
Abstract
Objective:
This study evaluates and compares Patient-Reported Experience Measures (PREMs) regarding patient satisfaction with urethral catheterisation (UC) and suprapubic catheterisation (SPC) post-robot-assisted radical prostatectomy (RARP).
Methods:
A prospective study was conducted at Queen Elizabeth University Hospital from January 2023 to March 2024 on patients undergoing RARP. Patients received either a UC or SPC, with each surgeon exclusively using one method. A patient preference questionnaire assessed comfort, ease of care, and the quality of pre-/post-operative information. Scoring was based on a visual analogue scale (1–10), categorised as very good (1–3), ok (4–7), or very poor (8–10). Demographic and body mass index (BMI) data were collected. Statistical analysis was performed using the chi-square tests.
Results:
A total of 204 patients were included, with 102 receiving UC and 102 SPC. Discomfort levels differed significantly between groups, with 37.3% of UC patients reporting ‘very good’ comfort versus 87% of SPC patients (p < 0.001). SPC patients also reported significantly higher convenience in care (95.1% versus 63.7% for UC, p < 0.001). Catheter-associated urinary tract infections were minimal (2% for both groups), while 4% of UC patients presented to the emergency department with blocked catheters.
Conclusion:
SPC improves patient experience post-RARP. Further research is needed on long-term outcomes, cost-effectiveness, and early continence recovery.
Level of evidence:
Not applicable
Introduction
Prostate cancer is now the commonest cancer in the male population in the United Kingdom, with prevalence increasing with age. 1 Over the years, surgical techniques for prostatectomy have evolved, and robotic-assisted radical prostatectomy (RARP) has become the gold standard due to its minimally invasive approach, with reduced perioperative morbidity and improved functional outcomes. 2
In the immediate post-operative period, urinary drainage is typically maintained via a urethral catheter (UC) for approximately 7 days. 3 This serves as a protective measure for the vesicourethral anastomosis, facilitating urinary drainage and potentially reducing tension while it heals. However, while UCs are effective, they are not without drawbacks. Many patients report bothersome urinary symptoms, including pain, discomfort, bladder spasms, restricted mobility, and social limitations, all of which can significantly impact quality of life (QoL) during the recovery period.4,5
Although the duration of catheterisation is debated, approximately 5–7 days is widely accepted, as there have been reports of higher incidence of acute urinary retention (AUR) with earlier removal. 6 There has been a move towards using suprapubic catheters (SPCs) as the preferable option for multiple reasons. A recent study compared the use of UC versus SPC in pelvic fascia-sparing RARPs which showed significantly less penile pain and bladder spasms. 7 Achieving post-operative continence has also been shown to be more quickly achieved when using an SPC with higher rates of patients with established continence at removal. 7 It has been theorised that delayed continence in patients with a UC may relate to confidence and the impact it has on QoL. A meta-analysis found a significant improvement in catheter-related problems at day 7 in patients with SPC when compared to UC. 3
When determining the most appropriate catheterisation method, several patient-specific factors must be carefully evaluated, including comorbidities, body mass index (BMI), and dexterity. Patients with high BMI may have technical challenges with SPC placement, whereas those with limited manual dexterity may struggle with self-care and catheter management, influencing the choice between SPC and UC. 8
Studies have demonstrated that strictures and anastomotic leaks do not occur at a higher rate with SPC compared to UC, indicating that SPC is a safe alternative in many cases.3,7,9 In addition, no significant difference has been observed in urinary retention rates or bladder neck strictures between the two methods, 6 further supporting the use of SPC as a viable option.
The primary aim of our study was to evaluate the use of SPC versus UC in RARP regarding patient satisfaction and comfort. Secondary outcomes included complications reported.
Methods
A prospective study was conducted at a single institute from January 2023 to March 2024. Approval was sought from the Urology Consultant Group. Prior to implementation, patient leaflets were produced, and nurses on the ward were trained with the change in practice. Patients who underwent RARP were included and either had a UC or SPC inserted. SPCs were inserted under direct visualisation intra-operatively and were based on surgeon preference. Patients with intra-operative complications, anastomotic leak on intra-operative leak test, or salvage cases were excluded. Two surgeons performed SPC insertion (one performed the traditional anterior approach (Lorenzo Dutto) and the other utilised a Retzius-sparing approach (Imran Ahmad)). The other two surgeons used UC as part of their standard anterior approach.
Patients were counselled on catheter management by nurse specialists and given an information leaflet to support this. UC patients had their catheter remaining on free drainage. SPC patients were instructed to keep the catheter on free drainage (attached to a catheter bag) until post-operative day 1, or when haematuria had settled. After which, the catheter bag was switched for a flip-flo valve, and patients were allowed to void per-urethrally and were instructed on how to check their post-void residue.
A patient preference questionnaire was created, and patients were contacted at least 2 weeks after catheter removal (Figure 1). The questionnaire included questions relating to comfort and ease of care as well as quality of pre- and post-operative information given. Other variables collected included demographics, BMI, and complications. Patients were asked to give an objective score (using a visual analogue scale, 1–10) as well as questions related to complications. Scores of 1 to 3 were categorised into ‘very good’, 4 to 7 as ‘okay’, and 8 to 10 as ‘very poor experience’.
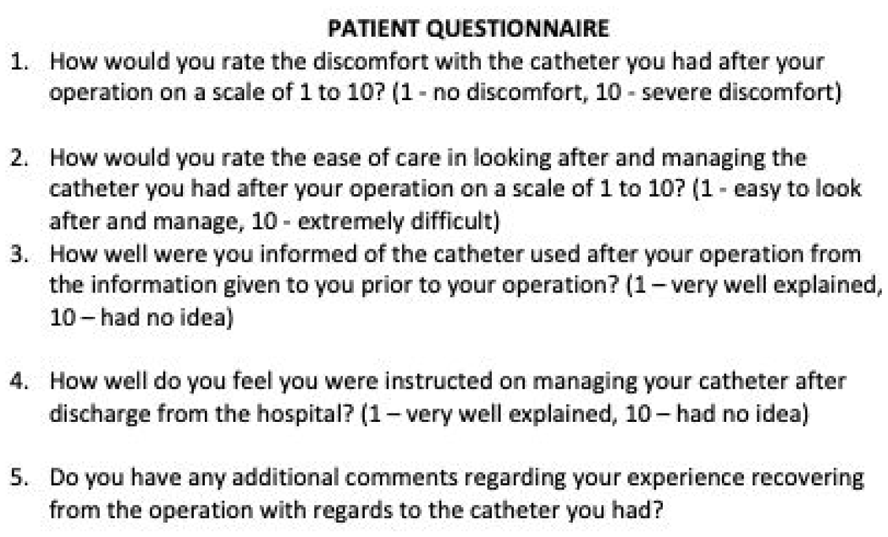
Patient questionnaire used to assess patient catheter experience.
Results were analysed using the chi-square using GraphPad Prism v10.
Results
A total of 204 patients were included in the study – 102 in UC group and 102 patients in the SPC group.
Groups were well matched, and there was no significant difference in median age of patient groups: (UC n = 63 (standard deviation (SD) = 6.3) versus SPC n = 64 (SD = 6.8) (p = 0.277)) (Figure 2) or BMI between patient groups (UC: 28 kg/m2 versus SPC: 29 kg/m2) (p = 0.633) (Figure 3).
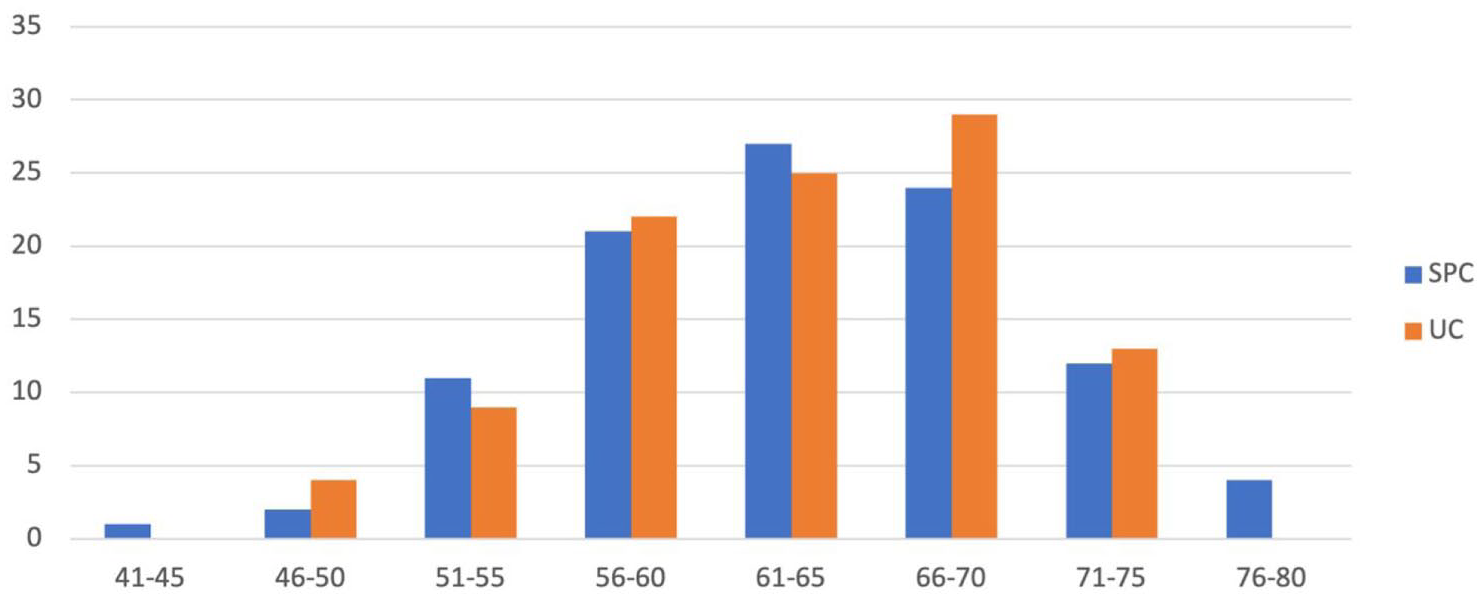
Age distribution of patients undergoing SPC and UC insertion (years).
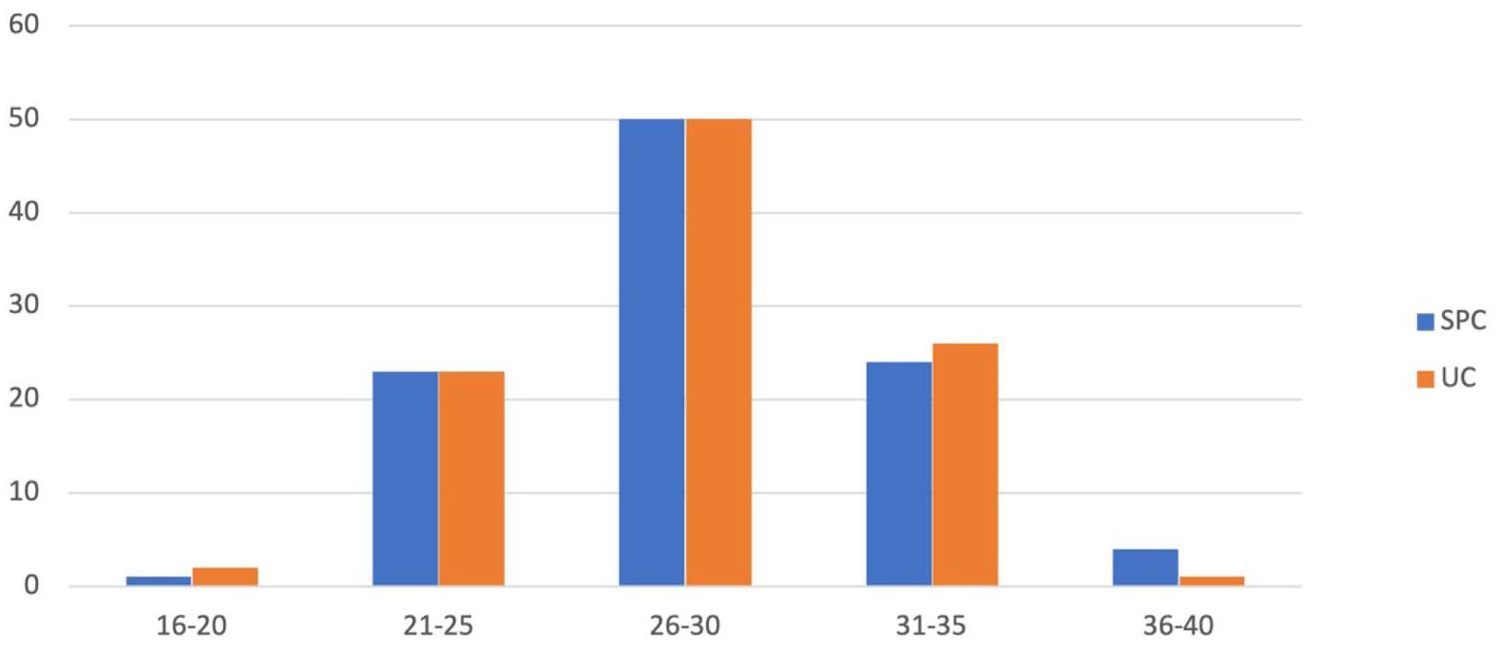
BMI distribution of patients undergoing SPC and UC insertion (kg/m2).
A general trend was observed indicating that both groups reported more positive than negative experiences overall. However, notable differences were evident in the proportions of patients experiencing the highest levels of comfort across different aspects of their care (Figures 4 and 5).
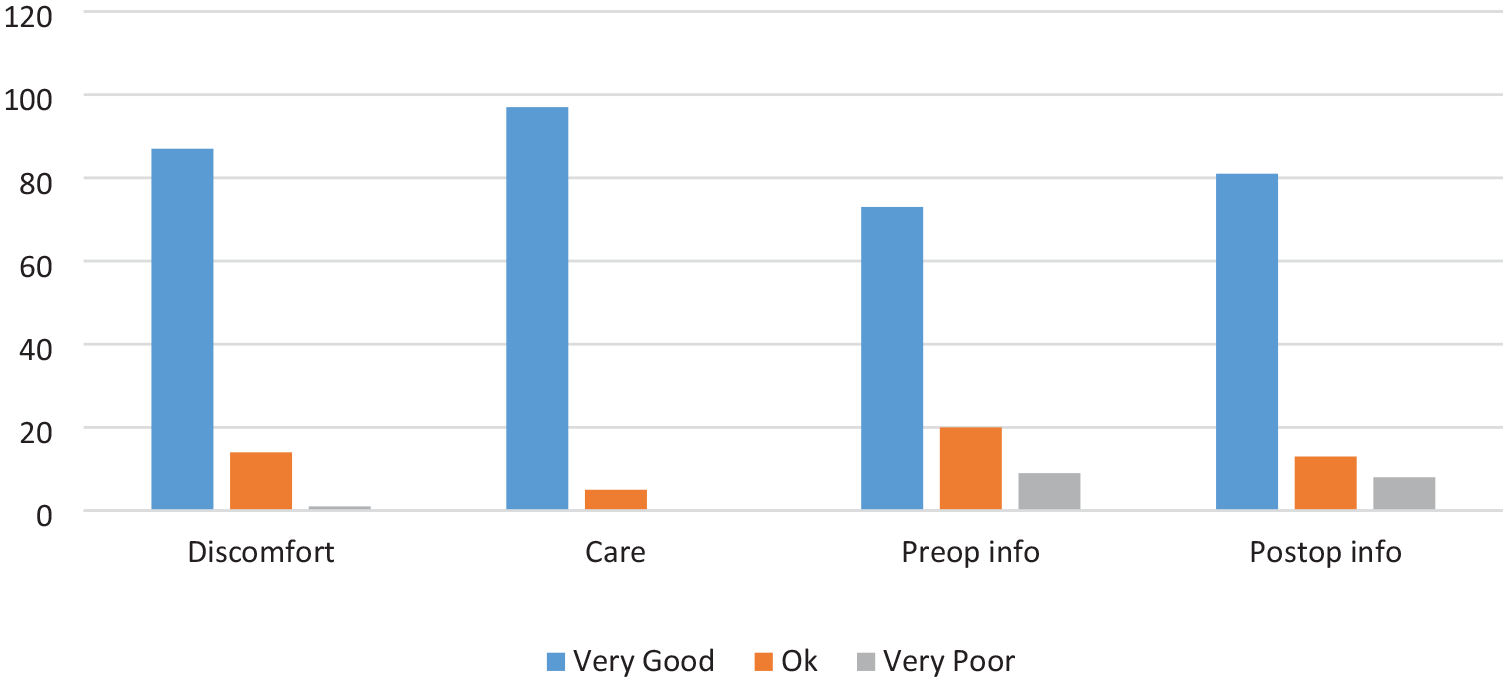
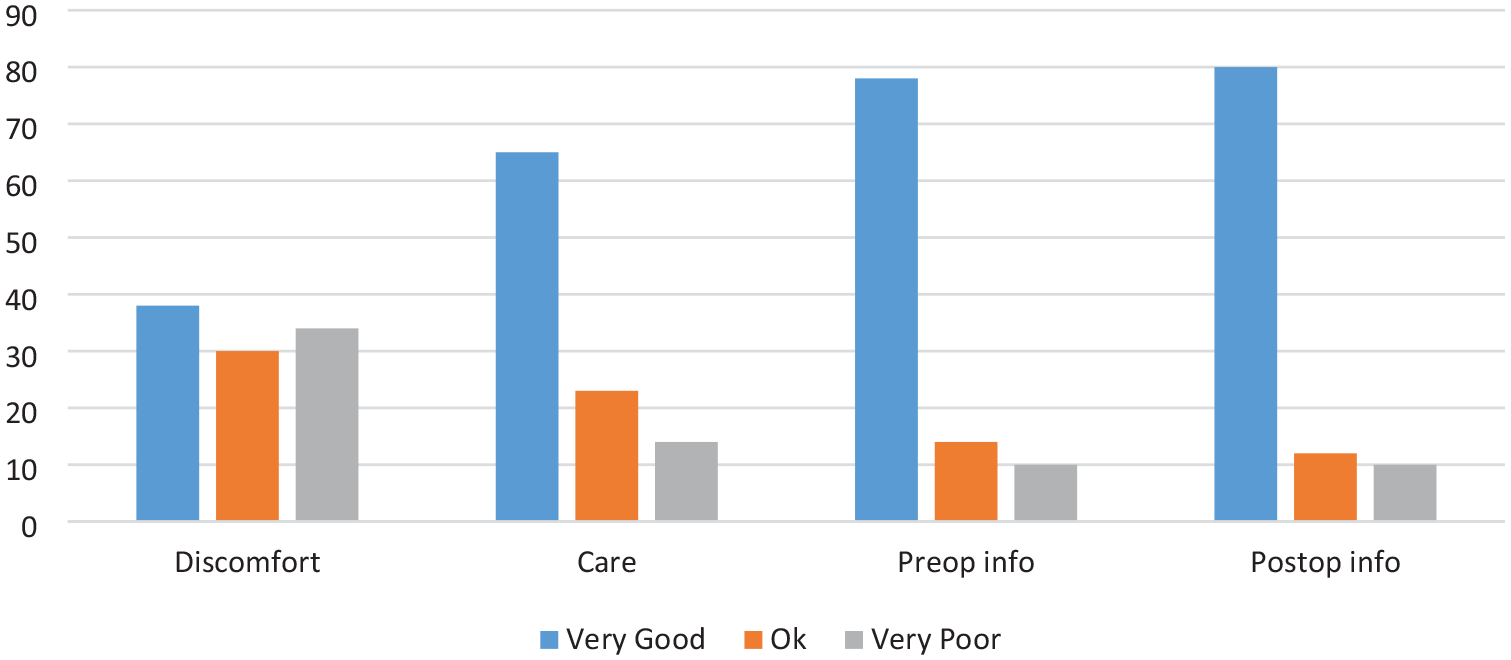
Patient-reported outcomes for UC group showing a high proportion of patients who report discomfort.
Patient-reported outcomes for SPC group showing globally high scores across categories.
Discomfort
The SPC group reported significantly lower levels of discomfort compared to the UC group (Figures 4 and 5). Among SPC patients, 85% rated their experience as ‘very good’, 14% rated it as ‘okay’, and only 1% (1 patient) reported it as ‘poor’. In contrast, the UC group had 37% selecting ‘very good’, 29% selecting ‘okay’, and a notable 33% selecting ‘poor’. These differences were statistically significant (p < 0.001).
Ease of care
SPC patients also reported significantly easier levels of care compared to UC patients. In the SPC group, 95% rated their experience as ‘very good’, with 5% selecting ‘okay’ and no patients reporting their experience as ‘poor’ (Figures 4 and 5). Among UC patients, 64% rated their care as ‘very good’, 23% as ‘okay’, and 14% as ‘poor’. This difference was also highly significant (p < 0.001).
Pre-operative information
Both groups reported similar levels of satisfaction regarding pre-operative information. In the SPC group, 72% rated the information provided as ‘very good’, 20% as ‘okay’, and 9% as ‘poor’ (Figures 4 and 5). Similarly, in the UC group, 78% rated the information as ‘very good’, 12% as ‘okay’, and 10% as ‘poor’. There was no statistically significant difference between the groups in this category (p = 0.305).
Post-operative information
Both groups expressed similar levels of satisfaction with post-operative information. In the SPC group, 79% rated the information as ‘very good’, 13% as ‘okay’, and 9% as ‘poor’ (Figures 4 and 5). Similarly, in the UC group, 78% rated their experience as ‘very good’, 12% as ‘okay’, and 7% as ‘poor’. These differences were not statistically significant (p = 0.874).
Complications
A comparison of complications revealed two cases of infection requiring antibiotics in the SPC group (Clavien Dindo 2). In the UC group, there were two cases of infection requiring antibiotics, two cases of catheter blockage, two complaints of leakage, and one case of urinary retention following removal of catheter requiring re-catheterisation for a prolonged period. None of the patients with an SPC required re-attendance to the local Emergency Department compared to four patients with UC (p = 0.121).
Discussion
Our findings align with emerging literature, indicating that patients generally have a more positive post-operative experience following RARP, with no increased risk of complications. 7 The findings demonstrate significant differences in patient-reported outcomes between SPC and UC groups, highlighting the superior patient experience associated with SPC. These results emphasise the importance of patient comfort, ease of care, and satisfaction with information in optimising post-operative recover following RARP.
SPC patients overwhelmingly reported higher levels of comfort with 85% rating their experience as ‘very good’ compared to just 37% in UC patients. Conversely, 33% of UC patients rated their experience as ‘poor’ compared to only 1% in the SPC group. The difference may be attributed to the anatomical placement of SPC’s, which are less invasive to the urethra, reducing pain and irritation, particularly during ambulation.
Similarly, ease of care was reported to be significantly better among SPC patients, with 95% rating it as ‘very good’. In contrast, 65% of UC patients shared this view, and 14% rated care as ‘poor’. These results suggest that SPC catheters may not only improve patient comfort but also reduce the burden of catheter maintenance, likely contributing to a better overall experience.
Pre-operative and post-operative information satisfaction levels were similar across both groups, indicating that the quality of communication and preparation provided by the healthcare team was consistent regardless of the type of catheter used. While both groups reported high satisfaction with pre-operative information, with around 72–78% rating it as ‘very good’, the remaining proportions rated it as ‘okay’ or ‘poor’. Similarly, post-operative information satisfaction was comparable between groups, with around 79% of SPC patients and 78% of UC patients rating it as ‘very good’. These findings suggest that while patients were generally satisfied with the information provided, there remains room for improvement to ensure that all patients feel fully informed and supported throughout their care journey. Complication rates were similar for infection in both groups of patients examined; however, patients with UC experienced issues with catheter blockage and required attendances to their local Emergency Department.
These results reflect similar findings found in other studies, in which reported the use of an SPC is a safe, comfortable, and viable alternative to UC following an RARP.7,10 There has been no reporting increase in post-operative complications from using an SPC, and in fact, there are lower rates of retention following removal of catheter. 7 Penile pain has been reported to be less as well as better patient satisfaction with an SPC. 10 A meta-analysis has shown that continence is achieved more quickly when using an SPC compared to UC 3 which is an aspect that our study should consider evaluating in the future.
There are limitations associated with the study include an element of selection bias, as patients were not randomised but rather underwent SPC or UC insertion according to surgeon preference. Differences in results may also be attributed to surgeon rather than SPC/UC. The study was also performed at a single site and should be replicated across different units to increase generalisability and ensure that findings are applicable to a broader patient population. In addition, variations in surgical technique and post-procedure care across different centres may influence outcomes, highlighting the need for multicentre studies to validate these results.
This study provides valuable insights into patient experiences with SPC and UC, but it is not without limitations. The reliance on subjective patient-reported outcomes may introduce bias. The focus of the study looked at the immediate post-operative care and did not evaluate long-term impact on continence or erectile function. Future research should aim to incorporate these variables to provide a more comprehensive evaluation of the benefits and risks associated with each catheterisation method.
Conclusion
SPC is superior to UC for patient comfort when recovering from RARP. Our results align with existing literature which demonstrates favourable patient-reported outcomes for robot-assisted laparoscopic prostatectomies. The significant difference in patient comfort and ease of care highlights areas of development for potential standardisation of post-operative pathways which include SPC use.
Footnotes
Acknowledgements
We would like to thank Alison Obeidallah for his assistance and guidance in this research.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cancer Research UK Clinician Scientist Fellowship award to Dr I.A. (C49745/A19661).
Ethical approval
Ethical approval was not required, as the study and research did not involve any new interventions or randomisation. No identifying information was used in the analysis or presentation of the results.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.
Consent to participate
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.
Consent for publication
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.
Data availability statement
All data is available on request.
Guarantor
I.A.
Contributorship
C.R.: data collection, editing, and writing of the manuscript. I.I.: data collection, analysis, and review of the manuscript. L.D.: review of the manuscript. I.A.: review of the manuscript, analysis, and project lead.