
Abstract
Objective
To determine whether a staff menopause clinic would benefit our peri/postmenopausal hospital workforce.
Methods
The three menopause consultants, with OH administration assistance, set up a virtual clinic for staff members to address the unanswered need for access to good menopause care. Feedback was gathered from the attendees and the staff who ran the clinic.
Results
The clinic was an overwhelming success and has now become an established clinic at a major London teaching hospital.
Conclusions
We hope that this model can be used in other trusts, and other companies to provide good menopause care to our senior female workforce to retain them. Acknowledgements: We would like to thank the OH staff who ensured the clinics ran so smoothly.
Introduction
In the NHS workforce nearly 50% of the working population are women in the 45–65 age group. Currently many women are leaving or considering leaving the NHS because of menopausal symptoms and/or Covid consequences. Access to HRT for women was already difficult before the pandemic but now this is even more challenging and many General Practices are reluctant to prescribe HRT. Women take HRT to relieve their symptoms of estrogen deficiency and to protect against the long term effects of ovarian failure eg. osteoporosis, cardiovascular disease, Parkinson’s disease, dementia etc. NHS England/Improvement are currently rolling out a programme to retain women in the NHS workforce by providing information on the optimal pathways for menopausal care.
As clinicians running the Guy’s and St Thomas’s NHS Hospital Trust (GSTT) menopause clinic we were very aware of peri/postmenopausal colleagues who were retiring early and the resultant significant loss to the workforce. We therefore felt that we would like to contribute to the NHSE/I programme by giving our GSTT staff access to menopausal experts to discuss their individual situations and give advice. We had already done large group information meetings to staff and managers, (male and female) but many women were not happy to divulge their personal situation to others and preferred a one-to-one consultation. We had regular monthly webinars on women’s health issues that were well attended and evaluated, and the evaluations suggested a one to one clinic would be helpful for the staff in the Trust.
Discussions around menopause can normally occur in primary care but many practices are not comfortable to prescribe HRT without expert advice and particularly now, it is challenging for a postmenopausal woman to get an appointment in primary care for a non-acute, or non “red flag” problem. We therefore set up menopause clinics purely for GSTT staff to attend, with the hope that if this model worked, it could be adopted by other trusts.
Aims
To provide a holistic consultation for staff members who are suffering from perimenopausal or menopausal symptoms within our trust and offer them a chance to speak to menopause experts with the aim of improving their health and wellbeing so they do not leave the NHS workforce, particularly at this challenging time.
This was also an ideal time to assess lifestyle and risk factors for future health.
We also wanted to assess the demand for these staff clinics and subsequent satisfaction with appointments
The original plan of NHSE/I was to target nursing staff as they are the female majority but we welcomed any female staff whatever job or location they had at GSTT. By making the clinics virtual we were able to cover all the areas including community staff.
Methodology
Staff Menopause clinic pre appointment questionnaire.
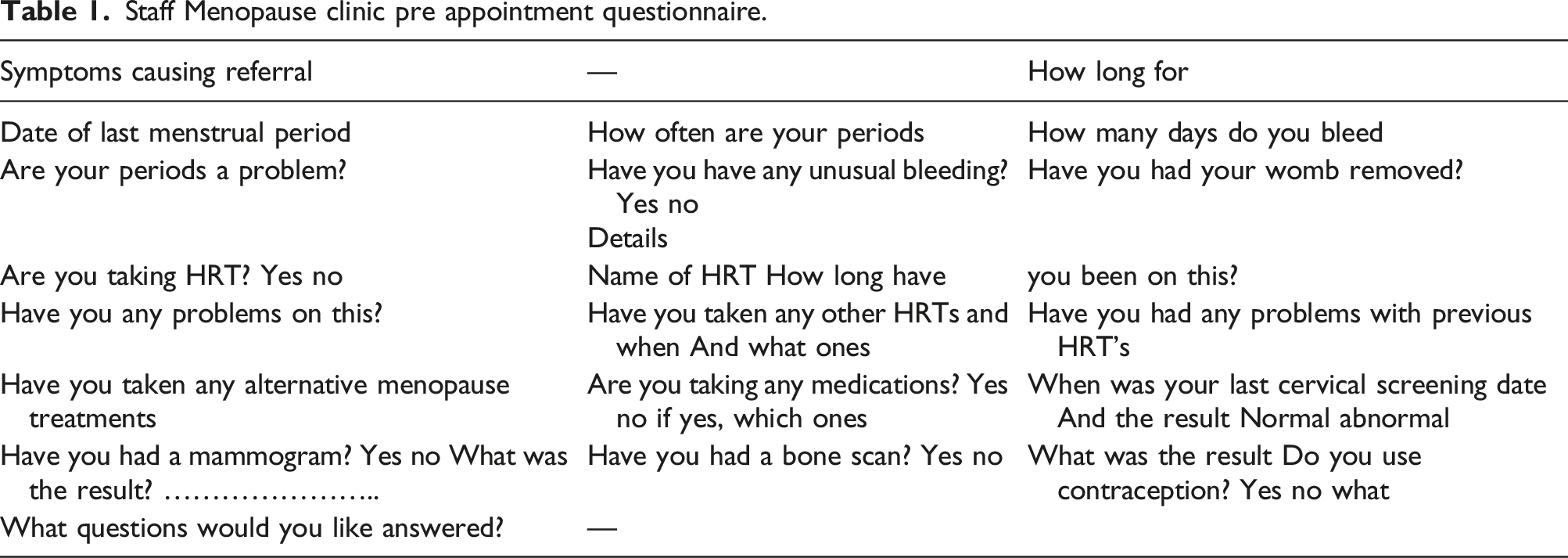
The clinics were done by us (JR,DH,DB) in our own time in the evenings with 15 min appointments, At the end of the appointment we would return the originally submitted form with our advice, to the woman and OH. These records were stored in OH. We advised but did not prescribe, so the woman could take the form to their GP with documentation from a menopause specialist.
If the GP was not happy to prescribe HRT then they could be referred to the menopause clinic, and if their situation was complex (comorbidities) then we would advise referral to the menopause clinic. We had agreement that anything urgent/red flag picked up such as post-menopausal bleeding could be referred straight into the 2 Week Wait service. Following the appointment, the attendee staff members were asked to complete an anonymous survey to provide feedback about their experience. The staff running the clinic were also asked to fill in a questionnaire.
Results
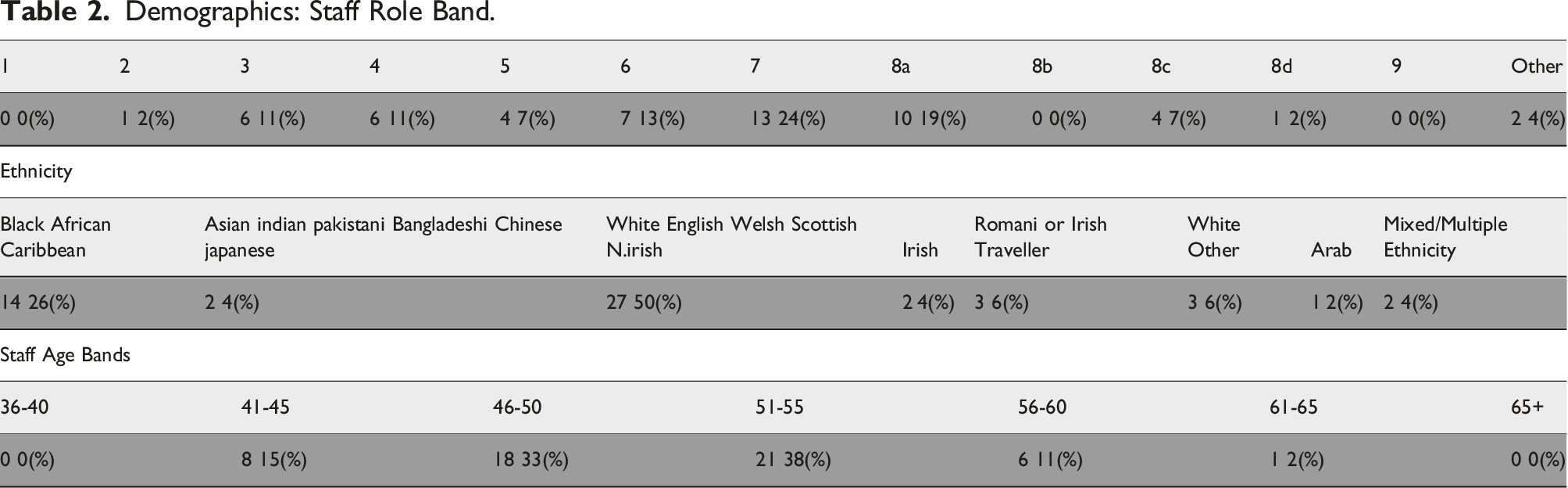
Demographics: Staff Role Band.
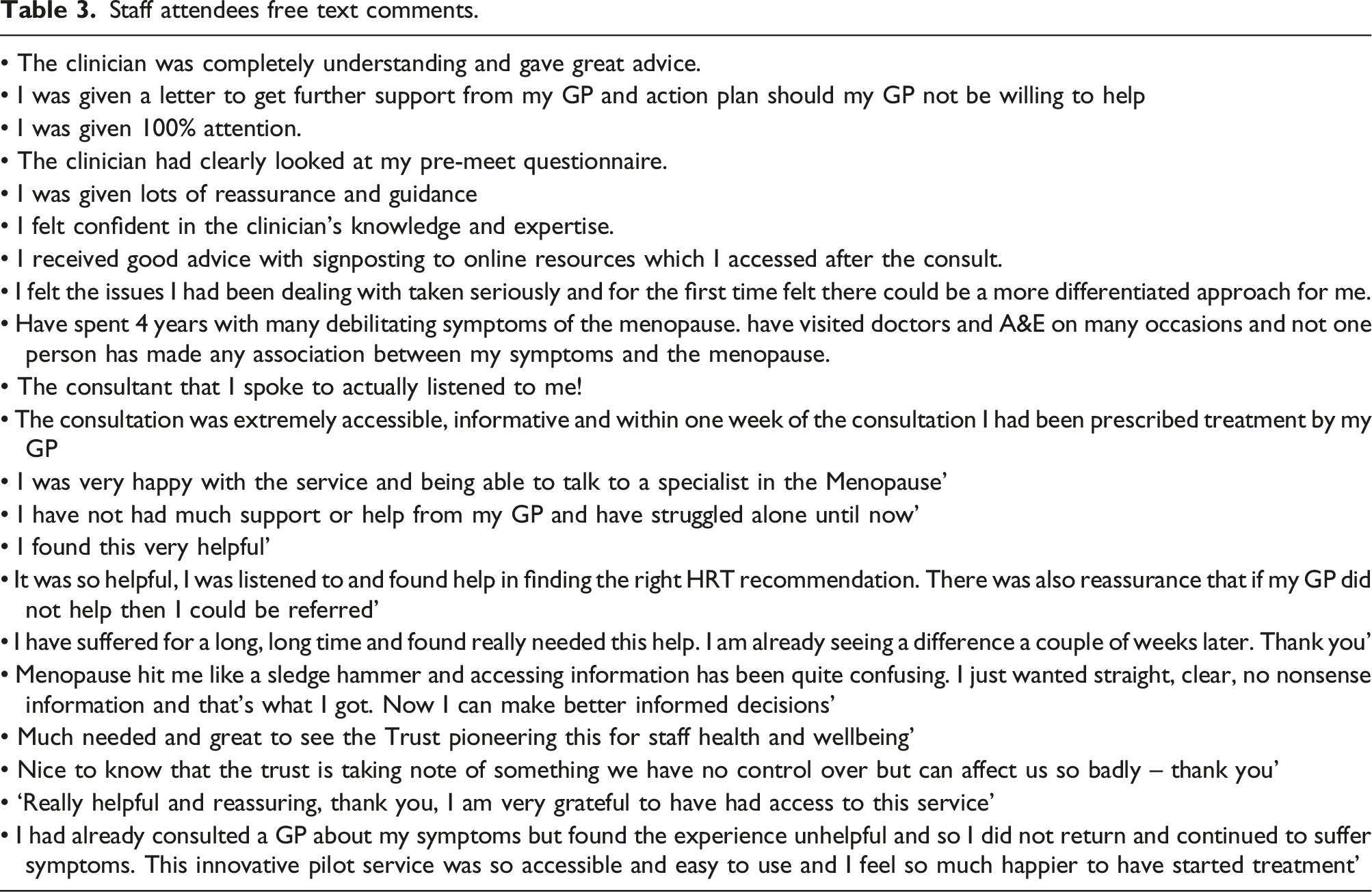
Staff attendees free text comments.
With regards to the staff who ran and organised the clinic – when asked to reflect on the interactions/consultations they had with GSTT staff attendees during this pilot it was 9.8. The staff felt that the pre-questionnaire helped to focus the consultation. The clinic was very rewarding for the staff who ran it is as there was “Ad hoc” positive feedback from participants. Positive comments were spontaneously sent directly to Head of Nursing. Very positive feedback at team meetings/training day presentations of the “Show we care” innovation.
When asked what went well: (1) the booking system (2) asking the patients to fill in the form before attending. (3) Chasing individuals who had not submitted self-referral forms (4) sending across clinic diaries and forms the day before the clinic to the clinicians.
When asked what could be improved (1) Send self-referral form over further in advance – cancel appointments if not sent in 48 h before appointment and put someone in from the waiting list. (2) More lead time of clinic schedules to clinicians. (3) Planned follow up survey post appointment to gauge effectiveness of advice and guidance leading to change/starting of treatment with GP (4) Longer appointment time – 15 min for consult and five to do administration (5) OH to send follow up letters and info out instead of clinicians (6) Variation in timings of clinics to accommodate shift working
Main themes that emerged from feedback from attendees and staff generally about menopause care: (1) Lack of support from and access to GPs. (2) Low level of expertise amongst GPs. (3) Lack of knowledge as to where to get reliable information and guidance.
Conclusions
This innovative clinic for our menopausal staff has been very successful as assessed by patients (staff clinic attenders) and the staff doing the clinics. The plan now is for a fully funded clinic staffed by menopause specialists who currently run the clinics at GSTT or specialists who have been trained in our clinic. We also plan to do an audit of the staff in this pilot study in 6 months to find out how they are and to ascertain what lasting impact this had on their quality of life and working life.
We hope that this provides a useful template for other trusts to adopt so that our peri and postmenopausal workforce can be retained, not only in the NHS but in the wider female workforce.
Footnotes
Acknowledgements
We would like to thank GSTT Occupational Health for their assistance with the administration of the clinic.
Authors’ contribution
JR and DH conceived the idea.
JR, DH and DB did the clinics in their own time.
JB did the statistical analysis and provided the OH support.
JR wrote the first draft of the manuscript.
All authors reviewed and edited the manuscript and approved the final version of the manuscript
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DH has done educational lectures for Gideon Richter and Meditronic JR does educational lectures but all fees are donated to the Kibera Pad company in Kenya to allow young girls to attend their education.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
As this was a pilot clinic there was no ethical approval needed but it was approved by the GSTT “Show we care” committee.
Guarantor
JR