
Abstract
Lesson
White blood cells, Erythrocyte sedimentation rate and C-reactive protein are sensitive tools to discover rare, but potentially serious pyogenic vertebral osteomyelitis, a disease whose incidence is increasing.
Keywords
The incidence of pyogenic vertebral osteomyelitis (VO) is increasing and patients may present to their general practitioner with low back pain (LBP), seek orthopedic or even neurologic consultation, or present to the emergency department. Many physicians are not fully aware of the potential of VO to present insidiously, very often without fever. Thus, significant diagnostic delays remain common in all patient series. Our report highlights the importance of looking for ‘red flags' in patients presenting with LBP by describing a patient who also had an unusual microorganism and notable rare complications.
Case report
A healthy 55-year-old physical labourer presented with increasing low-back pain (LBP) over two weeks starting after heavy lifting and associated with growing lassitude, anorexia, weight loss and night sweats without fever. His general practitioner recommended bed rest. On admission, he looked acutely ill, temperature 36.5℃, pulse 98/min, blood pressure 90/55 and no other abnormal findings. Chest X-ray, electrocardiography and urinalysis were normal. Laboratory tests showed: haemoglobin 10.5 g/dL (normocytic), white blood cells 26.4 × 103/µL (90% neutrophils), platelets 92 × 109/L, international normalized ratio 1.12, activated partial thromboplastin time 26 s, D-dimer 2.05 µg/mL, erythrocyte sedimentation rate (ESR) 100 mm/h, C-reactive protein (CRP) 191 mg/L, blood urea nitrogen 50 mg/dL, creatinine 1.14 mg/dL, albumin 2.2 g/dL, globulins 4.1 g/dL (polyclonal), prealbumin 6 mg/dL and normal glucose, electrolytes, creatine phosphokinase and amylase. Bilirubin was 2.2 mg/dL (direct 1.3), alkaline phosphatase 307 U/L, gamma glutamyltransferase 182 U/L and aminotransferases 57–81 U/L. Diagnosed as severe sepsis with hypotension, acute kidney injury and disseminated intravascular coagulation, cultures were obtained and fluids and empiric antibiotic treatment were started. Urgent contrast whole body computed tomography (CT) revealed L1 osteomyelitis with bilateral psoas muscle involvement and filling defects in the adjacent inferior vena cava (IVC) representing thrombi (Figure 1(a) and (b)). CT-guided psoas muscle aspiration yielded purulent fluid with penicillin-sensitive Streptococcus intermedius, also found in 2/4 blood cultures. Echocardiography and colonoscopy were normal, ruling out infective endocarditis and colonic neoplasm. No hypercoagulability was found. The patient initially improved on ampicillin and low-molecular-weight heparin but later developed paraparesis and bladder distention. Magnetic resonance imaging (MRI) showed discitis, destructive D12-L1 osteomyelitis and an epidural abscess (Figure 1(c)). Emergent surgical decompression, bilateral laminectomies and discectomy were done with psoas abscesses drainage. Following extended rehabilitation, the patient is almost fully recovered.
Contrast-enhanced abdominal CT in coronal and sagittal planes on the patient’s admission (a and b) and contrast-enhanced sagittal view MRI two weeks later (c). CT showing destruction of anterior aspect of L1 vertebral body (dashed black arrow), adjacent IVC thrombi (white arrows) and psoas muscle abscesses (black arrows). MRI (T1 weighted TSE with fat suppression) showing enhancement of T12-L2 vertebral bodies (dashed black arrows) and epidural abscess (dashed white arrows).
Discussion
Differential diagnosis of systemic causes of LBP.

‘Red flags’ in patients presenting with LBP.*
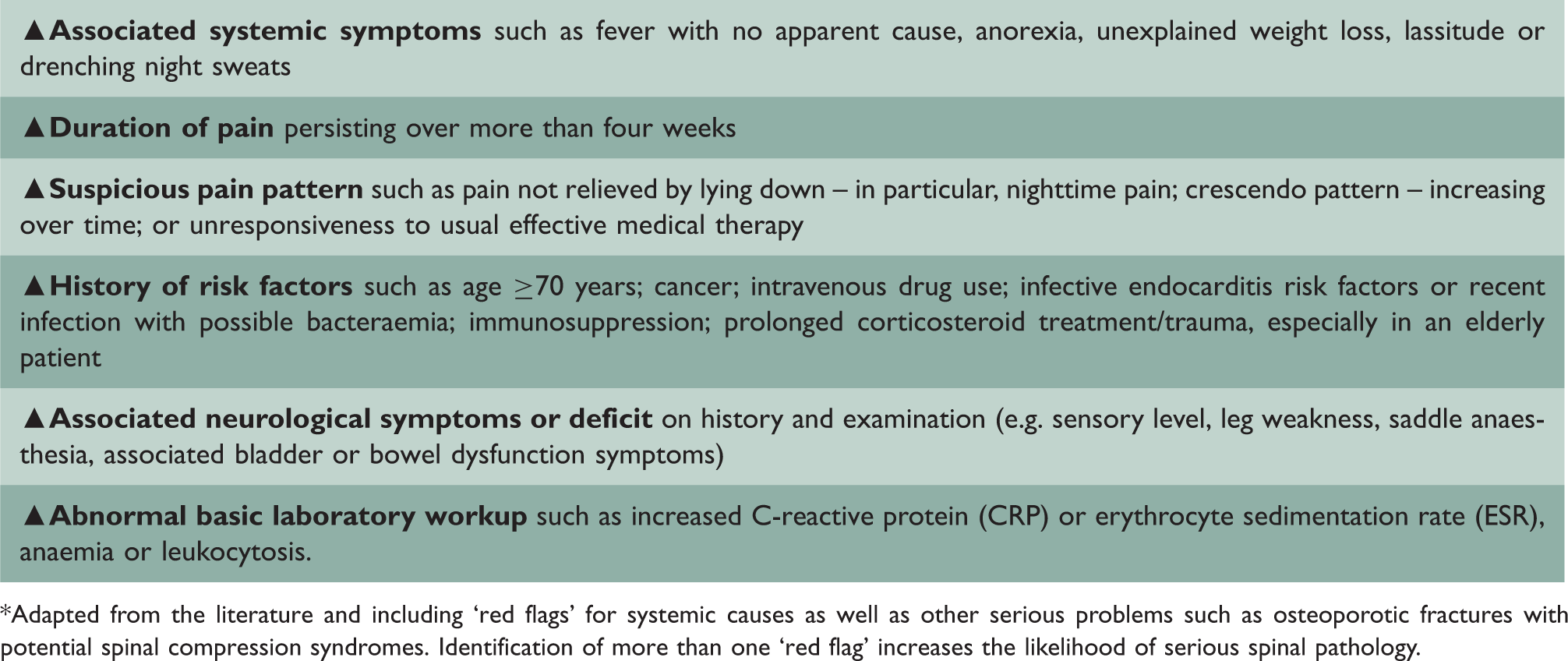
*Adapted from the literature and including ‘red flags’ for systemic causes as well as other serious problems such as osteoporotic fractures with potential spinal compression syndromes. Identification of more than one ‘red flag’ increases the likelihood of serious spinal pathology.
The common occurrence of LBP and persistent LBP in the population; the rarity of septic discitis accounting for less than 0.01% of cases in the primary care setting1,2 and the non-specific nature of many of the findings in the early stages, all contribute to a delay in diagnosis.1–3 Because such delay is common, a significant proportion of patients may present with neurological deficits on admission or signs of life-threatening severe sepsis. MRI is the imaging of choice, more sensitive and more informative than CT, 2 or roentgenograms that may not be revealing in one of two patients. 4 Importantly, fever is an inconsistent, frequently absent sign and its absence in a patient with significant persistent LBP does rule out VO. In contrast, acute-phase proteins are increased in most patients and helpful in early recognition by indicating the need of referral for appropriate imaging studies.1–3
VO is mostly acquired by haematogenous spread, but the portal of entry often cannot be identified. The dominant pathogen is Staphylococcus aureus, and many patients have underlying diabetes, immunosuppression or malignancy.1,2
Our patient’s age, sex and lumbar involvement are typical for VO, but the absence of a predisposing condition, the pathogen and the associated complications are rare.1–4 His VO likely followed a minor trauma disrupting the bone architecture as indicated by the history as well as S. intermedius bacteraemia, which is unrelated to infective endocarditis in most cases.5,6 S. intermedius belong to the ‘S. milleri’ group (SMG) organisms together with S. anginosus (the most frequent isolate) and S. constellatus. 7 They are most commonly found in the oral cavity (especially in dental plaque) where they constitute normal flora and also in the gastrointestinal tract and vagina. Most infections originate from the oral cavity or gastrointestinal tract, as is likely in our patient. 7 Though carriage of SMG organisms is regular, bacteraemia is infrequent. 5 Once it occurs, however, S. intermedius have a tendency to form abscesses and invasive pyogenic infections, unlike the other viridans streptococci. 8 However, SMG VO has been reported in only 10 patients, and secondary bilateral psoas muscle abscesses (by contiguous extension) are also unusual. Moreover, our patient had IVC septic thrombi proximal to the VO and the psoas abscesses – a very rare complication. Much like Lemierre’s syndrome (suppurative thrombophlebitis of the internal jugular vein in patients with severe oropharyngeal infections), proximal thrombi had been reported in rare patients with liver abscess, acute pyelonephritis or postpartum. 9 This is a first description of venous thromboembolism proximal to VO. Early recognition and treatment are imperative, combining prolonged parenteral antibiotics, anticoagulation and when necessary, surgical drainage.
Our patient exemplifies the spectrum of pyogenic VO and its important complications. The incidence of VO seems to be increasing, 10 and physicians’ awareness of this condition and its potentially misleading presentations should increase. In equivocal cases, verification of a normal blood count and, more importantly, ESR or CRP should be added to the ‘red flags’ screening and obtained early.