
Abstract
Introduction
To assess how health care professionals outline the management of care and explore which health or social care professionals were involved in the patient's treatment.
Methods
A survey with a patient vignette for general practitioners (n = 31) and registered nurses (n = 31) working daily in Finnish health centres located in four cities. Respondents answered structural questions and explained in detail the care process that they tailored for the patient. The care process was examined using content analysis.
Results
A physician–nurse working pair was declared to be in charge of the care process by 27% of respondents, a registered nurse by 9% and a general practitioner by 11%. However, 53% reported that no single person or working pair was in charge of the care process (response rate 72%). The concluding result of the analyses of the presented process was that both treatment practices and the professionals participating in the patient's treatment varied. Collaboration with social services was occasional, and few care processes included referrals to social services.
Conclusion
For the patient who needs both health and social care services, the management of care is a challenge. To improve the chances of patients being actively involved in making treatment plans at least three factors need to be addressed. Firstly, a written treatment plan should explicate the care process. Second, collaboration and interaction between health and social care services should be strengthened, and third, a contact person should be named to avoid care gaps in primary health care. Next-step data from patients need to be collected to get their views on care management and compare these with those from general practitioners and registered nurses.
Keywords
Introduction
One of the key problems in primary health care (PHC) is how to best manage care for patients with multiple care needs in order to ensure access to the necessary services and continuity of care. PHC is used both by occasional users, whose care needs can be solved within a single visit or a few visits, and by patients with more complex and demanding care needs.1,2 A small portion of the population (10%) has been found to use many different services, accounting for the majority of the use of resources of health and social care in Finland. 3 This paper focuses on this group of service users using a fictitious patient belonging to this group.
In Finland, health care is mainly financed by taxation and the Finnish citizen has a right to use public health care services. In 2015, the gross domestic product of healthcare expenditure was 9.4 in Finland and the OECD average was 9.0. 4 Municipalities are responsible for providing health care services by either producing or purchasing the services. The use of private health care services has increased in recent years and some municipalities have outsourced entire health centres. PHC centres dispense both curative and preventive health care. Some municipalities use patient segmentation where some of the health centres focused on chronic conditions, and some provided preventive medicine and services for care needs that can be solved within one or two visits. 5
The Finnish health centres have different organisational features, but at minimum they are staffed with general practitioners (GPs), registered nurses (RNs) and administrative personnel. Some health centres have a wider array: a laboratory, specialist psychiatric nurses, psychologists, social workers, physiotherapist, consultative gerontologists or psychiatrics. 6 The modes of grouping in networks vary: health centres staffed with GPs, RNs and other health care professionals can arrange interprofessional teamwork, whereas health centres staffed simply with GPs and RNs may need to use networks and arrange these professional services from other municipal or private organisations. In contrast to many other European countries, the RNs have relatively large autonomy and carry out a wide range of tasks while working in Finnish health centres. 7
Recently, major efforts towards informational continuity have been made by launching a national digital repository for electronic patient data (Kanta). Patients can download summaries of their electronic health records and prescriptions from this online portal. The implementation and development of Kanta is still in progress, but it is mandatory for the health service providers to attend Kanta. In trying to improve informational continuity one central problem is that social services are often behind information barrier because they mainly use information collection systems which are incompatible with those used in PHC.
Suboptimal functions in PHC services have been recognised in several countries 8 and the problems have been identified at policy, organisational and health care professional levels (which are often discussed as macro, meso and micro levels) and each of the levels interacts with and influences the others. 9 Common difficulties in the meso and micro levels are a lack of GPs and problems with the continuity of care.10,11 In developing the functionalities of Finnish PHC, where doctors are mainly grouped in local public structures with multiprofessional teams, several activities at different levels have been implemented: firstly, the promotion of PHC at the national level; secondly, the development of disease-specific guidelines and the local treatment pathways for certain diseases (available for health care professionals through the web: Current Care Guidelines) at the national level; thirdly, the strengthening of chronic care through organisational arrangements, such as centralising chronic care to certain specialised health centres; and fourthly, widening the array of the professionals participating in patient care. The crucial problem in Finnish PHC has been poor access to health centres and there have been imbalances over time, regarding production capacity, and the need for care between areas which generates the long waiting times in some PHC centres. Formerly, patients only had access to the health centre located in her or his residential area, but as a solution to the local problems, a national level reform implemented patients' freedom to choose the health centre. Currently, patients can choose a PHC centre with shorter waiting times which fits with the aim of the reform to improve access to PHC.5,6,12,13
It is commonly known that patients with a chronic disease or multi-morbidity benefit from a care plan.14,15 It is essential to tailor treatment for patients with complex care needs in order to ensure the continuity of the treatment. From the patient's perspective, continuity of care has three important dimensions: informational continuity, relational continuity and management continuity. 16 Informational continuity basically means that information on prior events is used to provide care that is applicable to the patient's current circumstances. Relational continuity is used simultaneously with personal continuity and means that the patient is in an ongoing relationship with the same health care professionals over time. Management continuity ensures that planned care from different providers is connected in a reasonable manner. 16 Building inter-organisational communication has been found to be difficult.8,17,18 In Finland, electronic patient record systems are often criticised because several different systems are used that are not compatible and involve structural barriers in the flow of information between PHC, secondary health care or social care.3,19 All in all, patients appreciate it when the same professionals take care of their treatment, 14 and continuity of care is related to better health outcomes.20,21
Patients with chronic conditions have reported more negative experiences in primary care in comparison to patients without chronic conditions 22 and studies on care coordination among these patients suggest that implementing a personalised care plan leads to improvements in patients' capability to manage their condition. 14 One meta-analysis suggests that implementing interventions among frequent users of health care services should include specific strategies, like case management and the promotion of self-management, in order to reduce health care utilisation. 23 The definition of care coordination has been discussed widely 24 and in the definition adopted by McDonald and Schultz the resources needed to carry out the required patient care activities include personnel.
This paper presents a micro-level analysis of variation in the everyday practices for a care process in the vignette of a patient with multiple care needs in PHC. The first study objective is to explore who will have responsibility for the management of patient care in the health centre and furthermore to investigate what kind of care processes are outlined to the patient. With vignette methodology we uncover the practices concerning the horizontal integration that takes place between health services and social services, as well the vertical integration that takes place between PHC and hospital care services. Furthermore, we recognise the practices that allow the integration of care within PHC (e.g. practices with both a GP and mental health services) and practices that support shared decision making between care providers and the patient.
Methods
Study design
A vignette study of fictitious patient with multiple care needs.
Data collection
The theoretical framework has three pillars: practice variations in health service utilisation, the chronic care model, and integration of care in terms of both horizontal integration (between health services and social services) and the vertical integration (between PHC and hospital care services).9,12,13,25,26 Practice variation may be studied at different levels of health care (micro, meso, macro), from considering the individual GP or RN as a decision maker to the level of an entire health care system. To examine practice variations in micro level (e.g. from GP or RN point of view) a vignette survey conducted. This vignette method allows actions in the context and it uncovers everyday practices for a care process. The vignette method comes close their personal experiences of the work in PHC and the structured questions of care management (a named contact person or a team, the use of a treatment plan and shared decision making between care providers and the patient) related the chronic care model.
The data collection in the Finnish health centres was performed in four large or medium-sized cities between 13 October and 26 November 2014. To ensure the trustworthiness of the fictitious patient the survey was piloted with additional physicians. In the final form the survey was shortened according these physicians' suggestions.
The survey included both structured and open-ended questions regarding the care management and different professionals participating in the fictitious patient care process (Table 1). In order to achieve narratives related to the contents of the care processes, we asked: ‘Briefly describe (using either text or a graph) both the patient care process at your health centre and cooperation outside the centre’.
The vignette presents a patient with multiple care needs from both health and social care services.

Data analysis
Responses were recorded, and we calculated percentages from the structured questions and used content analysis to draft the figures of care process. Content analysis can divide data according to interest: either as ‘latent content’ or ‘manifest content’. This study focused on ‘manifest content’ where the interest is in what is obvious in the material and what this tells about the topic being studied. 27 Figure 1 explains the analysis and measurements of the care process. The care process represents a simplified reality at micro level according to the key informants. For example the answer ‘The patient first comes to the doctor. The next appointment is with the specialist psychiatric nurse. The patient has the option to attend online therapy. The patient has to contact the social sector herself’ was reduced to the following care process: GP, online therapy, specialist psychiatric nurse. Each part of the care process was coded to its own variable in spreadsheet software by the first author. Some of the codes were mentioned several times. Those codes mentioned rarely were combined into larger entities. The care processes were divided into groups by sorting them according first contact and the length of care processes (organised from the shortest to the longest), and given running number for each. Furthermore the care processes were presented in a fourfold table by GP/RN and referral to special health care yes/no (Figure 2). The icons used in Figure 2 were designed to describe professionals' consulting hours. Every profession has a specific colour, for example red indicates an RN and is labelled with the initialism RN. The consultations have been depicted using people's profiles and teamwork using full faces. The icons for referrals depict a sheet of paper, with the background colour indicating the profession. Additionally, one icon represents patient contact by phone and another represents a laboratory visit.
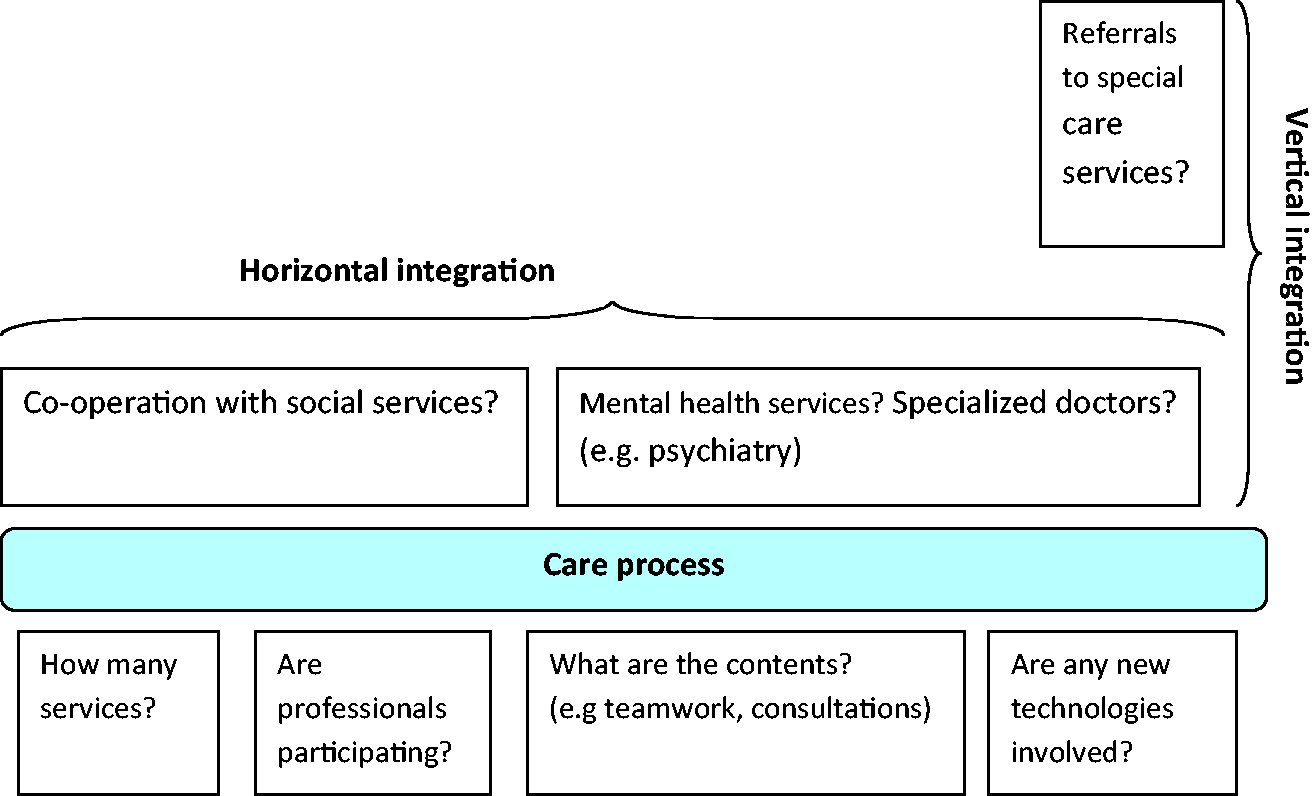
The measurements of a care process include several elements: (1a) co-operation with social services (horizontal integration), (1b) Mental health services, integration of care within PHC, (1c) The professionals participating to the process, contents and use of new technologies, (2) Referrals to special care services (vertical integration).
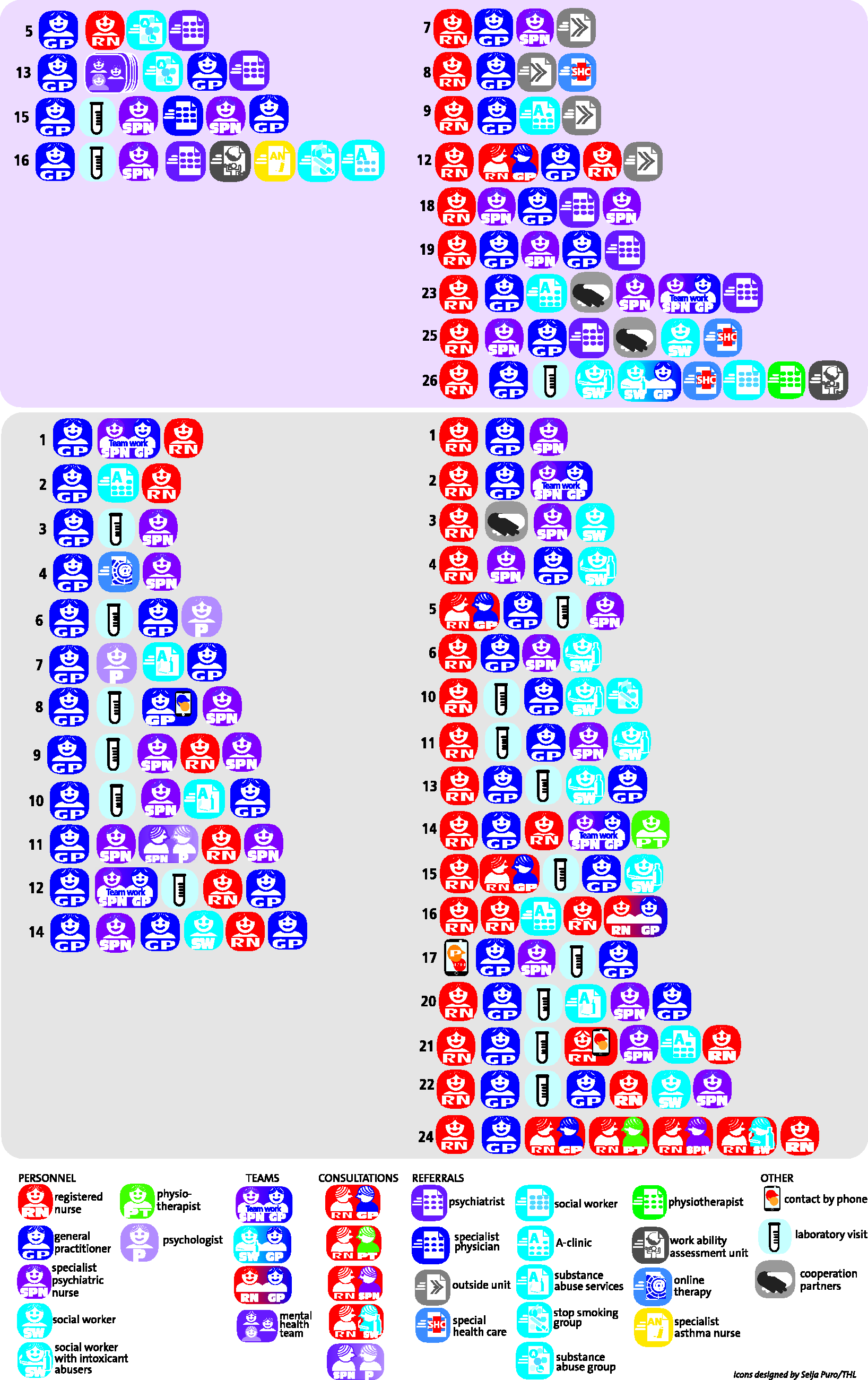
The variation in the care process at a health centre and cooperation outside the health centre for a fictitious patient with multiple care needs. The upper part includes care processes that contain a referral to special health care and the lower part those without divided by the running number of care process by general practitioner and registered nurse. The initialisms used within the icons are detailed below.
Study population
GPs (n = 31) and RNs (n = 31) working daily in Finnish health centres located in four cities. These key informants were given the survey, which included the vignette (Figure 3).
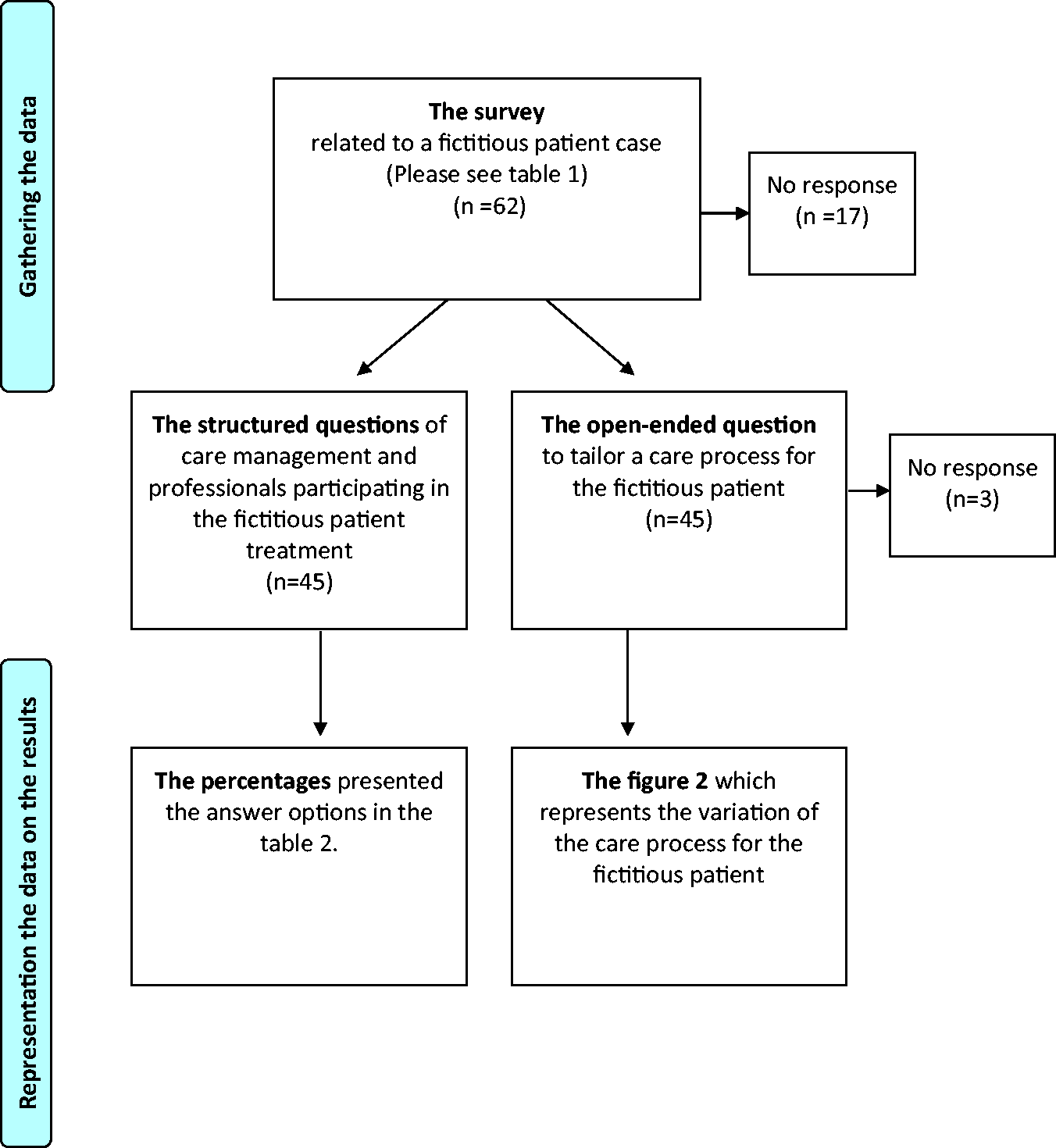
The flow diagram of data collection.
Ethics approval
The ethical approval for a project called Client-centred Primary Care was granted by the Ethical Review Board of the National Institute for Health and Welfare.
Results
The response rate for the survey was 72%. Table 2 presents the structured questions and the options for answering related to the patient in the vignette with multiple care needs. Techniques to support the patient in managing her condition varied, but lifestyle counselling by an RN was quite often proposed. The patient's active involvement in developing a treatment plan was proposed by half of respondents but a written treatment plan was proposed less often.
The results of the structural questions about the care coordination relate to fictitious patient called ‘Jenny’ in a vignette.
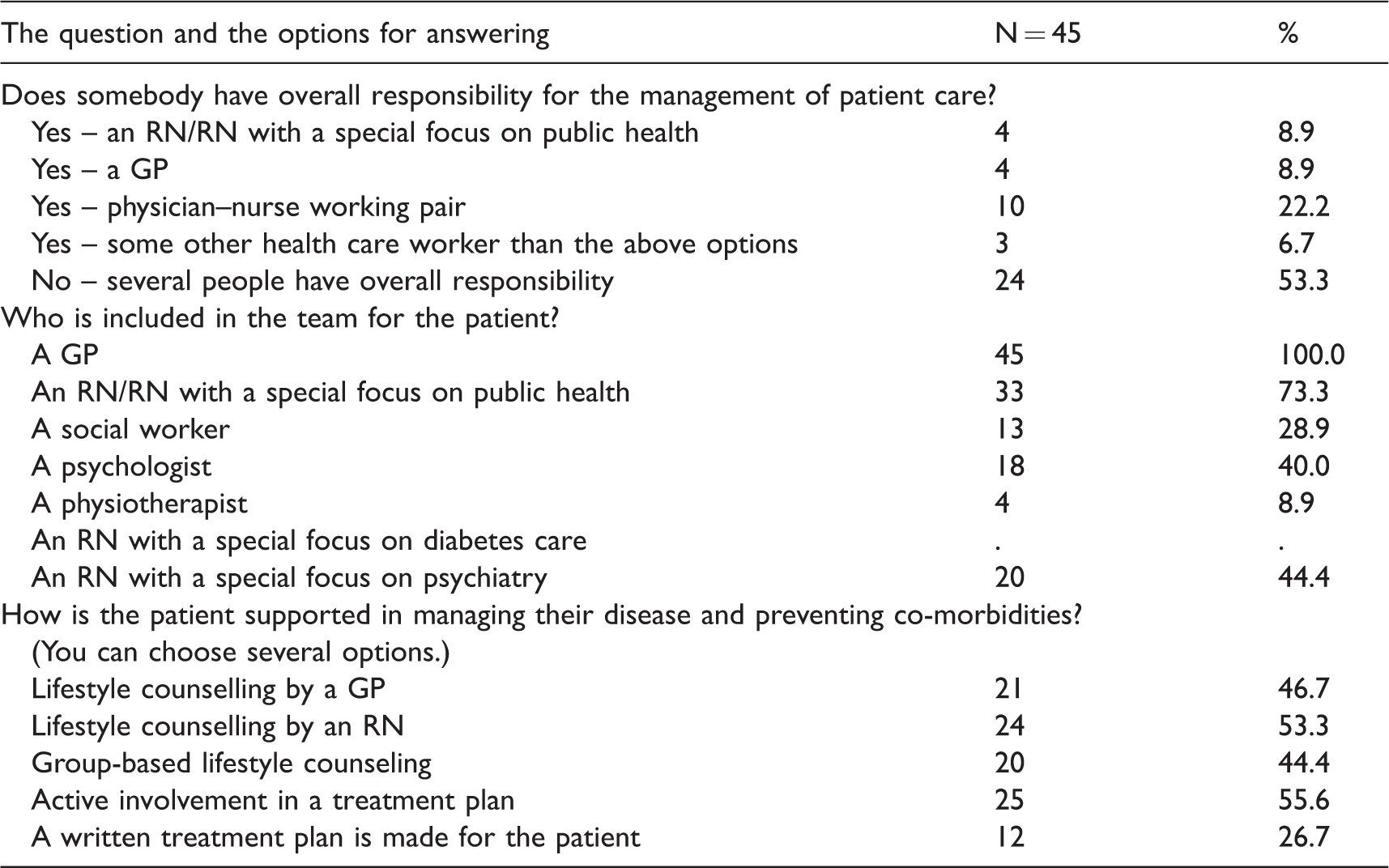
GP: general practitioner; RN: registered nurse.
When the respondents were asked to ‘Briefly describe (using either text or a graph) both the patient treatment process at your health centre and cooperation outside the centre’ they (n = 42) often described the care process as beginning with an RN appointment (62%) while and a care process beginning with a GP appointment was used as well (Figure 2). The number of services tailored to the patient's care process varied between three and nine. The care processes possessed in a fourfold table by the first contact (GP or RN) and by the referral to special health care ‘yes’ (the upper part) or ‘no’ (the lower part). Referral to psychiatric consultation was the most commonly used specialised care included in the treatment processes.
Table 3 shows the implemented elements of the planned care processes. Co-operation with social services was mentioned sometimes and a referral to various types of misuse services within social services was implemented for the care processes too (Figure 2 and Table 3). Vertical integration took place in a third of the care processes which included referrals to special care services (Table 3). In some cases, mental health services were provided within PHC (Table 3). Patient contact took place mostly face to face while the use of mobile solutions (5%) or web-based solutions (2%) were rarely mentioned.
The grouping the care processes by GP or RN and according the elements included in it.
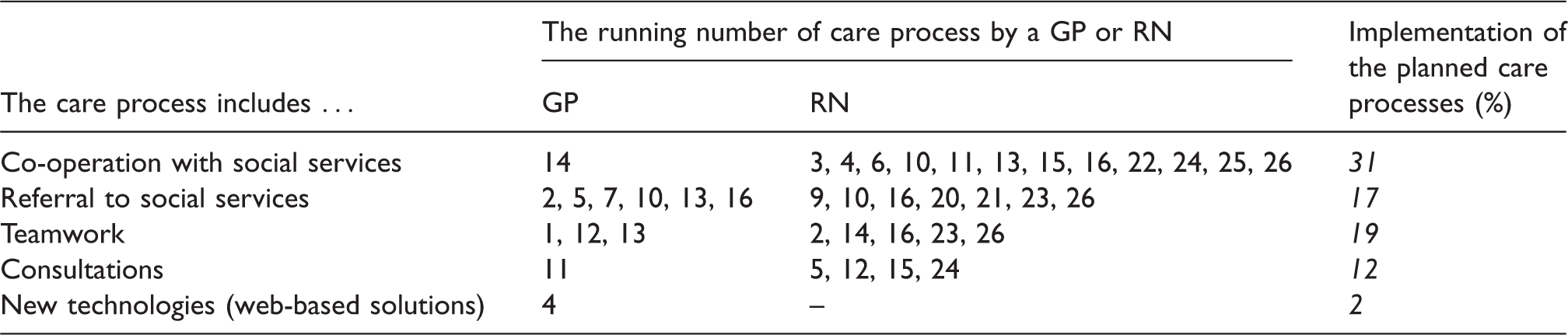
Note: The running numbers of the care processes are presented in Figure 2.
Care process decisions were not made entirely by GPs or RNs since the resources available and context wherein the health care centre is located have influence on care decisions. The data examples below represent the active segmentation process in two municipalities/cities that centralised patients with a high-level care needs for services in one health centre. The health centre staffed with a multiprofessional team aimed at the provision of integrated care for these patients. ‘If the criteria for high care needs were fulfilled, the patient would be sent to another health centre, where patients with high care needs are concentrated. (RN)’ ‘The patient would be allocated a named nurse, who would be able to coordinate the care and reserve her appointments with the GP. In the follow-up treatment, the nurse can act in accordance with the instructions and evaluate the outcomes of the treatment. The nurse can refer Jenny to other workers if needed. The treatment plan is drawn up together with the GP. Referrals to and consultations with specialized health care providers are done through the GP. (RN) ’ ‘Today, such patients are directed to a GP, who makes an assessment of the situation. In the future, the first contact is going to be a nurse. They will then be the gatekeepers to visits to the GP or alternatively patients will be redirected to another nurse. Service guidance will be given regarding mental health and substance misuse services. (GP) ’ ‘The patient would visit a nurse who manages the treatment. Firstly, the nurse would carry out AUDIT, measure blood pressure, the BMI etc. Secondly, a specialist psychiatric nurse would meet the patient, have a discussion and assess the situation (measure the BDI, AUDIT). If there is moderate or severe depression, the patient would meet a GP and, if necessary, a psychiatrist. (RN)
Discussion
In the study we investigated which elements were included to the care process of a fictitious patient with a substantial care needs. The analyses suggest that, treatment practices and the range of professionals participating in the hypothetical patient care for a patient with substantial care needs vary considerably in terms of care processes, the collaboration with social services was relatively uncommon and involving the patient in the treatment plan did not happen always.
The central finding in this study was that the treatment practices and the range of professionals participating in the hypothetical patient care for a patient with substantial care needs vary considerably in terms of care processes. This result is partly explained by the fact that the professionals' contribution to the care processes reflects the staff available at their organisation. Some health centres only have GPs and RNs, while others have a large range of professionals, such as psychiatric nurses, physiotherapists and/or psychologists. The cases where no single person or a named team was in charge of the care process awoke a concern about the continuity of the care. Some of the care processes included multiprofessional care teams focused on the treatment of depression or more general treatment of mental health problems. The professions involved in the care teams vary: some include a GP with an RN, or a GP and a specialist psychiatric nurse, while others also include a psychologist or a social worker. When comparing these findings with those of other countries, it is important to note that the nurse-driven work model in health centres is specific to Finnish solutions in PHC 7 but collaboration with mental health workers has been piloted widely. 28
Another central finding was that collaboration with social services was relatively uncommon and occasional, although it can be expected that patients would benefit from comprehensive care that also takes unemployment and people with substance misuse problems into account. Some care processes included referrals to psychiatrists or A-clinics, following the guidelines.29,30 In terms of co-operation with substance misuse services, health centre personnel often found it difficult to identify whom to contact. 13 The collaboration between health and social care has been challenged with substance misuse problems also in Sweden. 31
Patient contact mostly took place face to face while the use of mobile or web-based solutions in interaction are expected to increase as a result of the digitalisation of health services. Group-based lifestyle counselling was included in some of the care processes, reflecting existing practices and resources. Group-based methods are widely used in the treatment of substance misuse 30 where, in general, the intensive treatment interventions have been shown to be more effective than short-term interventions. 29 Group-based lifestyle counselling provides patients with the possibility to give and receive peer support. The organisation of a care processes is linked to the available resources and guidelines, as well as house rules and the education of the health care professionals. 26
When implemented into practice (as the chronic care model suggests 26 ) personalised care planning can improve a person's physical and psychological health status, 14 and a patient's active involvement in his or her treatment plan and activities is an important dimension of PHC.15,16 In relation to the patient in the vignette with multiple care needs, there is room for improvement in evidence-based practice when involving the patient in the treatment plan.
The scale of the intervention that is tailored to the patient with multiple care needs varies; some care processes would include three services while others may entail up to nine. We cannot say which care processes are best and a single solution is not necessarily needed or applicable. Furthermore, this study was not designed to test differences in connection with care processes for the patient with multiple care needs, the question was whether the attempts to treat such a patient properly are enough or whether the patient will return to emergency room. One point of discussion is whether these care processes affect the crucial Finnish problem of PHC (namely the poor access to care) and, if so, how they affect the problem. Another point for consideration is whether the access to care will be improved if the efforts to coordinate care – a treatment plan, named contact person or team, collaboration with social services – are fulfilled. In other words, does the patient receive the right services, in the right order, at the right time and in the right setting? 24 Additionally the nurse-driven work model 7 may be a part of the solution to facilitating access to PHC. Solutions described in the care processes were not solely dependent on decisions made at the health centres, but they were often linked to decisions made at municipality level, for example, the decision to concentrate the treatment of patients with several chronic conditions at a certain health centre in the city. The results from earlier studies suggest that the variation found related to patients with long-term conditions usually means that there is scope to focus on developing preventative activities and management strategies 32 and this might be a relevant interpretation related to the patient with multiple care needs also.
The referrals to secondary care represent horizontal integration in the care processes. Referral practices varied between the care processes; in general the tendency to write a referral was moderate. It is possible that the multiprofessional staffing in the health centre may decrease the tendency. GPs play a key role as the gatekeepers of access to secondary care in Finland. In different settings, a wide range of GP referral rates has been demonstrated.26,33
In this study, we focused on management continuity but, from the patient point of view, relational continuity (for example, seeing the same RN every time) is just as important.16,20,34 Further studies should address this aspect of continuity more closely. Next-step data from patients need to be collected to get their views on care coordination and to be able to compare their views with those of the health care professionals. Informational continuity could be maintained by better electronic patient records and an improvement in overall information systems architecture, 19 which would improve the flow of patient information between service providers.3,17,18 The information exchange is an elementary part of the care coordination. 24
The results suggest that only every second health care professional described patients as being actively involved in designing their treatment plans. However, an essential tool in the chronic care model is a treatment plan, thus a treatment plan as such is not a new invention. 26 Patients with a personalised treatment plan have been found to be more satisfied with the treatment from their GP than patients who do not have a care plan. 15 The customer interface is the place where good management can prevent both treatment from overlapping and unnecessary tests being taken, thus facilitating knowledge exchange and helping to save costs.3,34 On the basis of the findings, we argue that improving patient involvement in making their treatment plans is important for strengthening patient commitment to a treatment plan, facilitating the elements of continuity of care16,34 and improving care results.
In this study, we were interested in the management of the care process. To this end we developed icons to represent the elements and actors in the care process and used them to depict the variations of the care process offered to the patient with multiple care needs (need in both social and health care services). The vignette method offered a tool with which to map a variety of everyday practices and the different solutions using horizontal integration and vertical integration, including integration within PHC and mental health services. The vignette method allows key informants to describe the services available, for example they might describe a team with a social worker and GP or a work ability assessment unit. The vignette method includes the risk that respondents' answers reflect treatment in accordance with a gold standard rather than actual care process in the health centre, but the scale of the delivered treatment plans were similar to those of health centre users with a chronic condition, 15 and in this respect it can be argued that the responses describe everyday reality. The case of the frequent attender we presented involves the potential for high variation in treatment practices compared with low variation cases (e.g. hip fracture, acute myocardial infarction), where the diagnosis is clear and evidence-based health services are needed. 25 The amount of variation included in the care process of the fictitious patient case with multiple care needs was surprising, and it is possible that more data are needed to reach full sampling saturation. However there is reason to suppose that the description and analysis of a fictitious patient case gives inspiration to reflection on and develop treatment practices in PHC.
Concluding comments
The study showed that there was a substantial variation in the care process tailored to the very same fictitious patient with multiple care needs. The results of this study draw attention to three aspects of the care process that need to be addressed in order to improve continuity of care and patients' chances to be involved in care: a written treatment plan, close collaboration between health and social care services, and a named contact person to avoid care gaps. These innovations are most likely transferable to various healthcare systems.
Footnotes
Acknowledgements
The authors would like to thank a research assistant who made an important contribution to the acquisition of data and Seija Puro, who did the artwork of the icons.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The research was conducted in Client-centred Primary Health Care – Patient Choice And Care Integration-Project (No. 40291) funded by the Finnish Funding Agency for Technology and Innovation (Tekes), and Competent Workforce for the Future-Project (No. 303605) funded by the Strategic Research Council (SRC) at the Academy of Finland.