
Abstract
Large-scale data systems are increasingly envisioned as tools for justice, with big data analytics offering a key opportunity to advance health equity. Health systems face growing public pressure to collect data on patient “social factors,” and advocates and public officials seek to leverage such data sources as a means of system transformation. Despite the promise of this “data-driven” strategy, there is little empirical work that examines big data in action directly within the sites of care expected to transform. In this article, I present a case study on one such initiative, focusing on a large public safety-net health system’s initiation of sexual orientation and gender identity (SOGI) data collection within the clinical setting. Drawing from ethnographic fieldwork and in-depth interviews with providers, staff, and administrators, I highlight three main challenges that elude big data’s grasp on inequality: (1) provider and staff’s limited understanding of the social significance of data collection; (2) patient perception of the cultural insensitivity of data items; and (3) clinic need to balance data requests with competing priorities within a constrained time window. These issues reflect structural challenges within safety-net care that big data alone are unable to address in advancing social justice. I discuss these findings by considering the present data-driven strategy alongside two complementary courses of action: diversifying the health professions workforce and clinical education reform. To truly advance justice, we need more than “just data”: we need to confront the fundamental conditions of social inequality.
Keywords
Introduction
The past two decades have witnessed unprecedented attention to health inequality, including inequities patterned by gender, race, class, and sexuality (Braveman, 2014). Mounting public pressure to eliminate differences in health care access, treatment, and outcomes has fueled an emerging arena of “disparity policy,” with health equity instituted as a central concern within United States health policy making (Centers for Disease Control and Prevention, 2013; Department of Health and Human Services, 2011). At the same time, rapid technological advancements have garnered tremendous support within health reform, with technology viewed as a catalyst for change in transforming health care delivery. The surge of big data analytics in clinical settings, drawing from electronic health records (EHRs) and associated data-driven technologies, seemingly presents an opportunity to understand and intervene upon longstanding challenges in health care, including the problem of inequity. Taken together, this renewed public attention to “health disparities” combined with support for IT-based transformation have generated an emerging strategy of “data-driven equity,” in which data serves as the primary means of advancing social change in redressing inequality.
As a part of this “data-driven” strategy, health systems find themselves under increasing pressure to collect data on patient social differences (such as sexual orientation and gender identity (SOGI), and race, ethnicity, and language) and “social determinants of health” (including housing status, food insecurity, and social support) within EHR data systems (Cahill and Makadon, 2013; Douglas et al., 2015; Zhang et al., 2017). Data on social factors is central to equity, the argument goes, because data informs action and in turn leads to change. Data quantifies population-based differentials, tracks progress toward their reduction, and provides a sound research base for policy making and advocacy (Penman-Aguilar et al., 2016; Wasserman et al., 2019). Data is further integral to program administration and public accountability, with the goal of disparity reduction incorporated into data-based reimbursement schemes and public scorecards of system performance (Anderson et al., 2018; DeMeester et al., 2017). In our current era of big data analytics, data may also pinpoint equity gaps across geography and sites of care and allow health systems to develop population-based forms of treatment (Onukwugha et al., 2017; Zhang et al., 2017). Each of these proposed activities demonstrates the powerful allure of data-based strategies, with arguments for increased data collection fueled by high hopes of what technology will accomplish in the name of social justice.
Despite the enormous expectations placed onto data as a strategy for equity, however, there is little work that examines this data collection directly at the point of care, including frontline workers’ reactions to this flood of data-based initiatives. A review of academic scholarship identifies scientific reports based on resulting population-based data (Anderson et al., 2018; Penman-Aguilar et al., 2016; Zhang et al., 2017), and several agencies have issued technical guidance on data collection while publicizing data efforts as national work on “disparity reduction” (Centers for Medicare and Medicaid Services (CMS), 2015; Department of Health and Human Services, 2011; Fenway Institute, 2015a). However, few studies examine big data in action, choosing instead to focus on how to collect or what might be done after the data is already in. This sidesteps a crucial moment in which data intersects with the social world, as data and technology confront the social context they are expected to transform. By treating data as process (i.e., as a set of ongoing negotiations instead of an isolated technical artifact), this article offers an empirical examination of this strategy of “data-driven equity,” focusing on an extended case study of SOGI data within the field.
Drawing from ten months of ethnographic fieldwork at a large public safety-net health system, supplemented with 32 interviews with providers, staff, and administrators, I identify several emergent issues surrounding the SOGI data collection in relation to organization’s broader clinical setting. These issues speak to the central importance of social context in understanding the contours of health inequity, with the institutional conditions of safety-net care revealing the implicit assumptions within data-based strategy. In this article, I highlight three central challenges that elude data’s grasp on the problem of inequality: (1) provider and staff’s limited understanding of the social significance of data collection; (2) patient perception of the cultural insensitivity of data items; and (3) clinic need to balance data requests with competing priorities within a constrained time window. The issues identified in this case study reflect underlying structural challenges within safety-net care that remain unlikely to be redressed through data collection alone. While data and technology may hold great potential in advancing social change, this is neither automatic nor guaranteed (Bowker and Star, 1999). I discuss these findings by considering the data-driven imperative alongside two complementary courses of action: diversifying the health professions workforce and clinical education reform. These complementing strategies are more difficult to “see” amidst the data deluge, but together offer greater promise in redressing inequality beyond the present focus on technology-centered change.
Background
The United States health landscape has been subjected to a growing number of IT and data-based policy reforms, including new data analytic initiatives aimed at advancing health equity. This “data-driven” agenda is informed by several key developments. First, growing recognition of differences in health care access, treatment, and outcomes has drawn renewed attention to health inequity, with public officials instituting the goal of “disparity reduction” within multi-agency health policy making (Braveman, 2014; CMS, 2015; Department of Health and Human Services, 2011). Second, health systems have received expanded public scrutiny in relation to this policy objective, informed by scholarly work on clinical treatment’s contributing role in shaping inequality (Dubbin et al., 2013; Institute of Medicine, 2003; Spencer and Grace, 2016). Third, longstanding public critiques of medicine have fueled technological adoption within clinical care, with EHRs and data-based programs receiving strong bipartisan support within health reform (Ferris, 2010). At the intersection of these developments, advocates and public officials have called for routine, systemwide data collection on patient-level “social factors,” arguing that big data will transform health systems as a means of advancing health equity (Cahill and Makadon, 2013; Douglas et al., 2015; Fenway Institute, 2015a; Zhang et al., 2017).
In one sense, data as politics is nothing new. Data collection has long been central to policy making and public governance, with numbers at the heart of modern administrative states (Desrosières, 1998; Porter, 1995). The state primarily knows and acts upon the social world through quantification, with “the politics of counting” a problem of social knowledge and the making of mass publics (Merry, 2016; Scott, 1998). But in another sense, the political nature of data collection has transformed in our era of big data analytics, with new information gathering building from recently expanded technical infrastructure (Bigo et al., 2019; boyd and Crawford, 2012; Sharon and Lucivero, 2019). The national uptake of health IT reflects this emerging style of data-driven governance, with EHR databases simultaneously meeting heightened demands for public data while fueling expectations of local system transformation. The CMS has thus pursued new forms of accountability (Anderson et al., 2018; DeMeester et al., 2017) through public scorecards of system performance, data-based reimbursement schemes, and online presentation of downloadable data sets (data.cms.gov), all in the hopes of inducing “data-driven” change within sites of care.
Expanding from these policy initiatives, advocates and public officials have since latched onto data collection as the primary strategy for advancing health equity. This is particularly the case within gender and sexual minority health, with EHR data on patient SOGI viewed as “the key to ending LGBT health disparities” (Cahill and Makadon, 2013; Fenway Institute, 2015a). Public agencies have focused their efforts on specifying the technical requirements of this data collection accordingly (Figure 1). For example, in 2015, the Office of the National Coordinator for Health Information Technology mandated EHR vendors to provide technical capacity to record, modify, and access SOGI data (Meaningful Use Stage 3), suggesting this will provide more information to a patient’s care team to “aid in identifying interventions and treatments most helpful to the particular patient” (Fenway Institute, 2015b). CMS also prioritizes health IT in its CMS Equity Plan, recognizing standardized data collection on SOGI as an essential first step for “disparity reduction.” Building on these developments, the Health Resources Services Administration added SOGI data collection within Uniform Data System reporting requirements in 2016, with Federally Qualified Health Centers (FQHCs) expected to record and report SOGI items as a part of program participation. Advocates suggest this data collection within health IT programs is “one of the most important things our government has done to promote better understanding LGBT health disparities and interventions to reduce them” (Fenway Institute, 2015b), with data serving as the primary means of advancing social change in redressing inequality.
Recommended sexual orientation/gender identity (SOGI) questions.
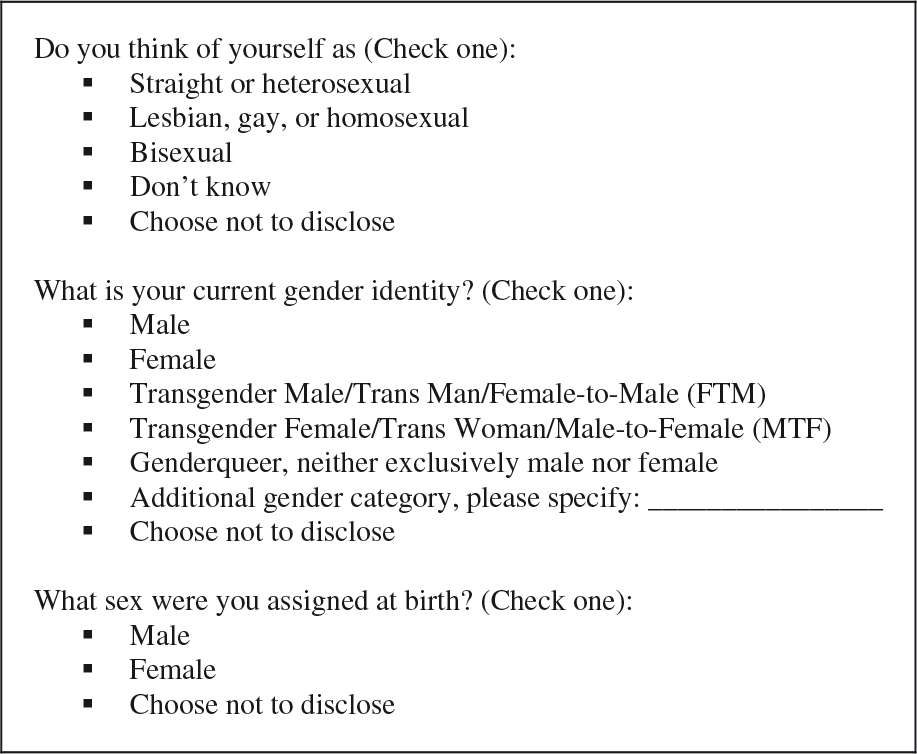
Source: reproduced with permission from Fenway Institute, 2018.
There is no shortage of arguments for expanded data collection on patient social differences, including SOGI and other “social factors.” From the perspective of state administration, aggregated population data may identify existing health disparities, benchmark progress toward their elimination, and inform social science research for data-based policy making (Penman-Aguilar et al., 2016; Wasserman et al., 2019; Zhang et al., 2017). Given that gender and sexual minorities have remained hidden for much of history, public data collection also carries symbolic significance within projects of state legitimation (e.g., “We don’t count if we’re not counted”). But the most promising attraction of this data collection is its potential intervention directly at the point of care, with big data analytics offering a key opportunity for system transformation (Douglas et al., 2015; Zhang et al., 2017). Researchers and advocates expect data to inform local providers and administrators on “who they serve” and “what patient needs are” in pushing toward equity (Cahill and Makadon, 2013; Cahill et al., 2014; Fenway Institute, 2018). Collecting SOGI data may lead to targeted screenings for “at-risk” populations and inform the future development of population-based treatments. Asking patients to “disclose” SOGI may also strengthen the patient–provider relationship, with data expected to enhance patient engagement and clinical communication. Identifying gender and sexual minority patients via data collection may further drive good “cultural competency,” such as permitting same-sex partners to enter hospital rooms or allowing patients to share preferred pronouns. SOGI data, in short, are widely expected to induce system transformation in alignment with health equity.
Despite these extensive arguments for data collection and the successive rollout of several SOGI data initiatives, however, there is relatively little work that examines big data in action within the health systems expected to transform. Existing studies focus on the technical details of item responses, reporting relatively high levels of patient acceptability in support of data collection (Cahill et al., 2014; Rullo et al., 2018). But as promising as they may appear, these studies typically employ survey methods that miss crucial elements affecting health care delivery in everyday practice. Focusing on the testing and development of standardized items, for example, tells us little about how these standards themselves interact with the social world, which is by no means guaranteed by their design or acceptability (Bowker and Star, 1999; Timmermans and Berg, 2003). But more importantly, such an approach downplays the social foundation of health care treatment and its relation to inequality itself (Spencer and Grace, 2016). The social practice of care is highly heterogeneous, shaped by institutional conditions, organizational settings, and interactional dynamics across patients and providers (Dubbin et al., 2013; Fiscella and Epstein, 2008; Rubin et al., 2018), yet these contextual factors have thus far received little attention relative to the technical details of item responses and the “acceptability” of proposed data collection.
Safety-net health systems reflect a particular setting of care that lends itself well to identifying the social context of health inequality. Typically defined by an institution’s relative placement within the ecology of regional health care delivery, the safety-net provides a significant level of care and services to uninsured, Medicaid, and other marginalized patients, and is strongly shaped by underlying political and economic arrangements that make it highly sensitive to policy change (Institute of Medicine, 2000). Public health systems and FQHCs serve as an essential core to the safety-net, historically providing indigent care to low-income populations. These organizations also typically serve higher proportions of racial and ethnic minority patients, monolingual non-English-speaking patients, and immigrant and undocumented patients, making the safety-net a key site for advancing health equity (Andrulis and Siddiqui, 2011; Fiscella and Epstein, 2008). In this article, I examine the initiation of SOGI data collection within a large public safety-net health system, using this case study to highlight the fundamental conditions of health inequality in relation to data-based strategy.
Theoretical framework
This article employs an ethnographic approach to examine data’s intersection with the social world, drawing on insights from science and technology studies (STS) and the sociology of quantification. Classic STS approaches call for studying “science in action,” leveraging a particular vantage point (“science in the making”) as means of opening up the black box of technoscience (Latour, 1987). Instead of treating data sets as technical artifacts only to be discussed after the data is “already in,” this article focuses on big data in action to develop a deeper understanding of the making and circulation of data throughout the social world (Law and Urry, 2004). In this case, data collection in the clinical setting involves a wide range of embedded actors who influence the character of “data-driven” transformation, with on the ground, technoscientific work shaping the nature of sociotechnical change (Bowker and Star, 1999; Clarke and Fujimura, 1992). Studying on the ground practices reveals the many elements in the situation, sharpening analytic focus from narrowly considered data sets to the data settings through which technical artifacts circulate (Loukissas, 2019).
These theoretical sensibilities further inform qualitative approaches to studying “big data,” with observational and interview methods capturing the contextual dynamics of emerging technologies (Merry, 2016). As large-scale data sources remake informational and organizational infrastructures from the inside-out (Clarke et al., 2003), ethnographic studies are particularly well-equipped to examine the complex, multi-faceted transformation engendered by computer and information technologies. A qualitative approach tracing the process of data collection itself, from initial activity with data scientists and analytics staff, internal meetings with system administrators and executives, and training visits with frontline providers and clinic managers, provides a multi-sited, multi-layered examination of the making and circulation of data within a single institution. Additional observations of care practices, including initial screening intake in the waiting room, the collection of vital signs by rooming staff, and documentation generated as a part of the clinical encounter, further capture the converging politico-economic, sociocultural, and technoscientific logics that undergird the work of becoming “data-driven.” I thus approach data collection as a social process, leveraging this case study from the safety-net to identify the emerging challenges surrounding technology-centered change.
Methods and fieldsite
This article draws from ten months of ethnographic fieldwork (n = 450 hours; September 2017 to June 2018) at a large public safety-net health system, supplemented by in-depth, semi-structured interviews (n = 32) with local providers, staff, and administrators. The health system primarily serves low-income patients on Medicaid and the remaining uninsured, with patients collectively reflecting a wide range of linguistic, cultural, and ethnic diversity. In initiating fieldwork, I first shadowed a primary data team charged with integrating data analytics within the health system under a data-based state accountability program. I attended internal meetings within administration, the department of quality, the analytics division, and several outpatient clinics and participated in the data team’s everyday work of program building, data analysis, and report writing. I then conducted targeted outreach at two outpatient clinics to observe the uptake of data and technology on the ground, shadowing frontline providers, clinic managers, and system staff as a part of routine proceedings. These observations were supplemented with in-depth, semi-structured interviews with key local actors representing a variety of roles. I interviewed program managers, data analysts, primary care providers, complex care nurses, quality improvement coordinators, clinic managers, and administrators, reflecting diverse backgrounds in medicine, nursing, public health, business administration, and computer science. Interviewees were asked for their perspectives on a wide range of topics, including state program implementation and data analytics integration. All fieldnotes and interview data were transcribed and analyzed following the principles of grounded theory (Charmaz, 2007).
The SOGI data collection initiative served as one main component of the larger data-based state accountability program, with the data team leading implementation within the system’s outpatient clinics. The team developed a brief training on SOGI (under an hour in length) and scheduled on-site clinic meetings with providers and staff to review prepared slides and handouts. Due to initial discomfort and disinterest in the topic (both from data team members as well as clinic providers and staff), perceived lack of support from clinic leadership, and operational staffing concerns during the scheduled training, not all providers participated in these sessions, opting instead to sort out the data collection themselves among their own support staff. Taken together, these initial observations suggested the deprioritization of the SOGI data initiative relative to other systemwide activities, ultimately motivating the present case study. In this article, I focus on the contextual elements that shaped this health system’s response to the data collection, presenting thematic findings on the present strategy of “data-driven equity.”
I: Provider and staff’s limited understanding of the social significance of data collection
Data is typically expected to stand on its own, with data collection positioned as a window of transparency yielding self-explanatory information. Expectations of SOGI data are not divorced from this thinking: advocates and public officials widely suggest that identifying patient populations within EHRs will lead to providers understanding patients and providing affirmative, population-tailored care (Cahill and Makadon, 2013; Fenway Institute, 2018). But while data collection may be quickly instituted due to its ability to atomize complex theoretical issues into a few standard checkboxes, there is no guarantee that those expected to work with data on the ground share the same understanding as those mandating collection at the level of policy. The practice of data collection alone does not tell providers and staff why and how sexual and gender difference matters for health, nor which particular aspects matter in which kinds of ways. Collecting patient-level data, furthermore, diverts attention away from more fundamental issues among health care workers, including their own views on whether sexual and gender difference is relevant for health, how they understand the nature of difference, and whether they are able and willing to advance equity through care.
At the health system I studied, SOGI data collection commanded a wide range of reactions at all levels, drawing provider and staff’s attention to the issue via the newly added agenda item. In sorting through the varied questioning following the initiative’s announcement, however, it was clear that few understood what they were expected to do now that the items were to be asked of patients. Providers and staff not only questioned the data collection itself, but also expressed skepticism as to whether sexual and gender difference mattered at all for patient health. One of the main staff members involved with the SOGI initiative identified this as the primary challenge surrounding data collection, with providers’ lack of understanding associated with a lack of buy-in: I’ve heard and been given feedback from providers, “I don’t understand why we’re doing some of these things” [data-based initiatives]. In particular with the SOGI questions, “I don’t understand why we are asking these questions. What does this have to do with somebody’s health?” I understand where they’re coming from, there’s a lot that’s already required of them, and now we’re asking them to change, to see providing health in a different way … It’s often hard for someone to even understand why we need to ask these questions, and then having to explain social determinants of health and health disparities to somebody who might not necessarily know what those things are. Even though they work in the health field, but my background is in public health, and there’s a lot of focus on social determinants, stigma, and all of those things. Primary care, from my observation, doesn’t seem like it so much, so it’s hard for them to even just understand health disparities … and if they’re not seeing the value of why we ask somebody that, it’s challenging to get their buy-in to ask these questions. It’s also challenging because these are things that we don’t talk about, like we don’t talk about sex or sexuality, so now we’re asking our providers to ask our patients this. Our providers are not comfortable talking about this with our patients, they aren’t even comfortable talking about race and racism. That’s something we know exists. But some people don’t even think it exists! Personally, I think we need to do more around social determinants of health and health disparities and really explaining that to people because– I don’t know that everybody’s universally onboard with why these questions have anything to do with your medical health. Program Analyst, Administration
In presenting data collection as something to simply implement in straightforward fashion, furthermore, technical standards fail to foster a deep comprehension of the complex nature of gender and sexuality. For example, scholars have long noted the multiple domains of sexual orientation, including identity, behavior, and attraction (Cruz, 2017). While recently initiated SOGI data collection primarily consists of identity items (Fenway Institute, 2015a; Figure 1), health systems may already gather information relevant for understanding patient differences (e.g., via sexual behavior). This unexamined connection across multiple domains surfaced during a post-interview EHR walkthrough with the team’s data analyst. He first clicked on the “Demographics” tab to show me where the SOGI data was recorded, collected along with patient sex, date of birth, and race and ethnicity. I noticed a “Social History” tab on the side of the screen, which he opened to reveal clinical documentation space for “risk behaviors” such as alcohol use, drug history, and sexual behavior—the latter containing checkboxes for activity with “men, women, or both.” Curious if sexual behavior ever came up during SOGI discussions, I asked the data analyst how he thought the two data points related to one another—couldn’t the existing behavioral data already identify certain sexual minority populations, complicating the SOGI identity items? He looked back at me, wide-eyed and stunned, before responding: “Wow- you know, I never thought about that! That really hasn’t come up at all, actually. I’ll have to mention it at our next meeting.” The practice of asking sexual activity has a long history within medicine, and yet based on my fieldwork, few staff or providers directly considered the connections between the two domains (additional connections were also left unexamined, such as the conflicting logics of gender identity items with sexual behavior responses based on sex). Each dimension of difference might matter for “equitable” care, yet if health care workers fail to appreciate the complex nature of gender and sexuality, then data collection on any item is unlikely to result in health equity.
Data does not stand in for the argument of the social basis of inequality, nor do they guarantee that such an argument is universally spread across society. Data collection on sexual and gender difference is relatively new compared to racial difference, yet it would be wise to learn from previous data-based efforts aimed at health equity. Ann Morning opens The Nature of Race noting that bureaucratic data collection within hospitals, schools, and government rarely come with an explanation of what race is and why it matters. In the absence of such explanation, institutionally embedded human actors are largely left to their own devices in making sense of the nature of difference (Morning, 2011). Dorothy Roberts (2012) further highlights how the broad acknowledgment of racial health inequities has by no means led to a straightforward interpretation of such disparity: countering emerging explanations based on race-neutral economics or inaccurate race-based genetics, she instead provides a powerful argument for the social nature of inequity based on stratified power and social hierarchy. Data cannot tell us what difference is, what it means, or how it matters for health, because data alone does not replace the argument for the social basis of health inequality. Without this shared understanding of data’s social significance, data collection is unlike to lead to any form of “data-driven equity.”
II: Patient perception of the cultural insensitivity of data items
The setting of technical specifications may grant new forms of legibility to the people being counted, with data collection sorting the social world into predetermined boxes in seeming isolation from other variables (Figure 1). And yet, the world we live in is highly heterogeneous, with people carrying a wide range of ideas and beliefs about themselves and others. Issues may then arise when forms of data collection do not correspond with the social worlds of those being measured (Merry, 2016; Scott, 1998). In the case of SOGI data, providers and staff perceive that not all patients see gender and sexuality as relevant for receiving care, suggesting these domains may be inappropriate in the clinical context due to patient differences in culture, language, and religiosity. Given the enormous structural challenges experienced in the safety-net, it would be short-sighted to dismiss this perceived insensitivity as part of national backlash against topics related to gender and sexuality: rather, social and cultural assumptions about who and what patients are like—such as being comfortable discussing sexual activity, possessing familiarity with American culture, and speaking English supported by a high school education—all play out at the point of data collection, with providers and staff concerned about potential impact on already marginalized patients.
Recommended sexual orientation/gender identity (SOGI) questions.
When discussing data collection at clinic meetings, providers and staff would share instances in which patients responded poorly to the SOGI items, shaping workers’ understanding of the issue (due to study design and institutional review board approval, I was unable to interview patients directly; but see Thompson, 2016 for research on this topic). In several cases, providers expressed concern with communicating issues of sexual and gender difference with patients who exhibit other forms of marginalization, such as non-English-speaking ability or lack of familiarity with American culture, or other characteristics such as high religiosity or low educational attainment. While from the perspective of technical data collection these aspects are all seemingly unrelated to gender and sexuality—after all, a patient could experience several of these and still be gender or sexual minority, of course—from the experience of frontline providers, these dimensions are often intertwined in ways that challenged such an understanding. The medical director of the system’s main outpatient clinic shared her discomfort around asking SOGI items, not because she believed they were entirely unimportant, but because she perceived the items to be culturally insensitive among certain marginalized patients:
What are your thoughts on the recent data collection on SOGI?
(pause) Personally, I’m a Christian. So I’m going to be honest with you. Yes, please. You should feel free to be honest with me. Yeah. I think asking SOGI data, the good thing about that is you don’t want to miss screening procedures for patients with gender transition, but at the same time, I don’t know if culturally … in my opinion we are discriminating more by asking these questions, I think.
What do you mean?
It means everybody is, according to me, already the same. So asking these data and putting them in a separate category, I mean we can look for screenings, but … okay, for example. Elderly couples come here, and if we are not culturally sensitive, we go and ask those questions and you will actually – patients get really offended, angry. So I don’t know. I’m not against it, but I’m not a big cheerleader because of my own religious reasons. I’m okay to ask those questions and document. But I already take care of them [gender and sexual minority patients] without judgment. And asking these questions, it’s like we have to be very careful about who we ask.
Have there been any challenges?
Yeah, a husband and wife came to the clinic for example, an Iranian couple, and I asked the wife – the wife usually comes in with the husband, right? – and I asked her, “Biologically, do you think at birth you were a female or male? Then what about now? Are you still a male or female? And do you like to have sex with men?” (shakes head) You know Iranian culture, even Pakistan and some Muslims from India, they can be very conservative. So when you ask that question in front of the husband, you know they both just completely shut down, especially at the beginning of the visit. So for me then it’s kind of difficult – you go in and they’re still upset with those questions. “Why are you asking me this, are they going to ask this question every single visit? Doctor, if they don’t have such questions in the future, I will really appreciate it.” I think it’s a taboo for them, talking about sex. I think it’s the culture, completely cultural. Medical Director and Primary Care Provider, Outpatient Clinic
I gathered additional insight into this issue at a statewide meeting for all program-participating health systems, with representatives from different organizations sharing their experiences with the SOGI initiative. One program manager, representing a rural health system, expressed extreme frustration with the data collection in relation to the unstated assumptions about the patients to be asked the SOGI items. She shared her health system’s experience asking the questions to non-English-speaking Latino/a migrant farmworker patients, in which initial efforts at cultural and linguistic translation had proven challenging. As a result, neither providers nor staff were willing to ask the items any further: How do you translate this to them [migrant farmworkers] in a way that’s not offensive? There is no respectful translation for them! Just asking the questions, we’ve lost patients from the fields, and they’re not coming back. They just up and leave, so our staff have refused to keep asking the questions. We’re not going to ask anymore, even if it means us losing money. [data collection tied to financial reimbursement under the state program] (Fieldnotes)
Theorists of intersectionality would remind us that gender and sexuality never stand alone as single constructs that directly correspond with social experience, but that these are always informed by other human dimensions such as race, class, and citizenship (Collins, 1990; Crenshaw, 1989). Intersectionality’s focus on centering multiple dimensions across levels of analysis (Choo and Ferree, 2010; McCall, 2005) is applicable here to the case of SOGI data. In a safety-net institution, with patients speaking a high number of non-English languages and representing a wide range of backgrounds, differences manifest in understanding and experiencing difference (Cruz, 2017; Thompson, 2016). Despite the tremendous work done to develop technical standards to measure patient differences through SOGI items, which seemingly identify the desired populations among all, this work does not eliminate social understandings of difference: it merely reflects one particular form of understanding that is expected to represent all people. Providers, staff, and patients are largely left to make sense of these terms through their respective prisms of race, class, culture, religion, and language, translating around the technical standards of data collection. These challenges risk providers and staff questioning the data’s appropriateness for already marginalized populations, with human actors unprepared to do the behind-the-scenes cultural work required for “data-driven equity.”
III: Clinic need to balance data requests with competing priorities within a constrained time window
Data collection does not take place in a vacuum. SOGI data is merely one of many items collected, including routine vital signs, health behavior assessments, substance use screenings, physical abuse questionnaires, and patient satisfaction surveys. In isolation, each of these data points are arguably introduced for optimizing patient health; taken together, however, they crowd each other out given the particular context in which safety-net care takes place (Fiscella and Epstein, 2008). Fifteen-minute visits, coupled with patient transportation or literacy challenges and provider documentation demands, severely limit SOGI’s potential impact within the clinical setting. Data collection is merely one activity of providing care: consulting with the patient, reviewing lab results, documenting EHR notes, refilling prescription orders, and addressing last-minute requests all reflect a context in which more and more is asked to be done within a constrained time window. Data collection on SOGI neither stands outside of nor fundamentally undoes this dynamic: rather, it becomes “just one more thing” as part of the flood of expectations placed onto the safety-net.
While not all forms of data are patient-reported, a significant portion of information gathering does require some level of patient participation. Multiple questionnaires, for example, are filled out by patients in clinic waiting rooms prior to the start of the appointment visit. In our biomedicalized culture of viewing patients as always already “at risk” or potential patients-in-waiting (Clarke et al., 2003; Timmermans and Buchbinder, 2010), patients and staff find themselves with a heightened burden of administrative work to complete for care. As the nurse manager below notes, these “tests” potentially overwhelm the human actors in the safety-net, with limited time to implement data collection: For [patients] to have to take a test – I call it a test, right? Because it’s a questionnaire, you answer. Some of those assessments terrify me because it can easily be a 50-item questionnaire. And then now you’re asking SOGI questions. So that’s really a lot that patients have to take on coming to this clinic, right? There’s SOGI, your PHQ-9 [depression screening], health assessments … As a patient myself, I would be totally overwhelmed. So that is the big question mark – as administrators of this clinic, how do you avoid that patient being overwhelmed, staff being overwhelmed, because on top of everything that we’re asking them to do, they can’t really say, “Oh, I don’t want to do it.” But it’s a lot that’s going on right now and as administrators we really need to make sure they’re all aligned to benefit our patients … You can imagine. Rolling out our photo initiative. Blood pressure rechecks. The SOGI questions! So maybe now you can understand what I was saying earlier – it really takes a lot of time for us to implement something, but we have to make a change without really looking at the details. Nurse Manager, Outpatient Clinic
Patients and staff are not the only ones pressed to give more and more attention to generate data: primary care providers also feel competing demands for time within the compressed 15-minute appointment window. From the one-time asking of SOGI items, advocates and public officials expect providers to provide competent, equitable care based on resulting data. But this is unlikely to happen if providers are not equipped to understand what such care would look like (discussed above) nor if they do not have the space and resources to do so. One physician champion, who overall expressed great enthusiasm for this turn toward data analytics, noted the strong impact her working conditions has on her ability to engage with SOGI data:
How do you think providers would react to having the SOGI data in the EHR?
I think they are too busy to pay attention, honestly. (pause) I mean, it might make a difference in terms of screening people for sexually transmitted diseases or that kind of thing, but to be honest I’m not sure it makes such a big difference with everything else we have going on here.
(extended pause) It sounds like what you were saying earlier, about there being too much—
Exactly, there’s just too much, and you’ve got fifteen minutes and the patient has ten things they want to talk about and you have two things you want to talk about and they need med refills, you know what I mean? And they’ve got to do all the screening stuff and immunizations, and we have to document, and and and. You can imagine, fifteen minutes is not a lot of time. You have to be totally “on” to fit it all in, and so all this other little stuff just falls by the wayside … Data’s great, but you have to have the time and energy to be able to look at the data and understand what that means, and for us right now it’s all about visits. My docs were seeing patients nine half-days a week. That four extra hours is filled with disability forms, refills – you know, you’re working all the time and you don’t have a block where you can just sit down and go, “Oh look, let’s pull the data from this population or that population.” I mean 11 patients per half-day is a lot of patients, and the more patients you see, the more lab results you have, the more refills you have, the more work to be done in the in-basket, messages that are coming in you have to work through, and there’s really just no time. Data’s great, but you have to have the time and energy to deal with it and to understand what it means and to make changes based on that and for a working doc here, we just don’t have time. Primary Care Provider, Outpatient Clinic
The organizational context of public safety-net care poses a serious challenge to the kind of data-based change sought by advocates: if there is no ability to meaningfully engage with resulting information, then what is the real value of collecting data? SOGI data may certainly be used at the local level by data analysts or administrators, or at the aggregate level by public officials or researchers. But even when quantifiable disparities are identified post-data collection, how are they to be acted upon in a context in which patients, providers, and staff alike are already pressed for time and resources, compounded by the socioeconomic challenges that profoundly pervade the safety-net? In certain contexts, it may be possible that data is easy to collect, analyze, and act upon to provide population-based care, with providers given the adequate space to do so. In the safety-net, however, this may be unrealistic without the broad recognition that implementing these changes requires additional resources beyond existing infrastructure. Data advocates may continue to argue for “data-driven equity,” but without a full understanding of differences in organizational context, they risk increasing burden without yielding transformation.
Discussion
Data-based policy initiatives carry strong currency in our current era of big data analytics and technology-driven change, with EHRs seemingly offering a key opportunity to advance health equity. But despite the potential promise of data-centered strategies as a part of United States health systems’ turn toward becoming “data-driven,” standardized data on patients tells us relatively little about the institutional conditions that undergird the problems we seek to redress. The ethnographic case study on big data in action I present here, in contrast, identifies key themes that inform our understanding of health and health care inequalities. Data alone will not equip providers and staff to understand health as a social phenomenon, rooted in structural inequities and intersectional complexities. Nor will it undo the organizational context of the public safety-net, in which multiple forms of patient vulnerability and administrative bureaucracy shape how patients and providers participate in care. Despite the grand expectations placed onto data as a means of social change, this case study from the safety-net suggests the pursuit of justice will require more than mere technical strategy. Advancing health equity will require a deep comprehension of the fundamental conditions that drive health inequalities and a firm commitment toward their elimination.
In the remainder of this article, I position the technical strategy of data collection alongside two complementary courses of action in alignment with health equity: diversifying the health professions workforce and reforming clinical education. None of these proposals should be seen as fixed solutions for the problem of inequity. However, these latter two courses of action shift the focus away from individual encounters (as with patient-level data collection) toward institutional conditions (including the composition of the health professions workforce, programs and policies of system administration, and scope of clinical and staff education). These latter approaches thus demand time and resources in pursuing the long road to health equity, comprising a qualitatively different strategy from the quick rollout of national data collection under IT policy and associated reporting requirements. But taken together, all potentially offer greater promise in bringing sustainable social change to the institution and practice of medicine.
Diversifying the health professions workforce as a means of advancing equity is not a new argument, even if it has yet to fully appear in the health policy realm with regard to SOGI (Council on Graduate Medical Education, 2016). A similar strategy has long been proposed in addressing racial and ethnic minority health inequities (Phillips and Malone, 2014; Sullivan and Suez Mittman, 2010), and more recent work connects the lack of a diverse tech workforce to the emerging challenge of algorithmic bias (AI Now Institute, 2019; Noble, 2018). Building on existing attention to diversity within the health professions (Council on Graduate Medical Education, 2016), advocates and public officials may expand these efforts to consider issues of gender and sexuality, placing special emphasis on gender and sexual minority professionals who also possess experience with nondominant racial, ethnic, linguistic, or cultural difference. Providers with direct experience of being gender and sexual minority may be better equipped to relate to and serve similarly situated patients, conduct gender and sexual minority health research, and mentor other providers and academics in the field (Mansh et al., 2015; Sánchez et al., 2015). Furthermore, just as the medical director from the case study centered her own experience in making sense of differences among patients, increasing the number of open gender and sexual minorities in the workforce will require all providers and staff consider differences among themselves as a means of understanding differences among patients. Pursuing this strategy poses its own set of challenges, as issues of stigma undoubtedly play out within medical education, hiring practices, and career promotion (Mansh et al., 2015), and there is no guarantee that members of underrepresented groups are fully incorporated within organizational proceedings (Berrey, 2015; Ely and Thomas, 2001). But if these fundamental issues exist at the institutional level, then individual interventions based on data sets are unlikely to bring about significant change in precisely such a setting (Loukissas, 2019). The findings I present here also caution against treating gender and sexuality as divorced from class, culture, language, race, and ethnicity, and these diversity efforts should thus pursue multiple forms at once so that providers and staff may be better equipped to translate across difference in providing equitable care.
Clinical education reform aimed at the future generations of the health professions workforce may also strengthen the pursuit of health equity, with all providers, staff, and administrators trained to understand health as a fundamentally social phenomenon. Introducing “structural competency” (Donald et al., 2017; Metzl and Hansen, 2014; Willging et al., 2019) as part of the education provided to registered nurses, physicians, physician assistants, social workers, and other allied health professionals offers an opportunity to foster a deeper understanding of the social significance of gender and sexuality in relation to health equity. Currently, most modules on SOGI are brief and/or elective (Carabez et al., 2015; Obedin-Maliver et al., 2011), with uneven incorporation into licensing exams conveying the systemic deprioritization of these topics within clinical training. Expanding from these efforts, education-based reforms should encourage clinicians to be aware of and actively work to change the social determinants of health and social context of health care, moving from individual-level interventions to address norms, institutions, and resource distribution shaping structural inequities in health (Link and Phelan, 2010). Training-centered approaches carry risks as well, as evidenced by the past decade of “cultural competency” initiatives (Betancourt et al., 2003) focused on patient values and beliefs at the expense of system-level concerns and power relations. But integrating teaching on structural factors, including the social and political shaping of care, stigma and social determinants of health, and power and stratified hierarchy across difference, holds enormous promise in shifting how clinicians understand their role in advancing health equity. This in turn may encourage providers and staff to advocate for funding and resources on behalf of marginalized communities, extending social change within existing health systems and beyond.
A multi-faceted strategy is surely required to achieve health equity, and these three approaches—collecting patient-level data, diversifying the health professions workforce, and reforming clinical education—may be seen as complementary and mutually reinforcing. And yet, technological advancements far outpace the systemic reforms proposed above, with data collection left alone as the primary strategy for redressing health inequities (Cahill and Makadon, 2013; Fenway Institute, 2015b). As the findings of my case study show, however, leading with data collection may not necessarily result in significant institutional change across all settings. If providers, staff, and administrators do not understand the social significance of data, remain unprepared to translate technical items across heterogeneous populations, and possess limited time to engage with resulting data, then data is unlikely to drive desired transformation—despite the grand hopes and expectations that fuel this strategy of “data-driven equity.” This article furthers the sociological call to contextualize health inequalities (Dubbin et al., 2013; Link and Phelan, 2010; Spencer and Grace, 2016), showing how the social context of safety-net care shapes the invisible work needed to advance social change. Future scholarship might examine this work across institutional settings, with comparative studies illuminating the contingent factors and hidden assumptions that undergird the strategy of “data-driven equity.” Future work should also examine health system responses to other data collection on “social factors,” including data on race, ethnicity, and language and “social determinants” such as housing status, food insecurity, and social support, and how such data initiatives reconfigure relations of inequality.
Conclusion
The rapid pace of IT development has ushered in grand hopes and expectations of “data-driven equity,” with technology-driven agendas shaping public strategies for social justice. Yet despite the eager clamor to leverage big data in the name of social change, data alone cannot fully address the underlying conditions informing the problem of inequality. The major challenges that undergird inequality, after all, are not merely technical issues, but profoundly social ones. Inequality is first and foremost a deeply social problem rooted in the hidden institutional conditions that shape all of social life. To redress inequality, we need more than “just data”: we need to confront the fundamental issue of where and how certain people stand relative to others. Perhaps then we will finally advance “the highest possible standard of health for all people” (Braveman, 2014), based on social conditions. Perhaps then we will finally exchange quick technological fixes for genuine social change.
Supplemental Material
sj-pdf-1-bds-10.1177_2053951720928097 - Supplemental material for Perils of data-driven equity: Safety-net care and big data’s elusive grasp on health inequality
Supplemental material, sj-pdf-1-bds-10.1177_2053951720928097 for Perils of data-driven equity: Safety-net care and big data’s elusive grasp on health inequality by Taylor M Cruz in Big Data & Society
Footnotes
Acknowledgments
I am grateful to the Health Tech Justice Research Group for providing general research support and to Ariana Thompson-Lastad, Hale Thompson, Jamie Budnick, and Mariana Lopez for sharing insightful feedback on an earlier manuscript draft. I would also like to express special thanks to my mentor, Janet Shim. Thank you, Janet, for making me the sociologist I am today.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by UCSF Departments of Social and Behavioral Sciences and Anthropology, History, and Social Medicine.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.