
Abstract
Introduction:
Metastatic disease is found in up to 20% of prostate cancer (PCa) cases at diagnosis. Since their introduction in the 1980s, long acting gonadotropin-releasing hormone (GnRH) analogues, administered subcutaneously or intramuscularly every 1–6 months have widely replaced bilateral orchidectomy as the method of castration for this cohort of patients. Recent evidence suggests that surgical castration confers a superior side-effect profile and cost. We aimed to perform a systematic review and meta-analysis to compare these two treatment methods particularly in terms of survival, side-effect profile and cost-effectiveness.
Methods:
A systematic review of the literature was performed for studies comparing medical and surgical castration for metastatic PCa. Outcome measurements included overall survival, side-effect profile and cost.
Results:
Fifteen studies on 63,682 participants (n = 59,045 for medical and n = 4637 for surgical) met inclusion criteria. Our analysis demonstrated a trend towards significance in overall survival rates in favour of surgical castration (hazard ratio = 0.89, 95% confidence interval (CI) = 0.79 to 1.01, p = 0.06), a trend towards significance in cardiovascular complications in favour of the surgical group (odds ratio (OR) = 0.79, 95% CI = 0.62 to 1.00, p = 0.05) and a significantly lower nadir prostate-specific antigen (PSA) level in favour of medical castration (MD PSA 1.17 less in medical castration group, 95% CI = 0.67 to 1.67, p < 0.01).
Conclusion:
Surgical castration appears to be a safe, feasible and efficacious alternative to medical castration, with evidence to suggest a potential survival benefit and limited evidence of a financial benefit in the treatment of men with metastatic PCa. Further studies are required to further quantify the financial burden of one method over another, as well as to identify which subgroup of patients respond best to each method of castration.
Level of evidence:
Level 1
Introduction
Prostate cancer (PCa) is the second most common cancer in men worldwide, with an estimated incidence of 1.2 million cases annually, resulting in 385,000 deaths each year. 1 Despite the increased identification of early, localised PCa through prostate-specific antigen (PSA) testing, metastatic disease is present in up to 20% of cases at diagnosis.2,3 Androgen deprivation therapy (ADT) in the form of either medical castration (MC) or surgical orchidectomy remains the gold standard treatment for metastatic PCa.3,4 The 1980s saw the introduction of long-acting gonadotropin-releasing hormone (GnRH) analogues, administered subcutaneously or intramuscularly every 1–6 months, widely replacing conventional orchidectomy as the treatment of choice for this cohort of patients.5,6
The advent of GnRH analogues saw a reduction in the proportion of men with metastatic PCa being treated operatively. 7 Interestingly, subsequent studies demonstrated no superiority of one treatment modality over another in terms of survival. 7 Irrespective of treatment choice, hypogonadism from ADT is a significant issue, causing a wide range of side effects such as osteoporosis and subsequent fractures, cardiovascular effects, metabolic issues and anaemia.1,7 Recent evidence has emerged suggesting that surgical castration (SC) may offer a more favourable side-effect profile than that of GnRH therapy, particularly resulting in less fractures, peripheral arterial disease and cardiac-related complications. 8 SC also has the advantage of reduced overall cost over long-term follow-up as well as avoiding the adverse oncologic outcomes associated with medication non-compliance.9,10 Evidence on survival benefit has been mixed. Our study aims to shed light on this controversial topic, by gathering and analysing the current evidence in the literature comparing MC and SC, particularly in terms of survival, side-effect profile and cost-effectiveness.
Methods
Study design and reporting guidelines
This study is a systematic review of randomised and non-randomised trials and follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines.
Search strategy
The following databases were searched as part of the systematic review in February 2023: Medline, EMBASE and Web of Science. The systematic search process with detailed search terms are outlined in the Supplementary Material S1. The last date of search was 14 February 2023. The grey literature was also searched to further identify ongoing works of literature.
Inclusion criteria
Studies in English assessing the outcomes of MC versus SC for metastatic prostate cancer were assessed for eligibility based on the following inclusion criteria:
1. Study design:
(a) Randomised controlled trials (RCTs)
(b) Cohort studies
2. Participants:
(a) Patients with castrate-sensitive metastatic prostate cancer
3. Intervention:
(a) Comparison of SC (bilateral orchidectomy) and MC (GnRH analogue)
4. Outcomes:
(a) Primary: overall survival, nadir PSA, nadir testosterone, cost and quality of life (QoL)
(b) Secondary: time to castrate resistance, cardiovascular complications, fractures, gynaecomastia, hot flushes and new-onset type 2 diabetes mellitus (T2DM)
(c) Basic participant characteristics: age, baseline PSA and method of castration
Exclusion criteria
1. Study design:
(a) Case reports
(b) Case series
(c) Conference abstracts
(d) Case–control studies
2. Participants:
(a) Patients undergoing castration for reasons other than metastatic prostate cancer
(b) Patients with castrate-resistant prostate cancer
3. Intervention:
(a) No comparison of MC (GnRH analogue) and SC (bilateral orchidectomy)
4. Outcome:
(a) Qualitative measures only, providing information that is not-comparable by meta-analysis
(b) Unclear outcomes
Study selection, data extraction and critical appraisal
A database was created using the reference managing software EndNote X9™. Two researchers (N.J.O.S. and H.C.T.) reviewed outputs from the searches independently of each other.
Initially, duplicates were removed. Study titles were then screened and assessed for potential relevance. The abstracts of selected potential studies were then read and assessed for eligibility for inclusion, based on the inclusion/exclusion criteria detailed above. Rejected studies were grouped together in the database by their reason for exclusion. The full texts of the abstracts deemed eligible for inclusion were then further analysed using the same criteria. Conflicts between the two reviewers (N.J.O.S. and H.C.T.) were resolved following an open discussion and final decision by the senior author (R.G.C.).
In order to extract and store data efficiently, the Cochrane Collaboration screening and data extraction tool, Covidence, was used. 11 Data were collected by two reviewers (N.J.O.S. and H.C.T.) independently, using the following headings; study details, study design, population, intervention, comparison groups and outcomes. Basic participant characteristics (age, baseline PSA, method of castration) were also extracted. Conflicts between the two reviewers were resolved following an open discussion and final decision by the senior author (R.G.C.).
A critical appraisal of the methodological quality and risk of bias of the included studies was performed. The critical appraisal was completed by two reviewers independently. Quality assessment of non-RCTs was performed according to the Newcastle–Ottawa Scale (NOS). 12 We assigned stars to evaluate study quality: 7 stars – ‘very good’, 5–6 stars ‘good’, 3–4 stars ‘satisfactory’ and 02 stars ‘unsatisfactory’. The critical appraisal was completed by two reviewers independently (N.J.O.S. and H.C.T.). Quality assessment of RCTs was performed using the Cochrane Collaboration risk of bias tool. 13 Furthermore, the certainty of evidence was assessed using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) tool for grading quality of evidence. 14
Data analysis
Statistical analysis was performed using Revman Statistical Software (Version 5 Copenhagen, Denmark). 15 Binary outcome data were reported as odds ratio (OR) and 95% confidence interval (95% CIs) were estimated using the Mantel–Haenszel method. For continuous data, mean differences and 95% CI were estimated using inverse variance weighting. Outcome measures (mean + standard deviation (SD) and median + interquartile range (IQR)) were recorded. If needed, outcome variables (mean and SD) were estimated from the median and range using formula described by Hozo et al. 16 With respect to OS, time-to-effect modelling was performed using the generic-inverse variance method. In brief, OS were expressed as hazard ratios (HRs) and were considered the primary analytical endpoints. HR and each corresponding CI were retrieved directly from included studies for use in this meta-analysis. Heterogeneity was assessed by I2 statistics, with >50% being considered as considerable heterogeneity. Random-effects modelling was applied in cases of increased heterogeneity (>50%) and a fixed-effects model applied otherwise. Statistical significance was attributed to p < 0.05.
Systematic review registration
Our systematic review was registered on PROSPERO in February 2023 (ID: CRD42022339561).
Results
Search results
The literature search described above yielded a total of 4871 results (Supplementary Material S2). Following the removal of 489 duplicates, 4382 studies were screened. After the initial screen, 370 abstracts were reviewed and assessed for eligibility, of which 31 were selected for full-text review. From these 31 full texts, a total of 15 studies met the inclusion criteria, all of which were included in the quantitative analysis.
Methodological characteristics and quality of studies
Nine of the included studies were retrospective cohort studies,3,6 –8,17 –21 three were prospective cohort studies22 –24 and the remaining three were RCTs.25 –27 Table 1 summarises the methodological characteristics of the included studies. All three of the included RCTs were ‘low risk’ of bias for most of the categories, using the Cochrane Collaboration risk of bias assessment for RCTs. All three RCTs failed to provide detailed information in relation to their blinding process, rendering them ‘intermediate risk’ of bias. In regard to non-RCT studies, one study was ‘very good’, six studies were ‘good’, five studies were ‘satisfactory’ and zero studies were ‘unsatisfactory’. Figures summarising the results of these risk of bias assessments can be found in Supplementary Material S3.
Methodological characteristics of the included studies.
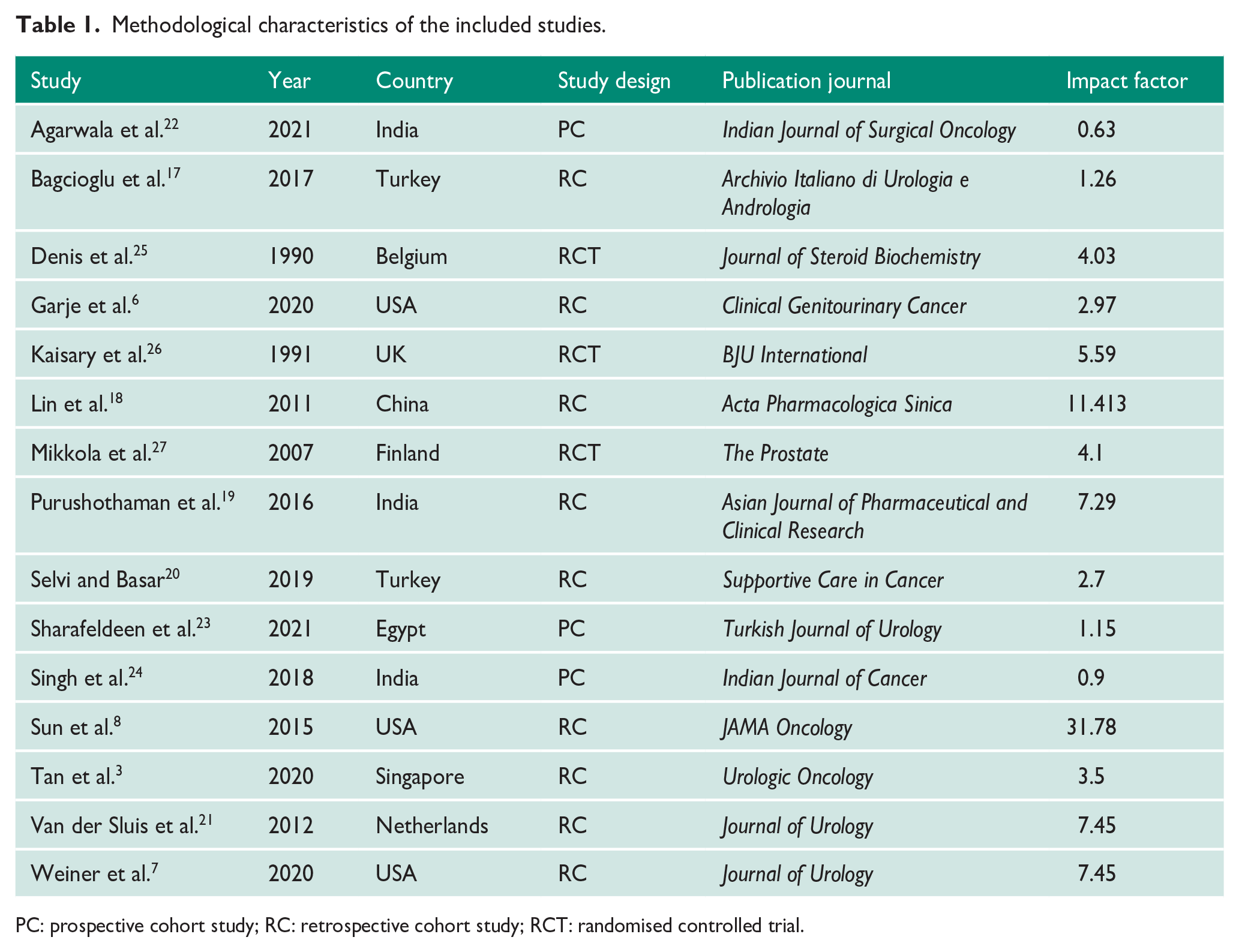
PC: prospective cohort study; RC: retrospective cohort study; RCT: randomised controlled trial.
Participant characteristics
The total number of participants from the 15 included studies was 63,682. Out of 63,682 participants, 92.7% (n = 59,045) underwent MC and the remaining 7.3% (n = 4637) underwent SC for metastatic prostate cancer. Two studies recruited 91.6% of overall patients6,7 One study reported ethnicity breakdown, which included 75.6% white men, 19.9% black men, 3.4% ‘other’ and 1.1% unknown. The baseline characteristics of participants are outlined in Table 2. A precise breakdown of castration method is presented in Table 3.
Baseline characteristics of participants.
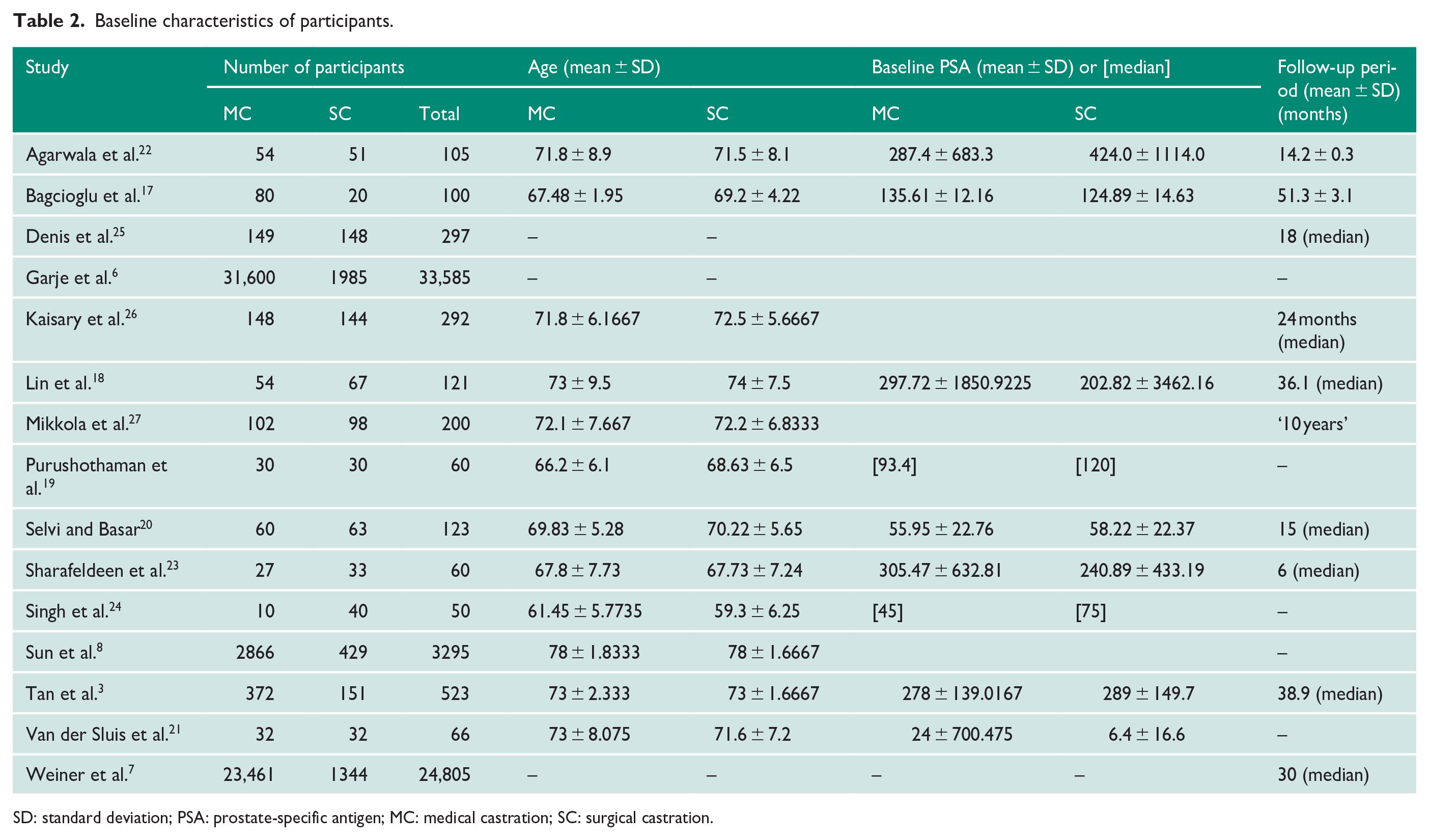
SD: standard deviation; PSA: prostate-specific antigen; MC: medical castration; SC: surgical castration.
Method of castration breakdown.
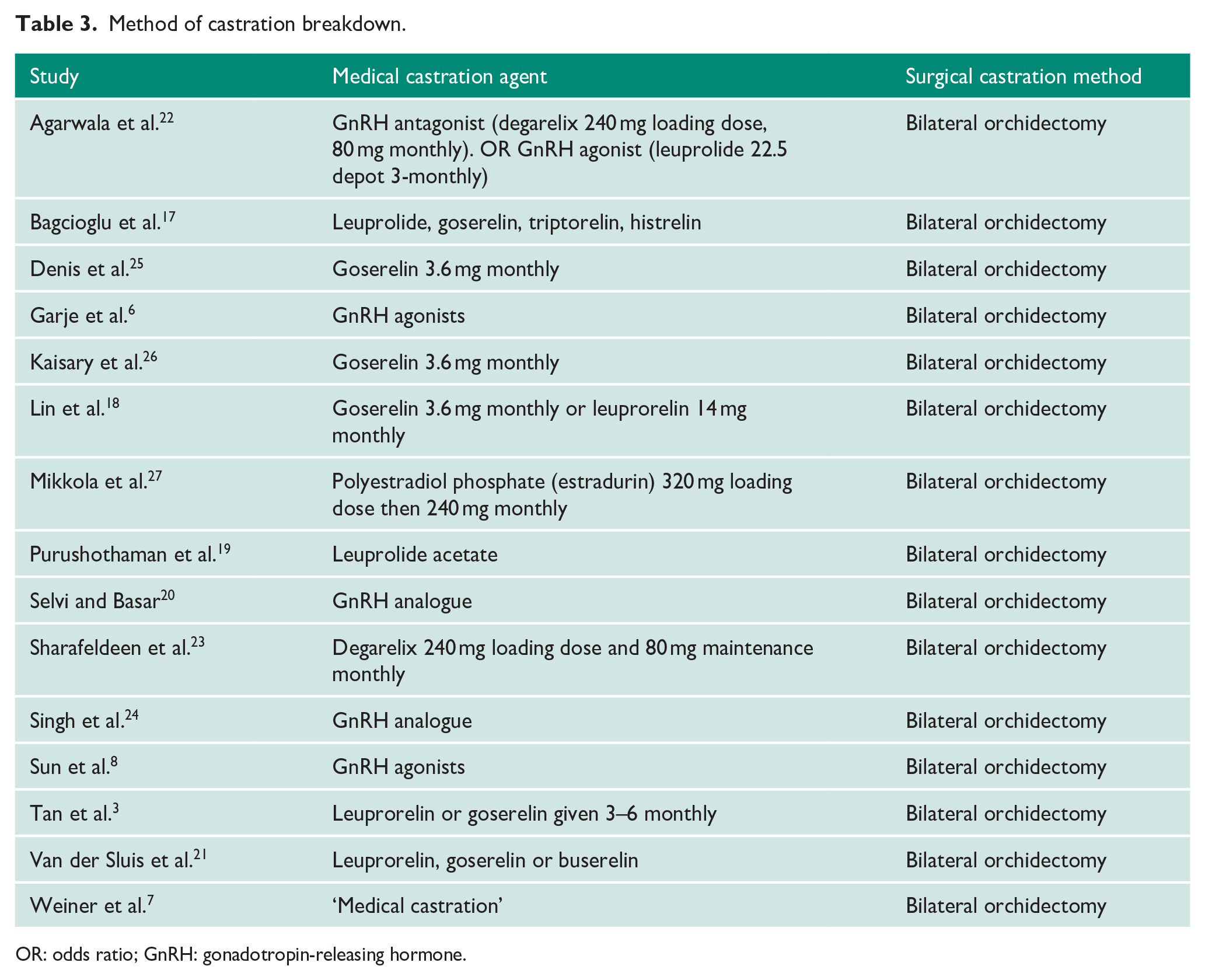
OR: odds ratio; GnRH: gonadotropin-releasing hormone.
Overall survival
Eight studies reported overall survival rates between the two groups. A meta-analysis using a random-effects model demonstrated a trend towards significance in overall survival rates in favour of SC (HR = 0.89, 95% CI = 0.79 to 1.01, p = 0.06), with considerable heterogeneity observed across the included studies (I2 = 69%) (Figure 1(a)).
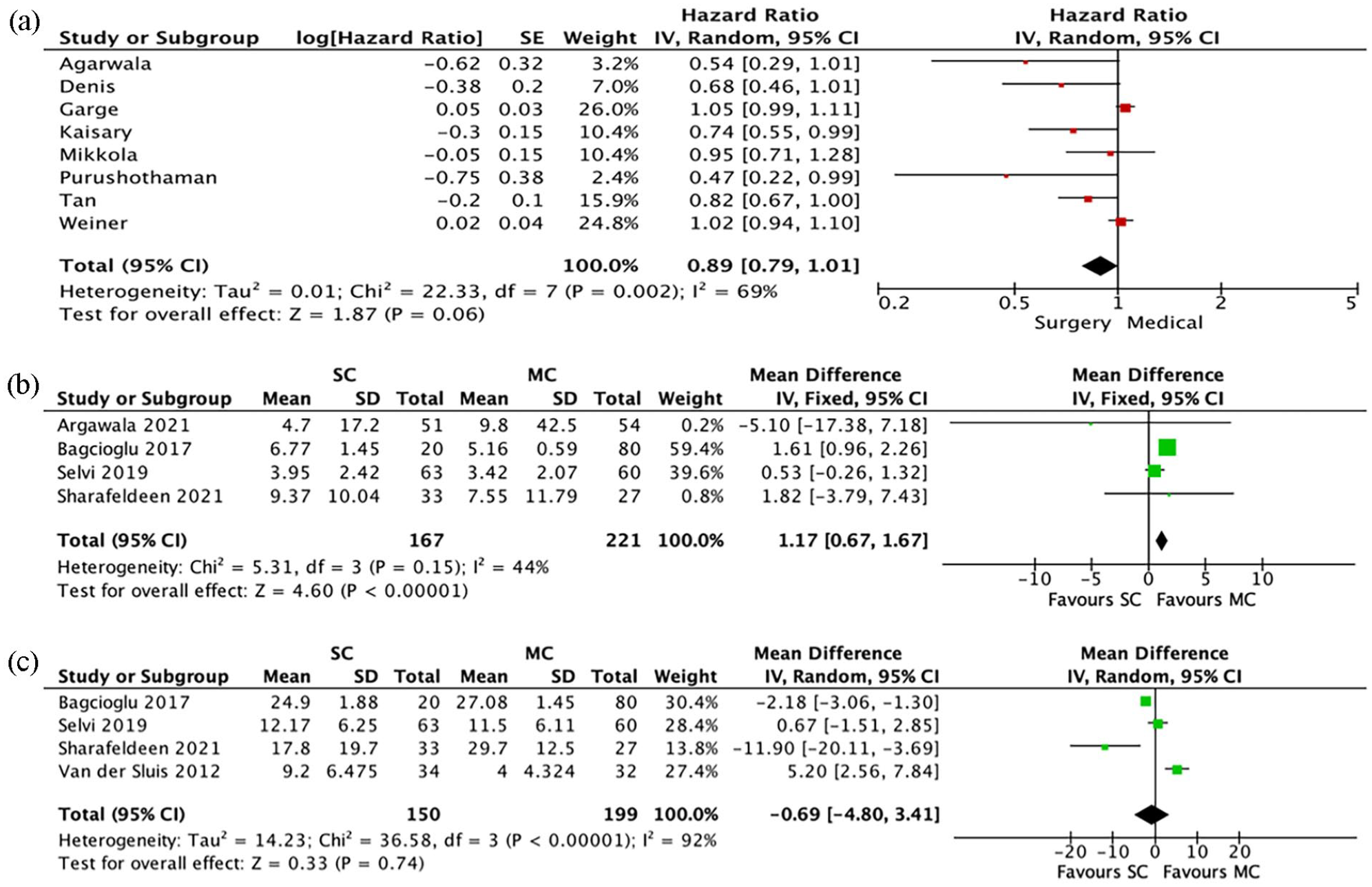
(a)–(c) Meta-analysis results: (a) overall survival, (b) nadir PSA and (c) nadir testosterone.
Nadir PSA
Four studies reported nadir PSA levels of SC and MC groups. A meta-analysis using a fixed-effects model demonstrated a significant difference between the two groups in favour of MC (MD PSA 1.17 less in MC group, 95% CI = 0.67 to 1.67, p < 0.01), with considerable heterogeneity reported across studies (Figure 1(b)).
Nadir testosterone
Four studies reported a comparison of nadir testosterone levels post-castration. A meta-analysis using the random-effects model demonstrated no significant difference between the two groups in regard to this outcome (MD = 0.69 ng/mL less in the SC group, 95% CI = −4.80 to 3.41, p = 0.74), with considerable heterogeneity between studies (I2 = 92%) (Figure 1(c)).
Time to castrate resistance
Two studies reported time to castrate resistance. A meta-analysis using the random-effects model demonstrated no significant difference in this outcome between the two groups (MD = 1.01 months more in the SC group, 95% CI = −0.85 to 2.87, p = 0.29), with considerable heterogeneity between studies (I2 = 95%) (Figure 2(a)).
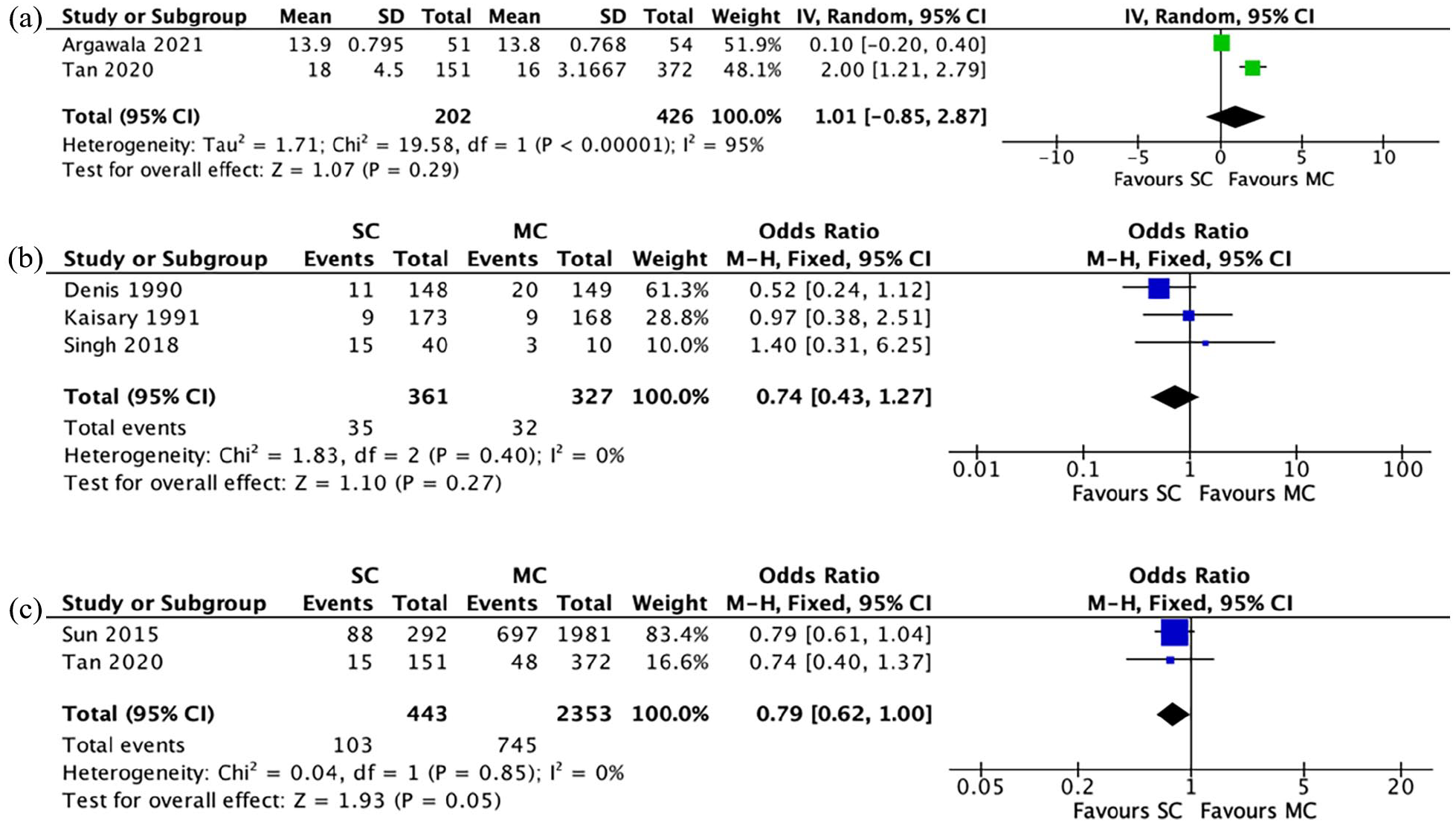
(a)–(c) Meta-analysis results: (a) time to castrate resistance, (b) gynaecomastia and (c) cardiovascular complications.
Gynaecomastia
Three studies reported rates of gynaecomastia in the SC and MC cohorts post-castration. The incidence was 9.7% (n = 35/361) in the SC group and 9.8% (n = 32/327) in the MC group. A meta-analysis using the M-H fixed-effects model demonstrated no significant difference between the two groups in regard to this outcome (OR = 0.74, 95% CI = 0.43 to 1.27, p = 0.27), with no heterogeneity between studies (I2 = 0%) (Figure 2(b)).
Cardiovascular complications
Cardiovascular complications rates were reported in two studies; however, they were not defined by either study. The incidence was 23.3% (n = 103/443) in the SC group and 31.7% (n = 745/2353) in the MC group. A meta-analysis using the M-H fixed-effects model demonstrated a trend towards significance in this outcome between the two groups, in favour of SC (OR = 0.79, 95% CI = 0.62 to 1.00, p = 0.05), with no heterogeneity between studies (I2 = 0%) (Figure 2(c)).
Hot flushes
Three studies reported rates of hot flushes post-castration. The incidence was 62.3% (n = 144/231) in the SC group and 66.7% (n = 140/210) in the MC group. A meta-analysis using the M-H fixed-effects model demonstrated no significant difference between the two groups in regard to this outcome (OR = 0.86, 95% CI = 0.57 to 1.28, p = 0.45), with low heterogeneity between studies (I2 = 25%) (Figure 3(a)).
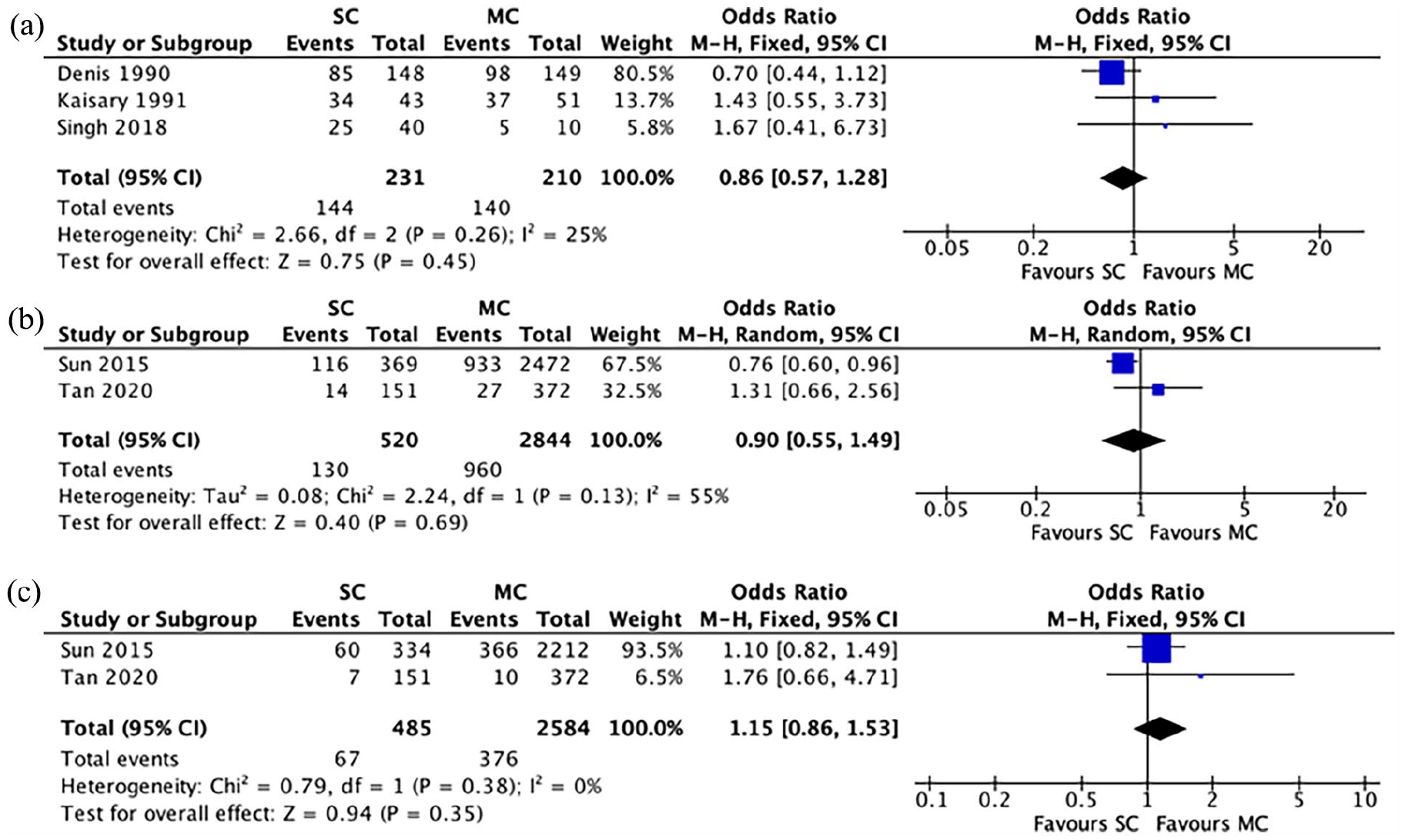
(a)–(c) Meta-analysis results: (a) hot flushes, (b) fractures and (c) new-onset T2DM.
Fractures
The post-castration fracture rate was recorded in two studies. This incidence was 25% (n = 130/520) in the SC group and 33.8% (n = 960/2844) in the MC group. A meta-analysis using the M-H random-effects model demonstrated no significant difference in fracture rate between the two groups (OR = 0.90, 95% CI = 0.55 to 1.49, p = 0.69), with considerable heterogeneity between studies (I2 = 55%) (Figure 3(b)).
New-onset T2DM
Two studies reported rates of new-onset T2DM between the two groups. The incidence was 13.8% (n = 67/485) in the SC group and 14.6% (n = 376/2584) in the MC group. A meta-analysis using the M-H fixed-effects model demonstrated no significant difference in this outcome between the two groups (OR = 1.15, 95% CI = 0.86 to 1.53, p = 0.35), with no heterogeneity reported across the studies (I2 = 0%) (Figure 3(c)).
Discussion
Our results demonstrate a trend towards significance in our primary outcome, overall survival, in favour of SC for metastatic prostate cancer. With the exception of nadir PSA levels post-castration favouring MC, there was no significant difference in other outcomes between the two groups. There was, however, a trend towards significance in overall survival and cardiovascular complications (p = 0.06 and p = 0.05, respectively) in favour of SC. To our knowledge, this is the first meta-analysis providing a comparison between bilateral orchidectomy and GnRH agonists in the treatment of metastatic prostate cancer.
Despite its limited use, SC appears to offer a survival benefit over MC in the treatment of metastatic prostate cancer; however, the reason behind this survival benefit remains unclear. 18 Morgentaler’s saturation model postulates that prostate carcinoma requires a minimal testosterone concentration to thrive. 28 Several studies have suggested that GnRH analogues are inferior to SC in achieving nadir testosterone levels; however, our meta-analysis of comparative studies showed no clear advantage of one modality over another in regard to this outcome.29 –32 Bilateral orchidectomy also offers the advantage of complete cessation of the production of testosterone, whereas GnRH analogues, due to variability in pharmacokinetics from person to person, may allow for a flare in testosterone if the medication becomes ineffective prior to the next dose. 18 Further studies are required to identify which subgroup of patients will benefit most from both SC and MC, from both an oncological and adverse effects perspective.
Unfortunately, due to a lack of available data, we were unable to quantify and meta-analyse several of our primary endpoints: cost of treatment and post-castration QoL. Previous research has suggested a negative psychological impact on physical appearance in patients who underwent bilateral orchidectomy. 33 In reality, where subcapsular orchidectomy is performed, the tunica fills with fluid giving the appearance of small testicles bilaterally. 34 In the setting of a rise in healthcare expenditure, financial burden should be incorporated into the selection of similarly efficacious treatment modalities of long-term androgen suppression. 6 Costs incurred by SC are limited to the procedure itself, anaesthesia, complications of surgery and follow-up care, whereas MC requires years of ongoing expensive medications, administration costs and costs provoked by complications to medical therapy.35,36 SC remains the standard of care in certain populations within Sub-Saharan Africa, primarily due to high costs associated with ADT and lack of funding. 37 Two studies included in our analysis reported a cost comparison between the two cohorts; however, these data were not meta-analysable. Sun et al. 8 found no financial advantage of one treatment modality over another ($9726.98 and $8478.46 in SC and MC groups, respectively); however, this can be attributed to the fact that costs were limited by a 12-month follow-up period and do not account for years of ongoing treatment required by medical androgen deprivation. At a median follow-up of 38.9 months, Tan et al. 3 found a significant financial benefit of SC over MC (SGD$5275 and SGD$9185.80, respectively). More studies are necessary to further quantify the degree of financial benefit incurred by one modality over another in the treatment of this cohort of patients. Similarly, data on patient QoL post-castration is lacking in the literature. More studies, incorporating ideally the same QoL scoring tool and patient-reported outcome measures (PROMs), are required to further identify which patients would be more suited to one method of castration over another.
This meta-analysis has several strengths and serves in providing important evidence which may be utilised to inform future therapeutic decision-making. The data curated in this study provide coherency in relation to outcome measures which in turn may to help counsel patients in accordance with anticipated outcomes and expected adverse effects of both MC and SC. Accordingly these data may improve patient counselling.
Notwithstanding, this study is subject to some inevitable limitations. First, there is but a few studies of prospective, randomised design previously performed on this topic, thus rendering it necessary to rely on studies of moderate quality evidence. Therefore, it is inevitable that results are subject to confounding, ascertainment and selection biases. Studies, which are retrospective in nature, may exhibit selection bias such as the selection of patients who are less comorbid for SC, thus potentially affecting overall survival outcomes for that cohort. Second, the paucity of data reported on treatment cost and QoL limits these data, making it challenging to draw conclusions in relation to these important outcome measures. Finally, the studies included in this study span 31 years (1990–2021) which brings into question the comparability of these data provided. In the wake of the molecular era, it is inevitable that the medical, oncological and surgical management paradigm of these diseases has evolved in accordance with our increased appreciated for the molecular biology underpinning this disease. Thus, comparability of such studies may be questioned. Despite these limitations, this is the first meta-analysis to directly compare outcomes of surgical orchidectomy and GnRH analogues in the treatment of metastatic prostate cancer and provides coherent data illustrating the improved survival outcomes observed following SC.
Conclusion
SC appears to be a safe, feasible and efficacious alternative to MC, with evidence to suggest a potential survival benefit and limited evidence of a financial benefit in the treatment of men with metastatic prostate cancer. Further studies are required to further quantify the financial burden of one method over another, as well as to identify which subgroup of patients respond best to each method of castration.
Supplemental Material
sj-docx-1-uro-10.1177_20514158231212534 – Supplemental material for Surgical versus medical castration in the treatment of metastatic prostate cancer: A systematic review and meta-analysis
Supplemental material, sj-docx-1-uro-10.1177_20514158231212534 for Surgical versus medical castration in the treatment of metastatic prostate cancer: A systematic review and meta-analysis by Niall J O’Sullivan, Hugo C Temperley, Matthew G Davey, Ailish Naughton and Rowan G Casey in Journal of Clinical Urology
Supplemental Material
sj-docx-2-uro-10.1177_20514158231212534 – Supplemental material for Surgical versus medical castration in the treatment of metastatic prostate cancer: A systematic review and meta-analysis
Supplemental material, sj-docx-2-uro-10.1177_20514158231212534 for Surgical versus medical castration in the treatment of metastatic prostate cancer: A systematic review and meta-analysis by Niall J O’Sullivan, Hugo C Temperley, Matthew G Davey, Ailish Naughton and Rowan G Casey in Journal of Clinical Urology
Supplemental Material
sj-docx-3-uro-10.1177_20514158231212534 – Supplemental material for Surgical versus medical castration in the treatment of metastatic prostate cancer: A systematic review and meta-analysis
Supplemental material, sj-docx-3-uro-10.1177_20514158231212534 for Surgical versus medical castration in the treatment of metastatic prostate cancer: A systematic review and meta-analysis by Niall J O’Sullivan, Hugo C Temperley, Matthew G Davey, Ailish Naughton and Rowan G Casey in Journal of Clinical Urology
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Contributorship
N.J.O. and H.C.T. contributed to data extraction. N.J.O. and M.D. contributed to data synthesis. A.N., H.C.T. and R.G.C. contributed to manuscript preparation. N.J.O. contributed to manuscript writing. N.J.O. and R.G.C. contributed to manuscript review/editing.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1975 Helsinki Declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Guarantor
H.C.T.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.