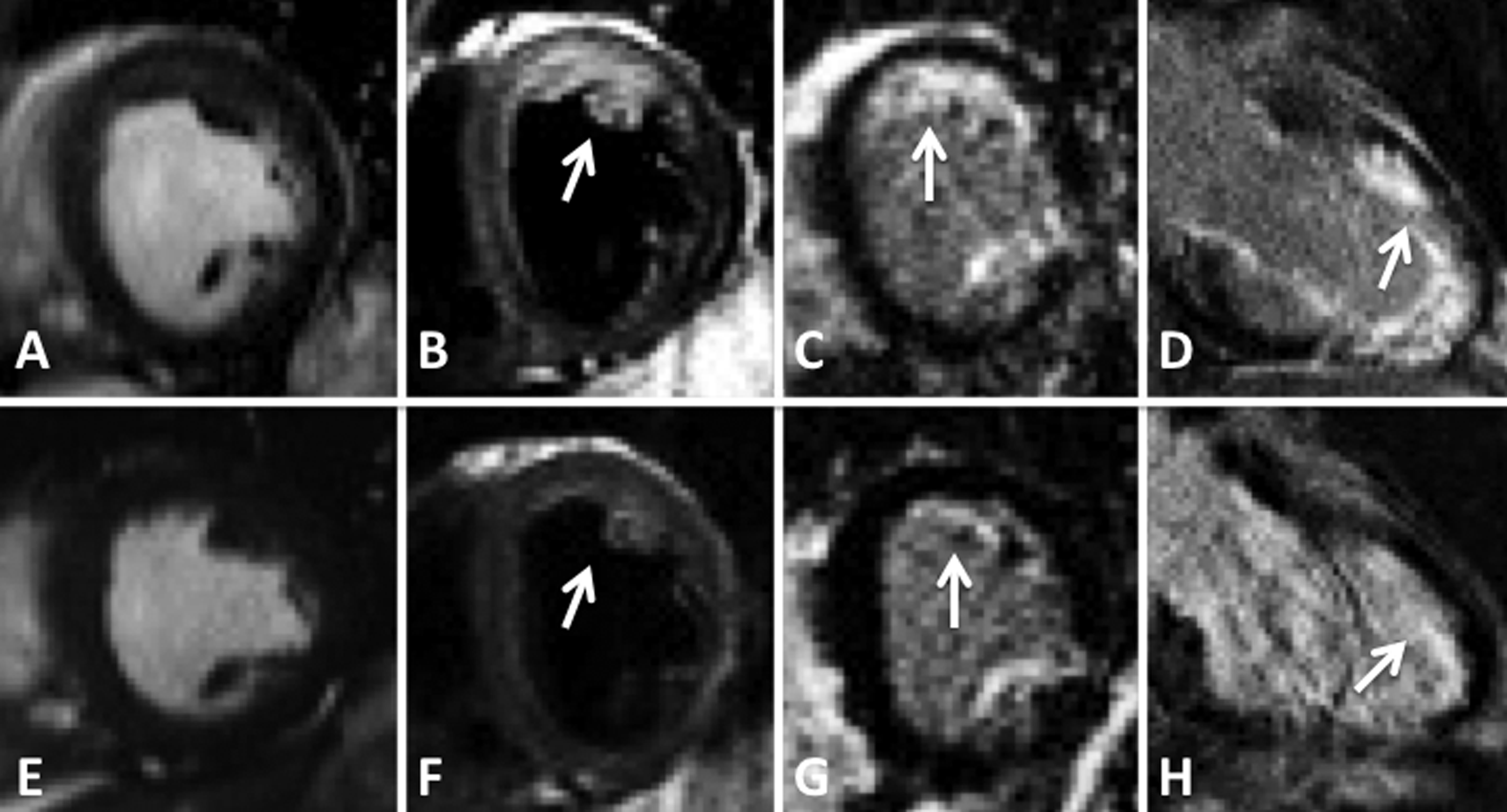
By day three of hospitalization, his clinical symptoms improved. He was discharged on day five with 40 mg prednisone twice daily. He returned for a follow-up visit 11 days after his initial presentation with improvement in his dermatologic findings, normalization of his white blood cell count, and resolution of his eosinophilia. He has continued to do well on low-dose prednisone. A repeat cMRI obtained nine months after his presentation demonstrated an unchanged distribution of myocardial fibrosis but resolution of myocardial edema on T2 imaging (Figure 1).
Discussion
This is an example of Churg-Strauss disease with cardiac involvement. There are many ways to evaluate cardiac involvement including echocardiogram, endomyocardial biopsy and cMRI. Of these modalities, cMRI provides a complete and safe evaluation of the myocardium.
Cardiac MRI is a sensitive test for the detection of pericardial effusion, valvular regurgitation, thrombus formation and disruption of myocardial architecture, particularly in the setting of myocarditis, myocardial infiltration and infarction. 5 In those with echocardiographic abnormalities, cMRI has a sensitivity of 88% and specificity of 72% revealing cardiac abnormalities in 62% of Churg-Strauss patients compared to 50% by echocardiograms. 6 Gadolinium-based contrast agents, which have the property of redistributing to areas of expanded extracellular space, can be used to detect acute inflammation and fibrosis. 7 This property, known as myocardial delayed enhancement, has been well correlated with pathologic specimens from endomyocardial biopsy. 7 T2-weighted fast spin echo imaging also allows for the detection of myocardial edema from acute inflammation. Our patient demonstrated myocardial edema of the left ventricle on T2-weighted images, as well as myocardial fibrosis of the left and right ventricles on delayed enhancement imaging (Figure 1). On repeat imaging, he demonstrated findings representing fibrosis secondary to prior inflammation (Figure 1).
While patients with myocardial involvement from Churg-Strauss present with a wide spectrum of cardiac findings, our patient presented with acute myocarditis. By using cMRI, we diagnosed the initial cardiac manifestations and followed the disease course. Cardiac MRI provides a safe and powerful tool for evaluating the presentation, progression and response to treatment of cardiac involvement in Churg-Strauss.