
Abstract
Introduction
Recent literature has explored the use of hormone replacement therapy (HRT) in menopausal women experiencing psychosis. Menopause women with previous psychotic events in their lifetime experience psychotic symptoms at later peak due to the low estrogen production in their bodies, known as menopause-associated psychosis, which can potentially be improved with the help of HRT. This review aims to discuss the effects of HRT on menopausal women with psychosis by comparing studies with combination of antipsychotic drugs.
Methods
A literature review using Ovid Medline search was used.
Results
These results indicate that HRT may have a positive impact on mood and cognition to decrease the expression of psychotic signs. Some estrogen-derived treatments, such as SERM (selective estrogen receptor modulator), might also improve the impact of the antipsychotics, giving the possibility of dosage reduction and fewer side effects.
Conclusion
Since the management of psychosis is challenging in menopausal women due to hormonal change and antipsychotic adjustment dosage, interdisciplinary management involving psychiatry, gynecology, and family medicine specialities is crucial. This approach can manage the hormonal, psychiatric, and overall medical issues of these patients, provide better psychiatric care, and improve their quality of life. Further research should validate the HRT protocols along with the enhancement of the technique when used in combination with antipsychotic drugs.
Introduction
Women can experience a second peak of new onset psychosis during the menopausal transition, also known as menopause-associated psychosis (MAP). 1 One leading hypothesis suggests that reduced estrogen in menopause removes the protection factor against psychotic symptoms, such as by increasing the dopaminergic responsivity in the striatum. 1 While MAP is widely recognized, 1 the mechanisms connecting low estrogen levels with psychosis remain unclear. Other results also showed that estrogen is neuroprotective in women with schizophrenia during two different peaks, such as first one between 25 and 35 years and a second one between 45 and 50 years.1,2 Previous studies demonstrated that women prior to perimenopause require less hospitalization compared to men, function better overall, and have less negative and cognitive symptoms.3,4 Sommer et al. showed that women below 45 years respond better to reduced doses of antipsychotics to help prevent psychosis relapse compared to men of the same age or women above 45. 5 However, an adjustment of antipsychotic dosage may be required for women experiencing an exacerbation of perimenopause.6,7 Women in perimenopause (around age 45) may experience worsening psychosis, leading to increased hospitalizations and higher antipsychotic dosages. However, limited quantity and quality of existing data have investigated the impact of hormonal replacement therapy (HRT) to help improve the quality of life of menopausal women with psychosis. We hypothesize that neuroprotection by estrogen replacement may be useful when its deficiency in menopausal women increases the risk for psychosis with escalation of symptoms that may need intricate intervention. This research paper is a literature review that highlights the benefits associated with HRT in women undergoing menopause with psychotic disorders, in combination with antipsychotic drugs.
Psychosis peaks by gender and age
Menopausal women experience a higher peak of psychotic symptoms than men, likely because of hormonal fluctuations and declining estrogen levels. According to González-Rodríguez et al., 4 women with schizophrenia show a later age of onset than men and experience a second peak towards the end of their reproductive age. Culbert et al. 8 suggest that both men and women have a first peak of psychosis in early adulthood. They also mention that a second peak of psychosis occurs in mid-life women aged between 40 and 50 years, with a higher risk of hospitalization than men in this age group. For those who already have psychosis prior to menopause, their symptoms are increased despite usual antipsychotics doses. Moreover, some women without a prior history of psychosis may experience new-onset psychosis during perimenopause, representing a second peak in the incidence of schizophrenia. 8 And both are due to the estrogen hypothesis, stating that estrogen is protective against psychosis and that protection is no longer there with the decrease of estrogen happening in perimenopause and menopause. The process of menopause may predispose to midlife psychosis in women due to estrogen loss. Culbert et al. 8 also suggested that women with schizophrenia tend to have ovarian hormonal shifts with irregular menstruation and anovulation, that result in low levels of estradiol below reference range. This is indeed exacerbated when estradiol continues to drop at menopause and worsening psychosis symptoms. These hormonal changes can worsen cognitive as well as emotional symptoms and thus increase vulnerability to psychotic disorders for menopausal women. 7 The data suggests that exogenous estrogen or HRT could help rise the effects of low estrogen and avert psychotic and cognitive side effects. 9 Treating psychotic disorders, especially during menopause, requires a gender-specific approach, highlighting the potential benefits of HRT in alleviating symptoms.
Relation between estrogen, psychosis, and antipsychotics in menopause
Gonzalez et al. demonstrated in their previous reviews the relationship between estrogen, schizophrenia, and antipsychotics.6,7 The reduction in ovarian estradiol (E2) during perimenopause and menopause leads to hippocampal and parietal cortex shrinkage, negatively impacting cognitive function, as estradiol plays a neuroprotective role. The role of estrogen also helps to reduce dopamine levels in the brain. 1 Lower estradiol levels during menopause may lead to higher dopamine levels, increasing the risk of psychosis relapse in women. Gonzalez et al. 7 also mentioned that women in general tend to have more D2 receptor binding sites than men and that estrogen increases the antipsychotic action via those receptors. Reduced levels of estrogen in menopause reduce the D2 receptor occupation by antipsychotics which negatively impact their potential to reduce psychotic symptoms.
Another review by Gonzalez et al. 7 reported that the symptom level in women with schizophrenia increases after menopause for several reasons such as estradiol loss, but, importantly, there is a loss of efficacy that is estrogen-dependent such as in CYP enzymes drug metabolism and adipose tissue redistribution.
Another cohort study nationwide in Finland investigated the use of monoantipsychotics (clozapine, olanzapine, risperidone, or quetiapine) and psychosis relapse in men and women with SSD (n = 61 889) and divided as per age group (difference by 5 years). 5 Increasing antipsychotic dosage in this age group, even with clozapine and olanzapine which are very powerful antipsychotic medications, does not provide any benefits in preventing hospitalizations. Due to reduced estrogen levels during menopause, authors suggest that women with SSD would benefit from HRT and SERMs, which mimic the effects of estrogen in the brain.
HRT and menopause psychosis
Research data support the idea that HRT helps to improve psychotic and cognitive symptoms in women who experience menopause. According to González-Rodríguez et al., postmenopausal estrogen levels significantly reduce the efficacy of antipsychotics and increase psychotic symptoms. 6 This change in hormones may aggravate psychosis, and it becomes challenging to manage schizophrenia or related conditions during a menopausal phase in women. Thus, they recommended adding HRT in junction with antipsychotics to help improve psychotic symptoms.
Similarly, Reilly and McCutcheon support these results and argue that menopausal hormone therapy might decrease relapse psychosis rates in menopausal women. 9 They also note promising evidence for HRT, which may increase well-being. Menopausal women with psychotic disorders still receive inadequate treatment. It outlines an inadequacy in the practices and a need to raise awareness about HRT as one option for treatment.
Methods
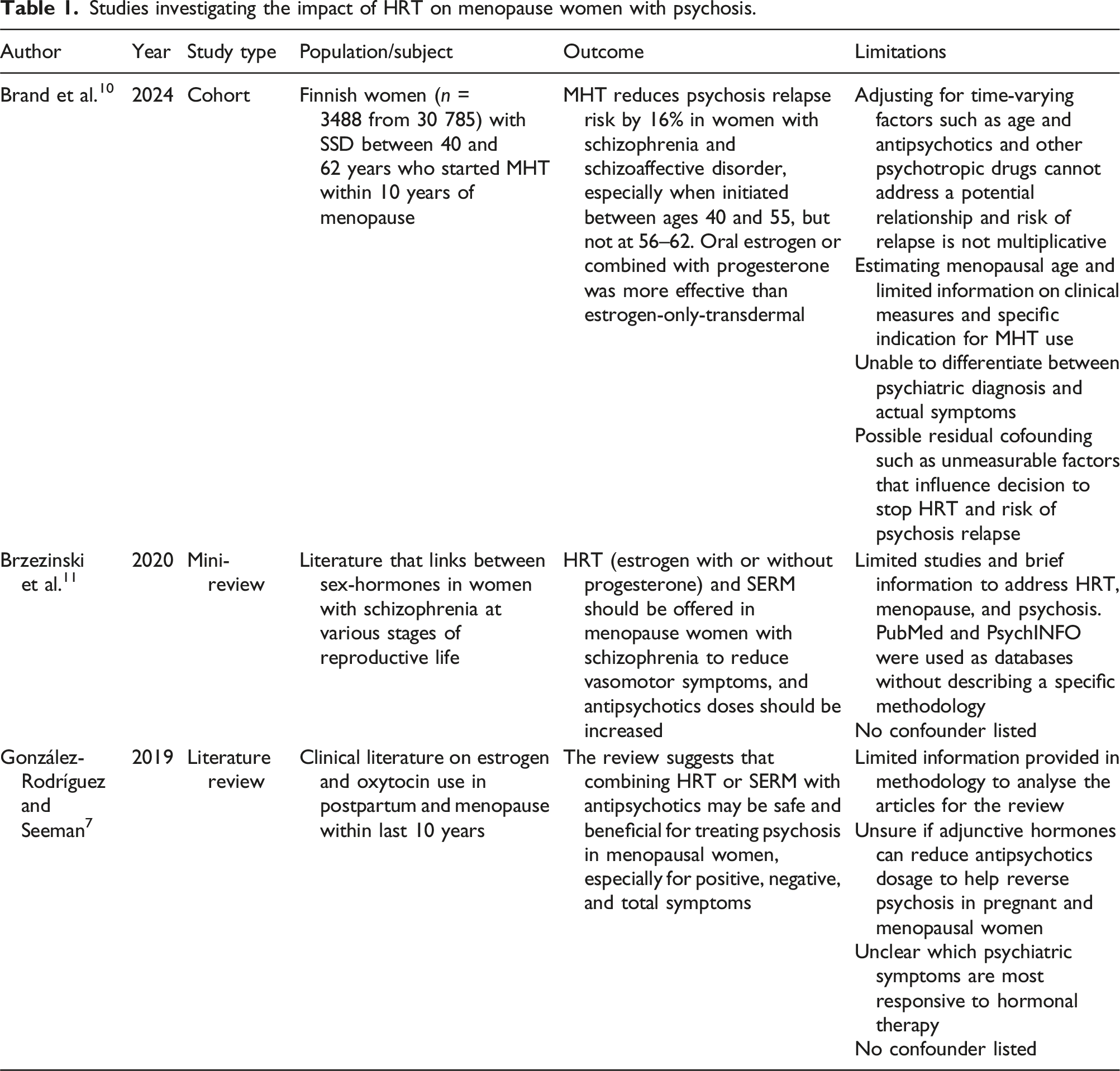
Studies investigating the impact of HRT on menopause women with psychosis.
Results
In this review, three articles investigated the impact of HRT on menopausal women with psychosis.
Brand et al. conducted a cohort study design in Finland (n = 3488 from 30 785) and observed that the impact of different types of HRT reduces the chances of psychotic relapse by 16% in women with schizophrenia or schizophrenic affective disorder (SSD). 10 These results reflect to women aged between 40 and 49 (0.78–0.95) and 50–55 (0.66–0.83) at 95% CI, but not when HRT was started between 56 and 62 (0.91–1.37). Brand et al. also found that estrogen-only formulation, fixed, and sequential combined formulation decreased the psychosis relapse risk by 14–21%. Estradiol alone, estrogen combined with levonorgestrel (LNG), medroxyprogesterone acetate, or norethisterone seem to be more effective by reducing relapse between 15 and 25%. Moreover, oral estrogen-only formulation significantly decreased the relapse (0.73–0.97), compared to transdermal route (0.75–1.04) at 95% CI. Women in this study may also have switched different antipsychotics (oral or injectables) during their follow-ups, although not addressed. Limited information on HRT cessation and psychosis relapse was provided in the article. Other mood disorders may have been present in menopausal women with SSD and which were not addressed in this study.
Brzezinski et al. conducted a mini-review in which they investigated the link between sex-hormones in women with schizophrenia at various stages of life, such as menopause. 11 Just as healthy women, women with schizophrenia during menopause experience vasomotor and psychosocial symptoms. In parallel, psychotic symptoms worsen in women with schizophrenia during menopause which impacts their quality of life. This review suggested the use of estrogen therapy, with or without progestogen, to be the most effective in menopausal women with schizophrenia, as per regular management of menopause symptoms, including the use of SERM’s with an increase of antipsychotic doses. Authors also suggested having a close monitoring of breast and cardiovascular changes, and avoiding drugs that can raise prolactin levels. Although this mini-review states that HRT in menopausal women with psychosis is the most effective treatment, it provides limited evidence.
According to González-Rodríguez and Seeman, they have suggested to lower antipsychotic dosages in menopausal women with psychosis already undergoing HRT to avoid the side effects related to high dosages such as cardiovascular disease, weight gain, sleep disturbance, and muscle/joint pain. 7 Another study by Seeman reported that females had 50–75% more chances of having side effects with antipsychotics than males and respond better with lower doses. 12 Side effects included weight gain, metabolic symptoms, sexual dysfunctions, and cardiac arrhythmias. They also suggested that women’s psychotic symptoms respond better than men at lower doses.
According to González-Rodríguez and Seeman, they mentioned that the use of estradiol was superior to placebo for positive, negative, and general symptoms in postmenopausal women with schizophrenia. 7 Raloxifene, a selective estrogen receptor modulator (SERM), was superior for positive, negative, and total symptoms but not for affective or cognitive function. HRT may have synergistic effects with antipsychotic medications, presumably because estrogen stabilizes and has an impact on neuro-pathways that mediate mood and cognition affected in psychosis. However, because some menopausal women are hypersensitive to estrogen and psychiatric agents, doses of HRT and antipsychotics must be adjusted when prescribed concurrently to mitigate the substantial risk of interactions. 7 For instance, there are antipsychotics that are paired with estrogen, such as clozapine and olanzapine. When estrogen levels decrease in menopause, clozapine and olanzapine also decrease and exogenous estrogen or SERM would rise their levels. Adipose tissue in menopause also reduces the efficacy of lipophilic drugs such as antipsychotics. HRT combination will also help achieve a better dosage of antipsychotic drugs and provide more effective treatment of both psychoses and menopausal disorders which will contribute to the patient’s quality of life. The methodology section of this article provided limited information to analyse the included studies. Authors were also unsure if HRT combination would help reduce antipsychotic dosages to help reverse psychosis in menopausal women. It was also unclear which psychotic symptoms were responding the most to HRT.
Discussion
Up to date, not many studies have investigated the use of HRT on menopausal women with psychosis. One of the explanations can be due to safety concerns around HRT. The use of HRT declined drastically in the first decade of century due to reports linking HRT to an increased risk of coronary artery disease, ischemic stroke, and breast cancer. 10 Later studies have shown the potential benefits of HRT when started within 10 years of menopause which is promising for future studies when combined with antipsychotics in menopausal women with psychosis. 10
Brand et al. were the first to assess different types of HRT and to assess their impact on relapse psychosis in menopausal women, suggesting that oral estrogen-only and in combination with progesterone to be an effective method in addition with antipsychotic use. 10 One of the possible explanations can be due to possible estrogen replacement to help correct the leading hypothesis as described earlier. This may decrease dopaminergic responsiveness and potentially improve MAP.
When estrogen is combined with dydrogesterone, a neutral progestogen with a similar structure to progesterone, a more favourable risk profile for breast cancer, cardiovascular, and venous thromboembolism is observed, compared to LNG which is a synthetic progestogen. 13 Although levonorgestrel may help psychosis, it can be associated with exacerbation of depression and premenstrual dysphoric disorder (PMDD), a severe form of premenstrual syndrome (PMS) in some patients. 14
Weiser et al. have also investigated the impact of HRT in women with SSD, but in reproductive age (n = 100 and age median of 38). Their results have shown that HRT improved psychotic symptoms when using 200 μg of estradiol patch twice a week in adjunct with their antipsychotic medication when using the PANSS (Positive and Negative Syndrome Scale). 15 The placebo group without estradiol patch had a higher score of PANSS of 14.4 compared to the experiment group at 13.4. This is in contrast with Brand et al. results in which the transdermal patch in menopausal women with psychosis did not show an improvement. 10 However, the authors attribute these results to a poor statistical power in the transdermal patch compared to oral estrogen only. One of the possible explanations would be that exogenous estradiol starts to become effective when endogenous estradiol decreases, or estrogen receptors become more sensitive during the menopausal transition. 15
When women experience low estrogen levels, they experience worsening psychotic symptoms. 16 There will be a point in life where people with schizophrenia, regardless of gender, exhibit a limit or no response to antipsychotics. Hence, previous data recommend adding exogenous estrogens to help with the efficacy of antipsychotics. 16 The addition of estradiol becomes beneficial to improving cognition in ageing women with schizophrenia.
Finally, Gonzalez et al. reported that the use of HRT in menopausal women with schizophrenia improves vasomotor symptoms, whether diagnosed with a psychotic disorder or not. 17 Their article also stated that HRT will improve psychotic symptoms in some. Future studies are suggested to explore specific routes and dosages for HRT to help improve MAP.
Conclusion
Preliminary findings suggest that HRT may play a role in managing psychosis in menopausal women, but further research is needed to establish its efficacy and safety. This review showed that HRT contributes to a decrease in psychosis relapse rates and the stabilization of the mood when combined with antipsychotics in menopausal women. However, the incorporation of HRT into psychiatric treatment involves careful consideration since the medication has unique side effects and interactions concerning antipsychotic dosages. This review may potentially encourage psychiatrists, gynecologists, and family physicians to work as a multidisciplinary team to address both the hormonal and psychiatric messages that these patients have. This multisystemic effort is significant as these patients suffer from both hormonal and psychiatric disorders. We recommend that future studies investigate which type of HRT and antipsychotics would be more appropriate in reducing psychosis relapse in menopausal women, with the goal of establishing standardized treatment protocols and promoting different medical doctors collaboration.
Footnotes
Acknowledgements
We would like to thank the psychiatric department of Montfort Hospital for their support and recognition of the importance of this project.
Contributorship
NS and VD were involved in the conception and design of this manuscript. NS wrote the first draft of the manuscript. VD revised and gave the final approval of this version to be published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
VD.